

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Control of postoperative pain is an important aspect of postoperative patient management. Adequate control of postoperative pain improves respiratory functions, reduces the risk of heart problems, promotes hemodynamic stability, inhibits hormonal and metabolic reactions, improves liver function by allowing for early exercise, and reduces the length of hospitalization by bringing about successful surgical outcomes [12]. One of the most commonly used methods of postoperative pain control is patient-controlled analgesia (PCA) [3]. PCA was first introduced clinically in the late 1960s. By pressing a button on the PCA pump, patients can control the dose and infusion interval according to the level of pain they are experiencing. Pain is commonly controlled by infusing drugs at a fixed rate in clinics. The infusion dose and interval are pre-set by a clinician according to the pharmacokinetics of the drug to prevent excessive infusion [4]. However, when drugs are infused at a fixed rate, patients may experience pain at 1-6 h after the operation, and request for more infusions [56]. And, they may also experience side effects such as nausea, vomiting, dizziness, headache, itching, and dyspnea over time after the operation due to excessive drug administration [78]. By infusing high doses of analgesics to control pain during the early period after the operation, and reducing the doses gradually after a certain period of time, side effects of PCA can be reduced, while patient safety and satisfaction can be increased [9]. A patient-controlled anesthesia device that uses this concept to allow patients to control the infusion rate according to time has recently been developed [10]. In this study, we compared the convenience, safety, and patient satisfaction of two different methods of PCA, which differed by whether the rate of infusion was variable or fixed.
MATERIALS AND METHODS
1. Subjects
This study was approved by the Institutional Review Board of the hospital in which this research took place. Informed consent was obtained from all of the study participants. Patients aged 18-74 years who had previously undergone orthognathic surgery, discectomy, or total hip arthroplasty, who were classified as American Society of Anesthesiologists (ASA) I or II in the physical status classification system developed by the ASA, and who wished to control postoperative pain through PCA were included in this study. However, these patients had: a history of hypersensitivity to drugs; a body mass index (BMI) ≤ 20 or ≥ 30; serious kidney, liver, or cardiac diseases; been taking narcotic analgesics or sedatives for a long time; used drugs or alcohol; or respiratory diseases were excluded. The patients were fully informed about analgesia and pain assessment devices to be used before they underwent the operation.
2. Method
All patients were premedicated with glycopyrrolate 0.2 mg, and monitored using an electrocardiogram, pulse oximetry, noninvasive blood pressure, end-tidal carbon dioxide monitoring device, and bispectral index (BIS). For anesthetic induction, propofol 2 mg/kg and rocuronium bromide 0.6 mg/kg were administered, and intubation was performed. Anesthesia was maintained at BIS ≥ 40 and ≤ 60, and within 20% of the normal blood pressure and pulse using nitrous oxide along with sevoflurane 0.7~1.3 volume% and remifentanil. Then, palonosetron 0.075 mg was administered to prevent postoperative nausea and vomiting. After the operation was completed, all drug administration was stopped, and pyridostigmine 0.2 mg/kg and glycopyrrolate 0.4 mg were administered to reverse muscle relaxation. Extubation was performed after patients opened their eyes and were able to take a deep breath. The patients were moved to the postanesthetic care unit (PACU). Once the patients regained consciousness and began feeling postoperative pain, they were divided into two groups, and their PCA devices were installed.
The patients were randomly assigned into either the control group or the test group. A PCA infuser (Accumate, Wooyoung Medical Corp., Seoul, Korea), which infuses at a fixed rate, was used for the control group, and a PCA infuser (PS-1000, Unimedics Medical Corp., Seoul, Korea), which makes time-scheduled background infusion, was used for the test group. Postoperative pain was controlled using PCA for 48 hours after the operation. Morphine 1 mg/ml was used. In the control group, the background infusion rate was set to 0.5 ml/h for 48 hours. The amount of PCA bolus was set to 1.0 ml and the filling time was set to 15 min so that the patients could self-administer the drug in times of need. In the test group, the background infusion rate was set at 1 ml/h at 0-24 hours after the operation and 0.5 ml/h at 24-48 hours after the operation. The amount of PCA bolus was 1.0 ml and the filling time was 15 min, similar to the control group.
The level of pain was measured on the basis of patients' scores on the visual analogue scale (VAS), which range from 0-10, in the recovery room. PCA devices were connected to the veins of patients who scored 4 or more on the VAS. Patients whose VAS scores were 4 or more even after performing PCA were administered ketorolac 30 mg as a rescue analgesic, and this infusion was recorded.
After the patients were moved to their wards, their VAS scores at 6 h, 24 h, and 48 h after the operation, the number of rescue analgesic injections, side effects (nausea, vomiting, itching, sedation, dyspnea), and satisfaction with analgesia on a scale of five (5 = excellent, 4 = good, 3 = adequate, 2 = poor, 1 = awful) were recorded.
The sample size was calculated with α = 0.05 and β = 0.2 by comparing patient satisfaction and assuming that a mean difference of two or more was clinically meaningful. The calculated sample size was 50 patients in each group. Therefore, this study was conducted with a total of 100 patients.
Statistical analyses were performed with Statistical Package for Social Sciences 17.0 for Windows (SPSS Inc., Chicago, IL, USA). All data were expressed as mean ± standard deviation. A Student's T-test was used to compare the demographic data (not including gender) and doses of morphine infused between the test and the control groups. A Mann-Whitney U-test was performed to compare VAS scores, and a Pearson's Chi-square test or Fisher's exact test was performed to compare the rate of side effects and patient satisfaction. The level of statistical significance was set at P < 0.05.
RESULTS
A total of 100 patients participated in this study. In the control group, three patients dropped out because of intravenous disconnection, and one because of patient rejection, resulting in a total of 46 patients completing the study. In the test group, four patients dropped out due to intravenous disconnection, and four due to patient rejection, resulting in 42 patients completing the study (Fig. 1). No significant differences in the general patient characteristics including age, gender, height, weight, and BMI were found between the two groups (Table 1).
1. Analgesic efficacy
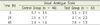
Although a significant decrease in VAS scores over time was observed in both the control and the test groups, no statistically significant difference in the VAS scores of the two groups were found (Table 2). In the comparison of morphine doses, no significant decrease in the dose was observed in the control group in comparison with the test group at 0-24 h after the operation. However, the dose had a statistically significant decrease at 24-48 hours after the operation, and overall in the test group (Table 3).
2. Safety and side effect
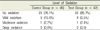
In both groups, nausea and vomiting had the highest frequency of all side effects; no significant difference in the rates of vomiting and nausea was found between the two groups. No significant difference in the rate of using rescue analgesics and itching was found between the two groups. Dyspnea was not observed in both groups (Table 4). No significant difference in the level of sedation was found between the two groups. Deep sedation was not observed in any of the groups (Table 5).
3. Patient satisfaction
Patient satisfaction was higher in the test group than in the control group, but not by a statistically significant difference (Table 6). In both groups, more than 30% of patients expressed dissatisfaction with postoperative analgesia.
DISCUSSION
While patients and clinicians prefer PCA over other methods of postoperative pain control, determination of the type and dose of drugs is still an important point to be considered [7]. Of various kinds of drugs used in intravenous PCA, opiates are the most commonly used analgesics [11]. Major examples of opiates include morphine, fentanyl, alfentanil, and pethidine, whose potency and associated side effects vary. Morphine, the opiate used in this study, is the most commonly used opioid in PCA. Morphine has a slow onset of action because it does not easily cross the blood brain barrier due to its hydrophilic property. Morphine-6-glucuronide (M6G), which is an active metabolite of morphine, can cause pain relief, sedation, and dyspnea, and is excreted through the kidneys [12]. Patients with renal failure must be careful when using morphine [12].
This study investigated the effects of morphine infused at a changing rate on postoperative pain control and patient satisfaction with analgesia. In both groups, pain was reduced over time after the operation, and this reduction was especially significant between at 6 h and 24 h after the operation. This finding was consistent with that of a previous study, which emphasized the need for intensive analgesia at 1-6 h after surgery; this is when pain reaches its maximal point [56]. In this study, morphine was infused at a fixed rate of 0.5 ml/h for 48 hours after the operation in the control group, and at 1 ml/h for 24 hours, and at 0.5 ml/h from 24 to 48 hours after the operation in the test group. Despite the different rates of infusion, the amount of morphine infused at 6 hours after the operation and 24 hours after the operation was similar in both groups. This suggests that the patients in the control group pushed the bolus button more frequently than the patients in the test group because of postoperative pain; this is because early concentrations of analgesics cannot adequately control the level of postoperative pain when infused in small doses at a fixed rate in PCA [1314]. Although morphine was infused at an identical rate of 0.5 ml/h at 24-48 h after the operation in both groups, a higher amount of morphine was used in the control group than the test group during this time interval, and over 48 hours postoperatively. This suggests that the patients in the control group pushed the bolus button more frequently than the patients in the test group 24 hours after the operation. Based on this observation, it appears that the patients in the test group infused themselves with high doses of morphine during the early postoperative period, which led to a rapid rise in the concentration of morphine in the bloodstream, and consequently, analgesic effects, to a point where infusions were no longer requested. The rates of using rescue analgesics due to severe pain after PCA was 17-26%, and no significant difference in the rates was found between the two groups. These findings show that PCA in which the rate of infusion is adjusted during the procedure allows patients to control their pain efficiently with small doses of morphine and without the need to press the bolus button.
Pain control using morphine infusions can result in side effects such as dyspnea, nausea, vomiting, itching, and urinary retention [11]. In this study, nausea was the most common side effect in both groups, and no difference in the rate of nausea was found between the two groups. The rate of nausea in this study was similar to the rates of nausea and vomiting observed in previous studies in which palonosetron was infused for PCA during an operation [915]. Reducing the use of opiates as PCA analgesics adding other types of analgesics or antiemetic drugs can lower the rates of nausea and vomiting [1617]. In addition, although the morphine dose in the test group was twice that in the control group in the first 24 hours after the operation, no difference in the rates of vomiting, itching, and dyspnea, and level of sedation was found between the two groups. This means that side effects occur at the same frequency in the test group, in which morphine was infused at different rates, as in the control group, in which morphine was infused at a fixed rate, and that both methods of IV PCA have the same degree of safety.
In this study, the overall patient satisfaction with postoperative pain control was higher in the test group than the control group, but the difference was not statistically significant. More than thirty percent of all patients reported dissatisfaction with analgesia due to side effects including nausea and vomiting.
In conclusion, PCA adjusted with different infusion rates for different time duration is more efficient and safe for the management of postoperative pain than PCA with infusion of fixed rate.





 XML Download
XML Download