

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
About 2% of patients with colorectal cancer have been reported to experience isolated para-aortic lymph node (PALN) recurrence after curative resection of the primary tumor [1]. The rarity of this condition has limited studies on the treatment of patients with isolated PALN recurrence of colorectal cancer, and there are no established treatment guidelines. Studies on the treatment of tumor recurrence in distant organs, such as the liver and lungs, have shown that surgical resection and chemotherapy (CTx) improve patient prognosis, establishing the role of surgical treatment for liver and lung recurrences [2345]. In addition, studies have compared outcomes of different treatment modalities, such as intensive CTx including target agents and local ablative therapy [6789]. Consensus in treating distant recurrences was largely due to the relatively high incidence of recurrence in the liver and lungs and to technological advances in diagnostic imaging methods for detection of these recurrences [1011].
However, the diagnostic accuracy of imaging modalities for PALN recurrence is limited. A systematic review of the diagnosis of PALN recurrences of cervical cancer have shown that CT and MRI each have a sensitivity of 60% and a specificity of 90% [12], and several studies in colorectal cancer have found that imaging modalities have a similar or even lower accuracy, with a sensitivity of 77% and a specificity of 71% [1314]. By contrast, imaging modalities have a specificity of about 90% in diagnosing liver/lung metastases of colorectal cancer [151617]. Assessing treatment outcomes in patients with PALN recurrence diagnosed by imaging modalities may be erroneous. Rather, pathologic confirmation of recurrent disease after surgical resection may assist in treatment planning.
Several case reports and a retrospective study have indicated that surgical resection is beneficial for patients with PALN recurrence [118]. One study reported, however, that outcomes of chemoradiotherapy (CRT) and surgical resection were similar in patients with recurrent rectal cancer [19]. To date, however, there is insufficient evidence to establish guidelines for the treatment of PALN metastases. The present study, therefore, investigated the effects of different treatments on oncologic outcomes in patients with PALN recurrence of colorectal cancer, as well as analyzing the course of disease in patients who underwent surgical resection for this condition.
Go to : 
METHODS
Patients
The study population consisted of consecutive patients who were diagnosed with isolated PALN recurrence after curative resection for primary colorectal cancer from January 2004 to December 2015 at Asan Medical Center, Seoul, Korea. The medical charts of these patients were reviewed, and survival outcomes, clinicopathological characteristics of the primary colorectal cancers, perioperative treatment, characteristics of PALN recurrence, treatment for recurrence, and treatment for rerecurrence were recorded retrospectively. The study protocol was approved by the Institutional Review Board (IRB) of Asan Medical Center (IRB No. 2019-1128), which waived the requirement for informed consent due to the retrospective nature of the study.
Of 176 patients with initial recurrence at distant lymph nodes, 46 experienced recurrence only in para-aortic regions. Distant lymph nodes were defined as lymph nodes located outside the regional drainage of the primary tumor, including PALNs, external iliac and common iliac lymph nodes, and other extra-abdominal lymph nodes.
PALN recurrence was defined as recurrence in lymph nodes surrounding the abdominal aorta and inferior vena cava, extending laterally to the edge of the psoas major muscles, cranially to the crus of the diaphragm, and caudally to the midpoint of the common iliac vessels. CT, MRI, and PET findings indicative of recurrence were integrated to confirm recurrence. A short axis diameter >8 mm on CT or MRI was considered highly indicative of recurrence. Visible lymph nodes <8 mm accompanied by high uptake on PET or high serum CEA concentrations were also suspected of being recurrences.
Resectability was assessed by a multidisciplinary team, consisting of expert colorectal surgeons, gastrointestinal oncologists, radiation oncologist, and gastrointestinal radiologists. Patients with a single isolated PALN recurrence or multiple PALNs forming a single cluster were considered resectable (Fig. 1). By contrast, multiple PALNs scattered on both sides of the aorta and recurrences invading adjacent major vessels, such as the celiac trunk or superior mesenteric artery, were considered unresectable. The sizes and locations of recurrent PALNs were determined by reviewing images. Node location was classified as above renal vessels, below renal vessels, and to the left and right of the aorta.
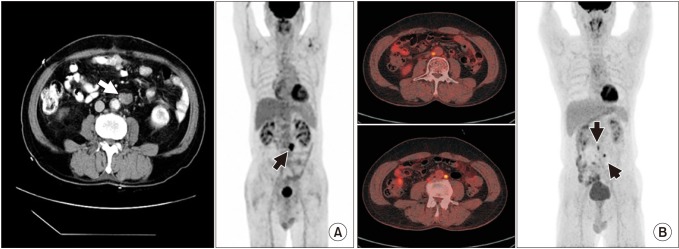 | Fig. 1(A) CT image and PET image of patient number 5 (Table 5). Short axis diameter of 17 mm, single cluster recurrent paraaortic lymph node (PALN) in CT image (white arrow), and correlating single high standard uptake value in PET image (black arrow) indicates possibility of resection. (B) CT and PET images of an unresectable patient. Multiple PALN between aorta and inferior vena cava with additional lymph nodes below kidney level shown in CT image (yellow uptake), with correlating multiple scattered high standard uptake value shown in PET image.Table 5Recurrence pattern and disease course of patients who underwent resection for recurrent para-aortic lymph node (PALN)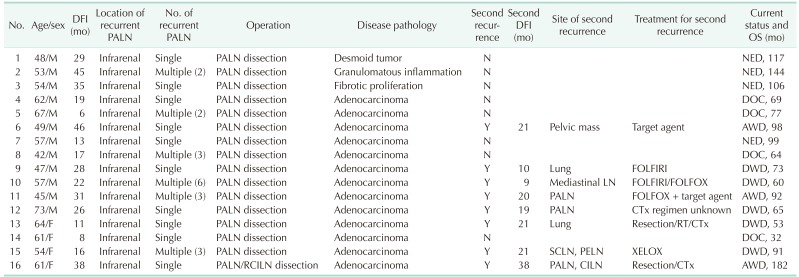 DFI, disease free interval; OS, overall survival; NED, no evidence of disease; DOC, dead of other cause; AWD, alive with disease; FOLFIRI, folinic acid, fluorouracil, and irinotecan; DWD, dead with disease; LN, lymph node; FOLFOX, folinic acid, fluorouracil, and oxaliplatin; PELN, para-esophageal LN; SCLN, supraclavicular LN; CILN, common iliac LN; Y, yes; N, no; RT, radiotherapy; CTx, chemotherapy.
|
Treatment of recurred PALN
Treatments for PALN recurrence included surgical resection with curative intent, CTx, and radiotherapy (RT), with the decision on treatment modality made by a multidisciplinary team, in consultation with individual patients. Surgical resection with curative intent consisted of wide excision of the lymph node and invaded adjacent tissue, including normal tissue, to secure clear resection margins. All patients who underwent surgical resection received adjuvant CTx. RT consisted of a standard total radiation dose of 48–55.4 Gy in 25–31 fraction. Three patients received RT as salvage treatment, and 7 patients received RT as either definitive treatment or for postoperative concurrent CRT. The decision on whether to treat patients with RT was made by a multidisciplinary team including a radiation oncologist. All patients treated with RT received either neoadjuvant or adjuvant CTx. Patients pathologically confirmed as having nonrecurrence after resection of isolated PALNs did not receive further treatment.
Statistical analysis
The primary outcomes were survival after recurrence (SAR) and overall survival (OS). SAR was defined as the interval from the first identified recurrence to death from any cause. OS was defined as the interval from the operation date of primary tumor to death from any cause. Categorical variables were analyzed using chi-square test. Continuous variables were expressed as mean standard deviation and compared using the Student t-test.
SAR and OS were estimated using the Kaplan-Meier method and compared by the log-rank test. Multivariable analysis with a Cox proportional hazards model was used to compare correlations of risk factors and primary outcomes. Number of PALN, disease-free interval (DFI), pN status, lymphovascular invasion (LVI), perineural invasion (PNI), and resection for recurrent PALN was included in the multivariable analysis. Patients with incomplete data were included in the analysis. All statistical analyses were performed using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA), with P < 0.05 considered statistically significant.
Go to :
RESULTS
Clinicopathological characteristics of patients and primary tumors
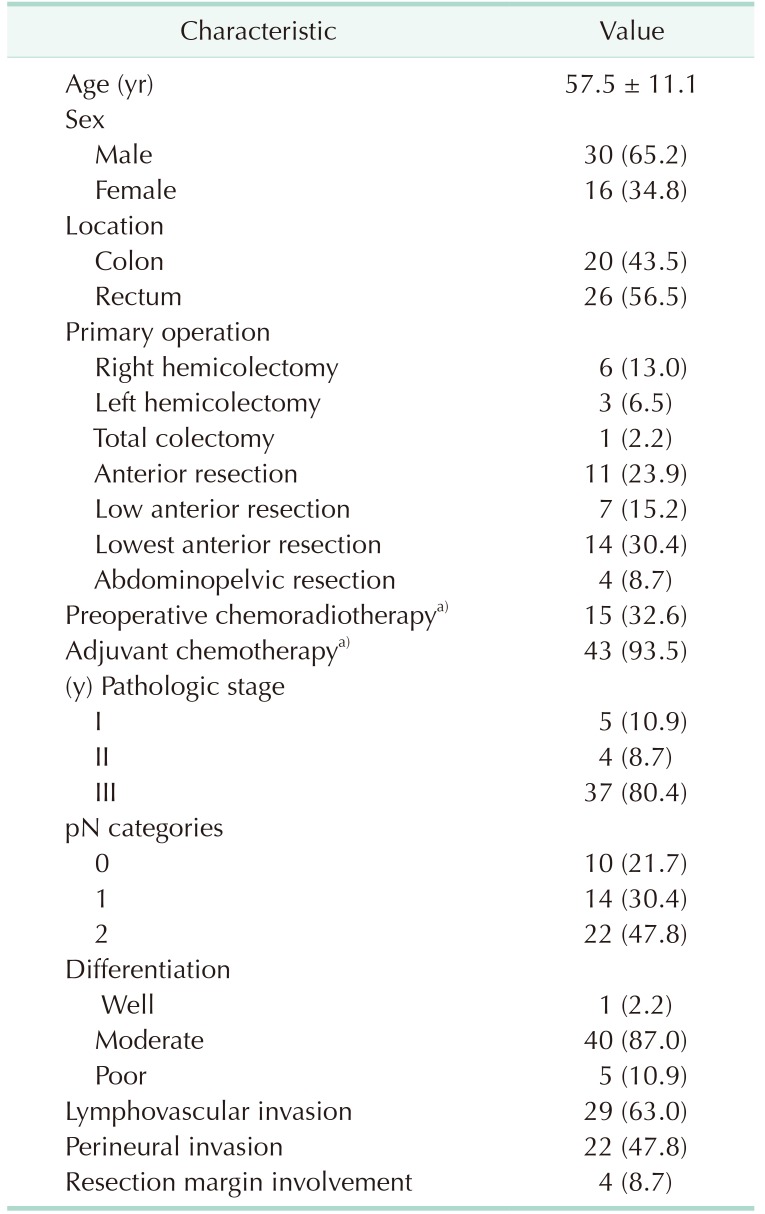
Of the 46 patients with PALN recurrence, 30 (65.2%) were men. These patients had 46 primary tumors, 20 (43.5%) located in the colon and 26 (56.5%) in the rectum. At diagnosis, 37 patients (80.4%) had stage III primary tumors, with 40 (87.0%) having moderately differentiated tumors. Node metastasis was observed in 36 patients (78.3%). Fifteen patients (32.6%) were treated with preoperative CRT and 43 patients (93.5%) received postoperative adjuvant CTx after resection of primary tumor. Pathologic results are depicted in Table 1. The median follow-up time was 50 months (interquartile range, 30–72 months).
Characteristics of PALN recurrence
Median time to PALN recurrence was 19 months, with 41 of the recurrent PALNs (89.1%) located below the renal vessels. Twenty-eight patients (60.9%) experienced multiple recurrences, and the median diameter of the largest LN measured in CT images was 17 mm. Of the 46 patients with PALN recurrences, 35 (76.1%) were classified as resectable. Sixteen patients (34.8%) underwent resection of the recurred PALNs; of these, 3 patients (18.8%) were found to have been misdiagnosed following pathologic examination, with one each found to have a desmoid tumor, chronic granulomatous inflammation, and fibrotic proliferation. These patients received no further treatment, but were followed up regularly (Table 2). Following resection, the median size of the largest LN was 19 mm compared with 17 mm by preoperation imaging. Of the 22 patients (47.8%) treated with CTx alone, 9 were treated with FOLFIRI (folinic acid, fluorouracil, and irinotecan), 2 with FOLFOX (folinic acid, fluorouracil, and oxaliplatin), 5 with XELOX (capecitabine and oxaliplatin), one with LF (folinic acid and fluorouracil), 2 with oral capecitabine, and 2 with targeted agents alone (pembrolizumab and avastin). The treatment regimen could not be determined in 1 patient, who received CTx at a different hospital. Among the 6 patients treated with CTx + RT, salvage RT was administered to 3 patients and definitive RT was given to 3 patients. FOLFIRI was given to 4 patients and XELOX was given to 2 patients.
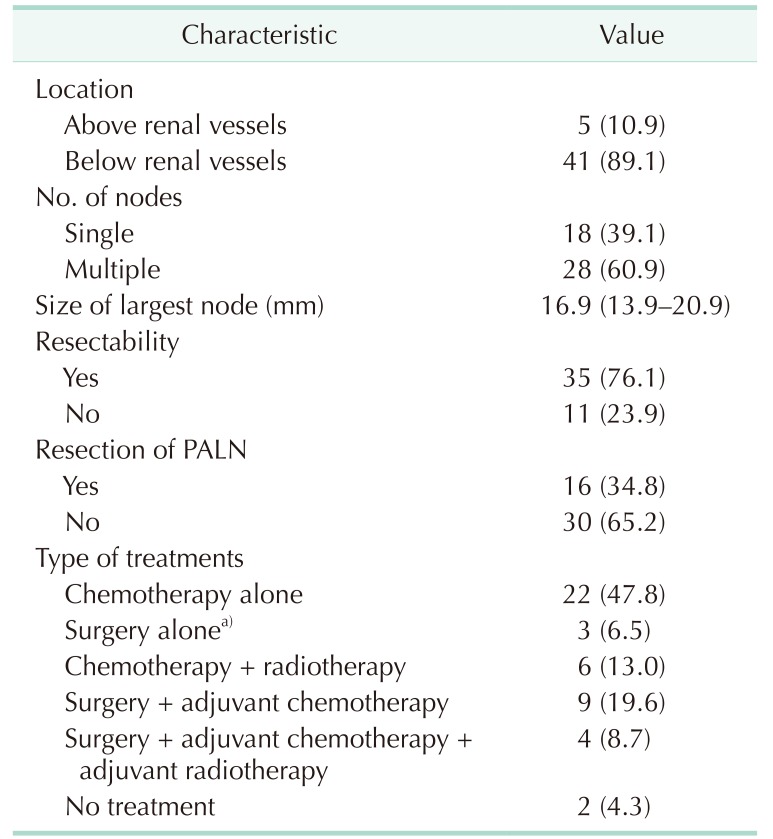
Of the 2 patients who did not receive any treatment, one, who was recommended to undergo CTx, refused treatment. The reason the second patient was not treated was not recorded.
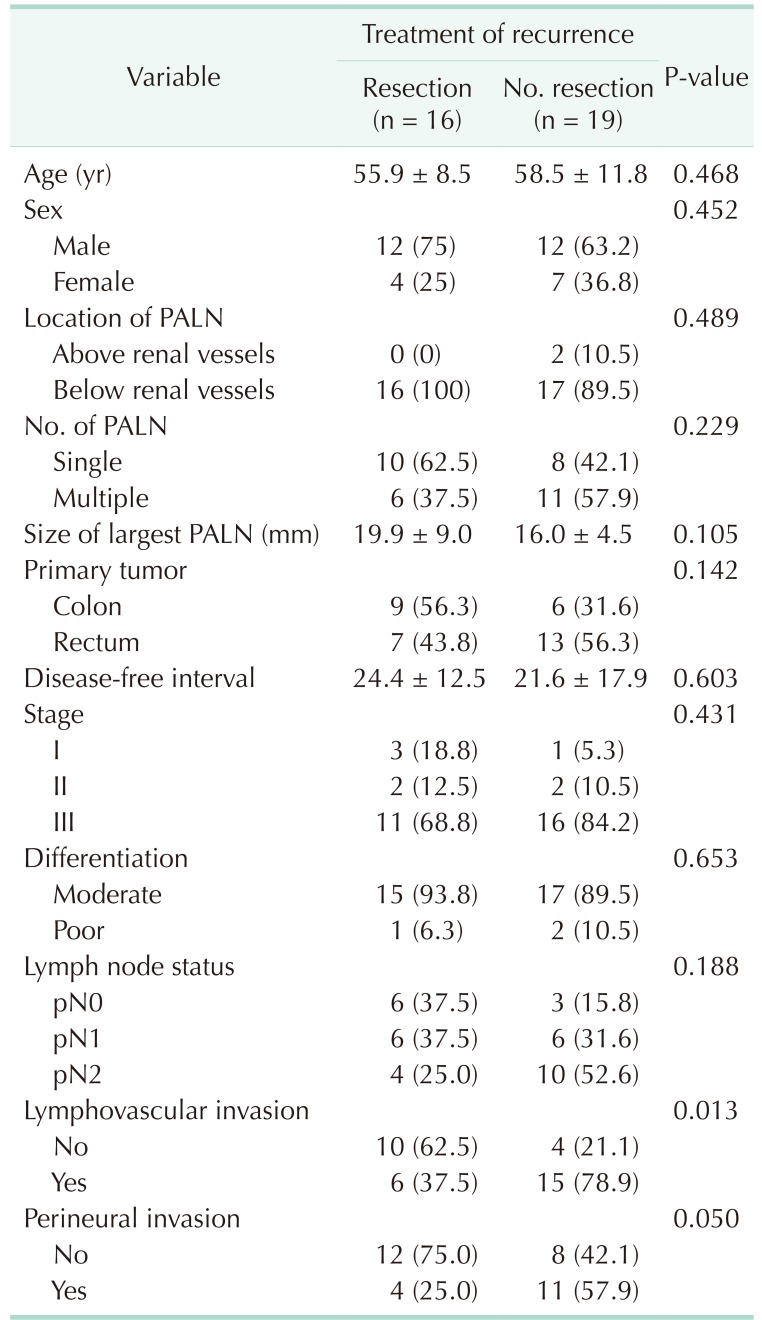
Generally, the demographic and clinical characteristics of patients between who did and did not undergo resection for recurrent PALN were similar. However, the rates of LVI (P = 0.013) and PNI (P = 0.050) of the primary tumor were significantly lower in patients who did than did not undergo PALN resection (Table 3).
Survival outcomes and factors related to prognosis
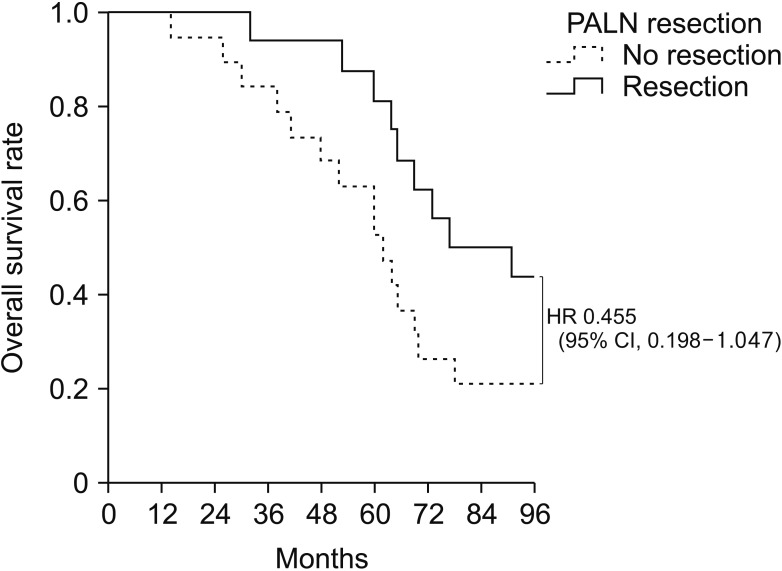
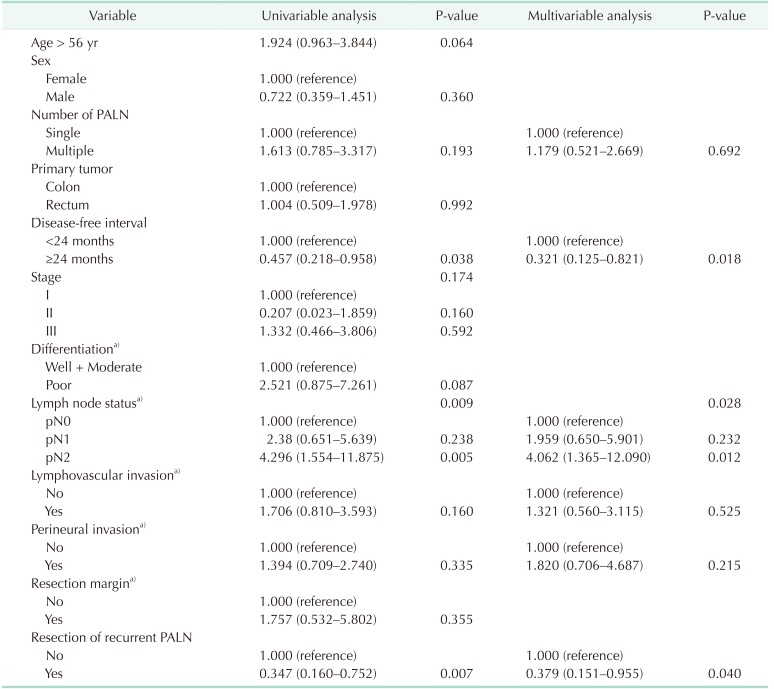
The 46 patients had a median OS of 64 months. Among the 35 patients with resectable PALN recurrence, SAR was significantly longer in patients who did than did not undergo PALN resection (71 months vs. 39 months, P = 0.017) (Fig. 2). OS also tended to be longer in patients who did than did not undergo PALN resection (77 months vs. 62 months, P = 0.055) (Fig. 3). Multivariable analysis showed that factors independently associated with SAR included DFI >24 months, less advanced pN stage of the primary tumor, and resection of PALN recurrence (Table 4).
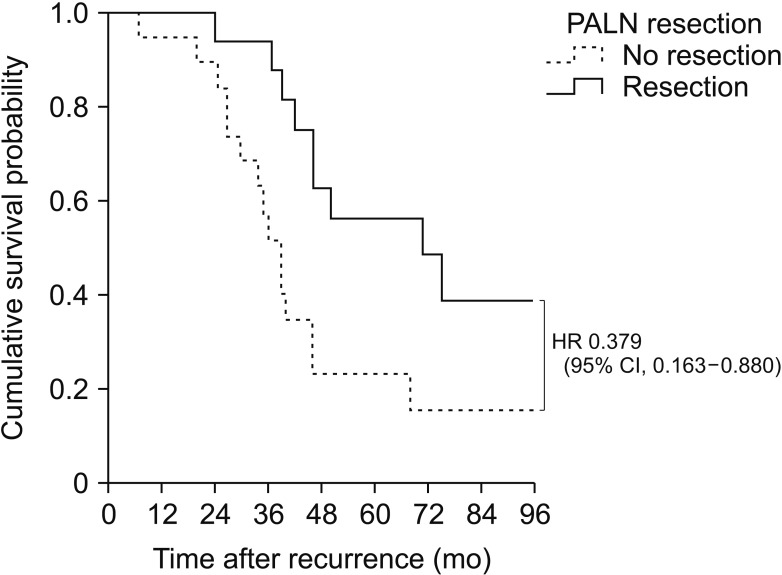 | Fig. 2Kaplan-Meier analysis of survival after recurrence rates in patients who did and did not undergo resection for resectable recurrent para-aortic lymph node (PALN) (n = 35). Survival after recurrence rate was higher in the resected group, with a hazard ratio (HR) of 0.379. CI, confidence interval.
|
Eight patients with recurrent PALN experienced secondary recurrence, 5 at distant lymph nodes, including PALN and mediastinal, supraclavicular, and common iliac lymph nodes; 2 in the lungs; and 1 in the pelvis (Table 5). Of the patients without secondary recurrence, 4 showed no evidence of disease at regular follow ups and 4 died of unknown causes.
Go to :
DISCUSSION
The present study showed that prognosis was better among patients who did than did not undergo surgical resection of recurrent isolated PALNs. SAR was significantly longer and OS tended to be longer in patients who underwent resection. These findings are in agreement with those of a previous study showing the benefits of surgical resection for isolated PALN recurrences [1], providing further evidence for the efficacy of surgical treatments.
Surgical resection for isolated PALN recurrence may benefit patients in many ways. Other than enhancing survival, as shown in the present study, surgical resection enables pathologic confirmation of recurrence in a disease difficult to diagnose definitively by imaging modalities alone, such as CT, MRI, and PET. Of the 16 patients who underwent surgical resection for recurrent isolated PALN, 3 were confirmed on postoperative histologic examination to have benign disease. The misdiagnosis rate was approximately 20%, similar to those in radiologic studies [121314]. These 3 rediagnosed patients were able to avoid unnecessary additional adjuvant treatments and only required regular check-ups. Similarly, 20% of the patients who did not undergo surgical resection may also have been misdiagnosed with recurrences, receiving CTx unnecessarily. The median OS of the 3 patients with confirmed lack of recurrence was 117 months, better than 95% central range of all patients. Therefore, it is reasonable to question the patients with outlying prolonged survival rates without pathologic confirmation (Table 5).
Although 8 of the 16 patients (50%) who underwent resection for isolated PALN recurrence responded to treatment, with no evidence of disease progression, only 4 of 19 patients (21%) who did not undergo surgical resection responded to treatment. Fourteen patients (73.7%) presented with disease progression to distant organs, such as the livers, lung, distant LNs, and bone. Time to PALN metastasis was similar in the 2 groups (22 months vs. 18 months, P = 0.331), suggesting that metastasis to distant organs may result from unresected PALN metastasis.
DFI and pathologic N stage of primary tumor were significant prognostic factors for survival outcome, but did not differ in patients who did and did not undergo the resection. The relationships between DFI and survival outcomes are not clear. For example, one study reported no relationship between DFI and survival outcome [1], whereas another study reported that DFI > 24 months was a positive predictor of outcome, a result similar to ours [20]. Further research is needed to verify whether DFI is a prognostic predictor in these patients. Other factors, such as number of PALNs, primary tumor location, LVI, PNI, and resection margins, were not prognostic of survival in the present study.
Patients with liver/lung metastases of colorectal cancer frequently receive local treatments, such as radiofrequency ablation (RFA), RT, and surgical resection. Local treatment modalities, such as RFA and RT, have shown survival outcomes comparable to surgical resection in carefully selected patients with liver and lung metastases [212223]. To date, however, few studies have assessed the efficacy of local therapy in the treatment of PALN. Survival outcomes in patients with isolated retroperitoneal LN recurrence were reported following CRT and surgical resection. The median OS in 22 patients who underwent curative CRT was 41 months [19], similar to the median OS of 40 months in 25 patients who underwent surgical resection [20]. In the present study, median SAR was 34 months in the 6 patients who received CRT and 46 months in the 10 patients who received neoadjuvant CTx followed by resection (P = 0.146). Median SAR was comparable in patients treated with CTx alone (36 months, P = 0.230). However, because imaging tools alone have a high false positive rate, patients may receive unnecessary treatment, with oncologic outcomes including patients falsely diagnosed with recurrence. Nevertheless, local treatments for PALN recurrences show favorable oncologic outcomes in selected patients, with more research needed to establish clinically applicable treatment indications.
The present study had several limitations due to its retrospective design. Although group characteristics and medical records were as complete as possible, the data may not be comprehensive. The decision to resect recurrent isolated PALN was dependent on individual surgeons. Over the last decade, however, a multidisciplinary team, consisting of oncologists, surgeons, and radiologists, has made decisions on patient treatment, making these treatments more consistent. Another limitation was the relatively small number of patients included in the present study. Direct comparison of the 2 groups of resected and nonresected patients may not have been appropriate, inasmuch as patients who did not undergo resection were likely to have more aggressive tumors or be in poorer general condition. Nevertheless, tracking disease progression and response to different treatment modalities were possible.
In conclusion, this study indicates that surgical resection has advantages in patients with resectable PALN recurrence. Pathologic confirmation of the recurrence can alter treatment. Larger studies comparing patients who have received different treatments and with longer follow-up times are needed to determine optimal treatments for these patients.
Go to :
 XML Download
XML Download