

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Acute herpes zoster results from reactivation of the latent varicella zoster virus in the sensory ganglia of spinal or cranial nerves. Acute herpes zoster is characterized by pain, itching, and sensory changes in the affected dermatomes [1]. Neuraxial intervention treatments such as epidural block, in combination with antiviral therapy, effectively reduce acute pain arising from herpes zoster and prevent postherpetic neuralgia (PHN) [23]. In a recent case, deep cervical plexus block with occipital nerve block was reported to reduce herpes zoster-induced pain [4]. Therefore, peripheral nerve block may be an effective option for the treatment of acute pain arising from herpes zoster.
The superficial cervical plexus (SCP) is derived from the ventral rami of C1–4 spinal nerves. During SCP block (SCPB), the injectate can be spread into the deep cervical plexus [5]. Here, we report a case of a 71-yr-old woman suffering from pain and itching on her right C2–4 dermatomes, arising from herpes zoster, who was successfully treated with SCPB.
CASE REPORT
A 71-yr-old woman who had had a painful herpetic rash on her right cervical 2–4 dermatomes for 16 days was referred to a pain clinic (Fig. 1). Two days after the onset of the rash, a clinical diagnosis of herpes zoster was confirmed by a dermatologist and the patient was prescribed 250 mg famciclovir three times a day for 7 d, pregabalin 150 mg twice a day, and tramadol 150 mg once a day for 14 d. Despite this medication, the patient's pain was rated at an intensity of 6 on the numeric rating scale, ranging from 0 (no pain) to 10 (worst pain imaginable). Additionally, she complained of severe itching in the affected areas.
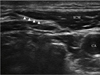
The patient refused cervical epidural block because of the potentially fatal risks, such as epidural hematoma leading to neurological complications. Therefore, SCPB was considered because it is easier and safer than epidural block and the injectate can be spread into the deep cervical plexus. After obtaining written patient consent for the procedure, an ultrasound-guided SCPB was performed (Fig. 2). With the patient in the correct position, the transducer was placed on the lateral neck, overlying the sternoclavicular muscle (SCM) at the level of its midpoint. The needle was then passed through the skin, platysma, and prevertebral fascia. The tip of needle was placed behind the posterior border of the SCM. We injected 0.5% lidocaine 15 ml mixed with triamcinolone 30 mg. Five days after the procedure, the patient's pain and itching completely disappeared. As of now, she has remained symptom-free for 6 months. Consent for publication of this case was obtained from the patient.
DISCUSSION
The majority of herpes zoster cases involve elderly patients [12]. Herpes zoster affects peripheral and/or central nerves, producing pain, itching, and abnormal sensory experiences. PHN is the most common complication associated with herpes zoster. Independent predictors of PHN include old age, severe pain, and more than two affected dermatomes [26]. In this case, a 71-yr-old patient experienced severe herpetic pain on the C2–4 dermatomes.
Early treatment with antiviral drugs can reduce acute pain arising from herpes zoster and prevent PHN [2]. Additionally, in combination with antiviral agent treatment, neuraxial blocks such as interlaminar or transforaminal epidural blocks shorten the duration of herpes zoster pain and reduce the incidence of PHN [237]. However, neuraxial blocks are associated with potentially fatal neurological complications resulting from epidural hematomas [8]. Peripheral nerve block can be utilized when central neuraxial block is contraindicated [4]. Peripheral nerve block with local anesthetics and steroids effectively reduces pain in a nerve injury pain animal model. Administration of steroids around the injured nerve reduces ectopic discharge from damaged neurons and perineural inflammation [910]. Deep cervical plexus block with occipital nerve block has been shown to effectively reduce acute pain arising from herpes zoster on the cervical dermatomes [4]. The SCP has four braches which include the lesser occipital nerve, greater auricular nerve, transverse cutaneous nerve of the neck, and the supraclavicular nerve, that emerge from posterior border of SCM. The SCPB injectate can be spread into the deep cervical plexus [5]. Compared with deep cervical plexus block, SCPB can be easily and safely performed using ultrasound, and it is widely utilized for carotid endarterectomy in awake patients [11]. In addition, SCPB can be an alternative option for general anesthesia in the drainage of submandibular and submental abscesses [12].
In the present case, ultrasound-guided SCPB with a combination of 0.5% lidocaine 15 ml and triamcinolone 30 mg was safely performed and completely alleviated pain and itching arising from herpes zoster.
In conclusion, ultrasound-guided SCPB can be a safe and effective modality for treatment of acute symptoms arising from herpes zoster. Additionally, it can potentially prevent PHN. Further studies investigating the clinical significance of SCPB in the treatment of herpes zoster are required.

 XML Download
XML Download