

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Among the primary carcinomas in the liver, intrahepatic cholangiocarcinoma (IHCC) is the second most common cancer after hepatocellular carcinoma (HCC), and the incidence is increasing worldwide [12]. However, the volume of literature on IHCC is scarce compared to that for the widely studied HCC [34]. Only 10%–20% of IHCCs are deemed resectable at the time of presentation [5], and the median survival time ranges from 6–9 months for patients with unresectable disease [6]. It is generally believed that IHCC is primarily a surgical disease, and surgical resection offers the only prospect for long-term survival [7]. Unfortunately, even after curative-intent surgery, the clinical outcomes of patients undergoing liver resection are disappointing, with a 5-year survival rate of 20% to 35% [8]. Furthermore, the efficacy of adjuvant therapies, including systemic chemotherapy and radiotherapy, is poorly understood, and there are no standard criteria [9]. Many factors have been found to predict prognosis after surgical resection for IHCC, but a consensus has not yet been reached regarding the factors that could significantly and independently influence the survival rates [101112]. Furthermore, because of the low survival rate of IHCC patients who undergo surgical treatment, it may be difficult to accurately assess the prognostic factors of long-term survival. Therefore, the purpose of this study is to identify the prognostic factors of IHCC, analyze the patients who have survived for more than 10 years after surgery, and to identify the prognostic factors associated with long-term survival in such patients.
Go to : 
METHODS
Data sources and study population
From January 2003 to December 2012, 429 single-institution patients who underwent hepatic resection for pathologically proven IHCC at Asan Medical Center were enrolled in this study. The cohort of patients did not have metastatic lesions at the time of diagnosis and had no preoperative chemotherapy; subsequently, they underwent hepatic resection for therapeutic purposes and achieved R0 or R1 resection. Preoperative variables included age, sex, underlying liver cirrhosis, serum CA 19-9 levels, and antigens of Clonorchis sinensis. All patients underwent preoperative contrast-enhanced CT or magnetic resonance imaging (MRI) of the chest and abdomen. A biopsy was not routinely performed before surgery. Pathological data for tumors were examined, including data on size, number of tumors, the grade of differentiation, presence and extent of vascular invasion, perineural invasion (PNI), and lymph node (LN) metastases. Margin and nodal status were identified based on the final pathologic review by a dedicated pathologist. The tumors were staged using the TNM classification, and the patients were regularly followed up after surgery. CT or MRI was used to monitor the abdomen and chest radiographs prospectively for up to 2 years every 3–4 months, and every 6 months for up to 5 years, after which the surveillance was performed annually. The date of the last follow-up, vital status, and recurrence-related information was collected for all patients, with recurrence defined as histologically confirmed or strongly-suspected recurrence in imaging studies. Additionally, the duration from the initial date of surgery to the development of recurrent disease was recorded. Data collection and analysis were performed according to the institutional guidelines, which conformed to the ethical standards of the Declaration of Helsinki. This retrospective study was approved by the Institutional Review Board of Asan Medical Center (No. S2019-0525). Patient informed consent was waived because of the retrospective nature of the study.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA). Summary statistics were obtained using established methods and presented as percentages, mean, or median values. Recurrence and survival curves were estimated by the Kaplan-Meier method. Predictive analysis of variables associated with the factor-specific hazard of recurrence and survival was performed using the multivariate Cox proportional hazard model. Hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated. All reported P-values were two-sided, and P < 0.05 was considered statistically significant.
Go to :
RESULTS
Baseline characteristics
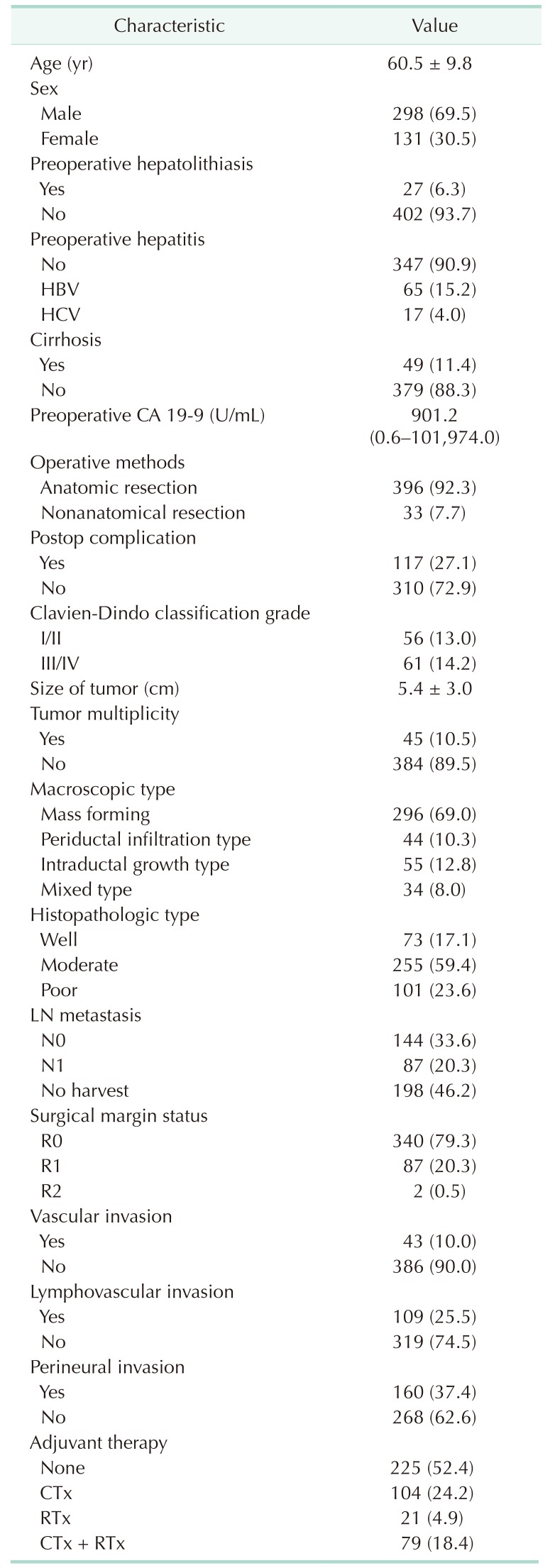
The clinicopathologic characteristics of patients in this study are shown in Table 1. In the cohort, the median age was 60.5 years (range, 31–83 years) and males were dominant (69.5%). Preoperatively, 27 patients (6.3%) had intrahepatic cholangitis, and 65 (15.2%) and 17 patients (4.0%) had HBV and HCV infection, respectively. Additionally, 49 patients (11.4%) had preoperative cirrhosis, and 204 patients (47.6%) had high preoperative CA 19-9. Subsequently, anatomical resection was performed on 92.3% patients, and R0 resection was performed on 79.3% of patients. Laparoscopic surgery was performed in 7 patients: 5 laparoscopic left lateral sectionectomy, 1 laparoscopic S6 monosegmentectomy, and 1 laparoscopic S6 partial hepatectomy. Postoperative complications occurred in 27.1% patients and Clavien-Dindo classification grade III/IV complications were noted in 14.2%. According to postoperative clinico-pathological factors and patient conditions, 204 patients (47.6%) underwent adjuvant chemo-radiation therapy.
Pathological report
The average tumor size was 5.42 cm, and 10.5% had more than one tumor. On macroscopy, the mass-forming type was the most common in 296 patients (69.0%), followed by the intraductal growth type (12.8%), and periductal infiltrating type (10.3%). Furthermore, the histopathologic analysis revealed that moderate differentiation was the most prevalent (n = 255 [59.4%]) among patients, while 10% had a vascular invasion, 25% had LVI, and 37% had PNI.
Risk factor analysis for patient survival and tumor recurrence
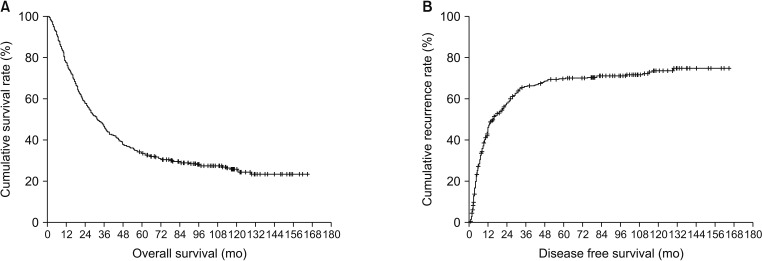
The overall 1-, 3-, and 5-year survival rates of patients were 76.5%, 44.1%, and 33.3%, respectively, while the disease-free 1-, 3-, and 5-year survival rates were 51.1%, 31.0%, and 28.3%, respectively (Fig. 1). Multivariate analysis showed that high CA 19-9 (≥38 U/mL) (HR, 2.191; 95% CI, 1.601–2.998; P < 0.001), LN metastasis (HR, 1.750; 95% CI, 1.281–2.391; P = 0.001), and LVI (HR, 1.519; 95% CI, 1.097–2.104; P = 0.012) were independent factors associated with overall survival. Of these, high CA 19-9 (≥38 U/mL) (HR, 1.549; 95% CI, 1.126–2.133; P = 0.007) and LN metastasis (HR, 1.426; 95% CI, 1.022–1.990; P = 0.037) were also analyzed as independent factors affecting recurrence; additionally, adjuvant therapy (HR, 1.743; 95% CI, 1.242–2.447; P = 0.001) was another independent factor that affected recurrence (Table 2).

Comparison of clinicopathologic data between patients who survived ≥10 and <10 years
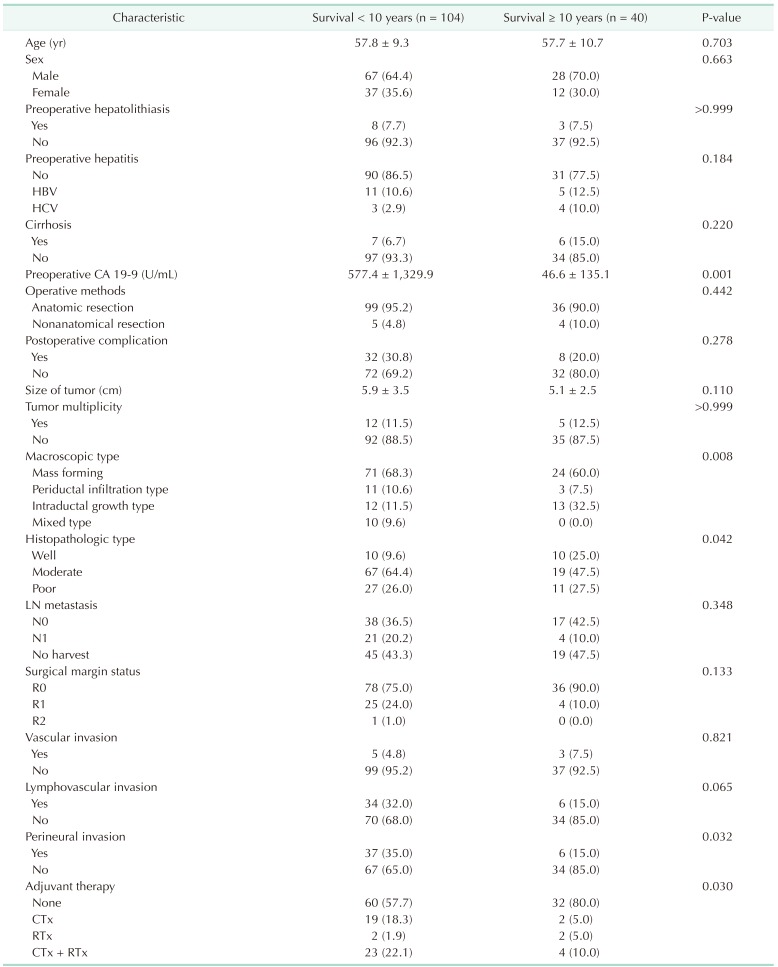
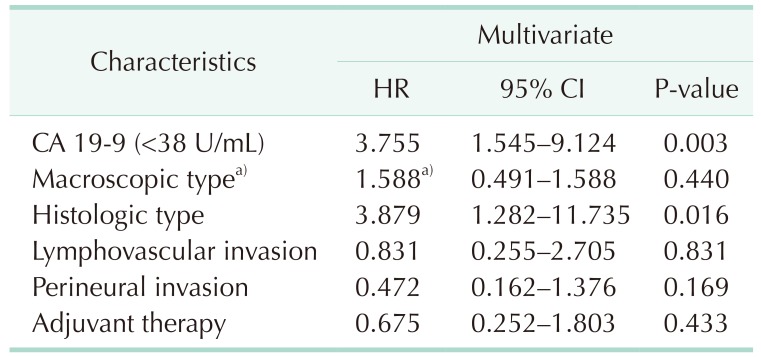
The results of the univariate analysis of patients who survived for over 10 years and less than 10 years are demonstrated in Table 3. Lower levels of CA 19-9 (<38 U/mL) were more frequently observed in patients who survived for more than 10 years (P = 0.001). Additionally, the prevalence macroscopic type (P = 0.008), histological type (P = 0.042), LVI (P = 0.040), PNI (P = 0.032), and adjuvant therapy (P = 0.030) were statistically different between both groups. Multivariate analysis also showed that low CA 19-9 (<38 U/mL) (HR, 3.755; 95% CI, 1.545–9.124; P = 0.003) and well-differentiated types (HR, 3.879; 95% CI, 1.282–11.735) were independent factors affecting the ≥10-year survival rates (Fig. 2).
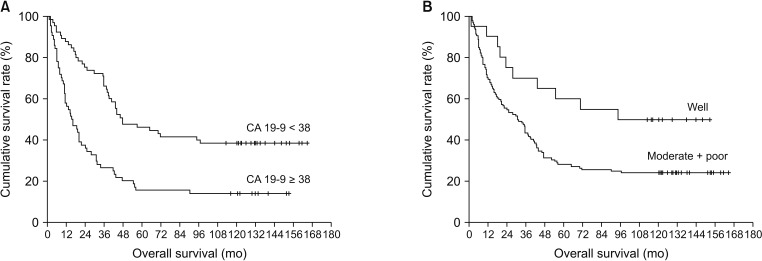 | Fig. 2(A) The results of Kaplan-Meier analysis of patients who survived over 10 years and below 10 years according to the CA 19-9 level. (B) The results of Kaplan-Meier analysis of patients who survived over 10 years and below 10 years according to the histopathological type.
|
Comparison of clinicopathologic data between patients who survived >5 and <1 year
Of the patients who died within 1 year (group 1) and those who survived for more than 5 years (group 2), the proportions of each of the following factors showed significant differences in univariable analysis: (1) CA 19-9 > 38 U/mL (group 1: 74.7% vs. group 2: 34.7%, P = 0.001), (2) tumor size > 5 cm (group 1: 57.7% vs. group 2: 43.0%, P = 0.035), (3) intraductal growth type (group 1: 3.1% vs. group 2: 22.4%, P = 0.001), (4) well differentiation type (group 1: 6.2% vs. group 2: 27.1%, P = 0.003), (5) PNI (group 1: 54.2% vs. group 2: 19.6%; P < 0.001), (6) vascular invasion (group 1: 76.2% vs. group 2: 4.7%, P < 0.001), (7) LN metastasis (group 1: 52.5% vs. group 2: 16.7%; P < 0.001).
Go to :
DISCUSSION
It is widely acknowledged that the curative treatment of IHCC is surgical resection. Despite the surgical advances and risk factors for IHCC, the clinical outcome after resection is still dismal [1314]. Consequently, the 5-year survival rate in our institution was 33.3%, which was comparable to the previously reported survival rates [11131516]. Although several studies have analyzed 5-year survival rates and recurrence rates, few studies have investigated the long-term survival for more than 10 years. This may be related to the low 5-year survival rate, and thus, the assumption that a small number of patients would survive for more than 10 years. To the best of our knowledge, only one retrospective single-institution study reported the results of an actual 10-year survival analysis [17]. Si et al. reported that 21 out of the 251 patients (8.4%) included in their study survived for more than 10 years; however, this value is not negligible. However, they also analyzed the clinicopathologic characteristics of patients who survived for more than 10 years and found that the prevalence of the following factors was higher in this cohort: time for the first recurrence, lower levels of alkaline phosphatase, tumor markers such as CEA and CA 19-9, single tumor, and smaller tumor size. However, due to the small sample size, they did not obtain statistically string evidence that the factors mentioned above could affect long-term survival. In this study, 40 patients (25.1%) survived for more than 10 years after surgical resection, which is higher than the rate in the above-mentioned study. Multivariate analysis demonstrated that low levels of CA 19-9 (<38 U/mL) and well-differentiated histologic types were predictors of survival for more than 10 years (Table 4). Among these factors, CA 19-9 is an easily and objectively measurable laboratory finding before surgery. These findings suggest that CA 19-9 may be used as a basis for the application of policies that consider more active surgical treatment in patients with low CA 19-9. In addition to curative resection in patients with high-level CA 19-9, further studies of adjuvant treatment may be needed to improve the poor survival rates.
Furthermore, LN metastasis appeared to be an independent factor affecting both survival and recurrence in this study. In a recently published meta-analysis, this has been shown to be the strongest predictor of survival (HR, 2.09; 95% CI, 1.80–2.43; P < 0.001) [18]. The results were based on 5 previously published studies with the largest cohort. In only 2 of the 5 studies mentioned above, the frequencies of lymphadenectomy were described as 55.2% and 72.1%, respectively [811]. In these studies, LN metastasis was found in more than one-quarter of all patients undergoing LN dissection. Conversely, we performed lymphadenectomy in more than half of the patients, with one-third of these patients presenting with metastatic LN, which is comparable to the previous 2 studies. These results indicate that LN metastasis was found in at least 30% of patients who underwent lymphadenectomy, and this should not be ignored. Furthermore, LN metastasis is essential for accurate staging and subsequent prognosis prediction. Therefore, routine lymphadenectomy of IHCC should be considered. However, since this analysis is derived from a retrospective study, it is necessary to verify this proposal through a randomized control study.
One of the interesting findings of this study is that LVI is an independent prognostic factor for survival. In fact, LVI has been reported to be associated with LN metastasis in breast cancer [19], endometrial cancer [20], and colon cancer [21]. It has also been identified as an independent risk factor for survival in urinary tract carcinoma [2223]. In a previous multi-institutional analysis of IHCC, LVI proved to be an indicator of poor tumor biology and was suggested for use as a screening criterion for adjuvant treatment [24]. Although the oncologic effect of the adjuvant treatment was not statistically analyzed in this study, it is meaningful that the concept of LVI is applied to patients who undergo surgical treatment for IHCC. Therefore, future studies will need to demonstrate that adjuvant treatment can achieve a good oncologic outcome in patients with LVI.
There are several limitations to this study. First, by analyzing cohorts collected over a long period of time, it is possible that changes in surgical methods or treatment policies may have introduced some bias. Second, we did not routinely perform lymphadenectomy, and therefore, the influence of LN metastasis may have been reduced, which may have influenced multivariate analysis of risk factors. Additionally, the extent of lymphadenectomy may be determined by the subjective judgment of the surgeon. Finally, contrary to our expectation, adjuvant treatment appears to be a factor that increased the recurrence rate. This may be attributed to the limitations inherent to retrospective studies, and may also result from the more aggressive adjuvant treatment that is applied to patients with advanced-stage tumor or poor tumor biology. In the future, large-scale prospective studies should be conducted to establish a more detailed guideline to decide if adjuvant treatment should be recommended.
In conclusion, an elevated level of CA 19-9 (≥38 U/mL), LN metastasis, and LVI were identified as independent risk factors for survival after resection of IHCC. Furthermore, CA 19-9 (<38 U/mL) and the histologic type were independent factors predicting the survival for more than 10 years. Despite the poor outcome of surgical treatment for IHCC, patients with these factors are expected to survive for a relatively long time and they should be actively considered for surgical treatment.
Go to :
 XML Download
XML Download