

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is characterized by irreversible airway obstruction, and the worldwide mortality and prevalence of the condition is increasing.1 It has been predicted that by 2030 COPD will have the 5th highest disease burden and 3rd highest mortality rate.23 Chronic inflammation represents the major pathogenesis of COPD and involves the actions of neutrophils, macrophages, lymphocytes, and various cytokines. Oxidative stress also contributes to chronic inflammation through the production of reactive oxygen and nitrogen species.45
Uric acid is the final oxidation product of purine metabolism. It is a proinflammatory substance and is also a powerful endogenous radical scavenger and antioxidant.67 Various studies have demonstrated the association between serum uric acid and systemic inflammation; however, the results vary depending on the disease in question. Hyperuricemia lowers the risk of Parkinson's disease and multiple sclerosis and shows a protective effect in stroke and spinal cord injury.68910 However, hyperuricemia increases the risk of cardiovascular disease, cancer, and kidney disease.111213 There is currently no consensus on the normal range for uric acid; it has been suggested that the upper limit of the normal range should be < 7.0 mg for men and < 6.0 mg for women, but other studies recommend levels of < 6.0 mg, which represents a target of gout treatment for both gender.141516
In patients with COPD, smoking causes inflammation and oxidative stress, which leads to tissue damage and reduced lung function. A previous report has demonstrated the proinflammatory function and antioxidant effect of serum uric acid in the context of COPD.17 Recent studies have revealed elevated uric acid to be an independent predictor of mortality, and this parameter is associated with a higher risk of acute exacerbation of COPD.1819 However, these studies were conducted in patients who were admitted for acute exacerbation of COPD, and there is a paucity of research into the significance of serum uric acid levels in patients with stable COPD. Therefore, we investigated hyperuricemia-related factors and the effect of hyperuricemia on long-term outcomes in patients with stable COPD.
METHODS
Study population and design
We recruited men with COPD from the Korea Obstructive Lung Disease (KOLD) cohort. Details of the design of the KOLD cohort and related research results are described elsewhere.20 All the subjects were determined to have stable COPD and were recruited from pulmonary clinics across 16 hospitals in Korea from June 2005 to June 2015. The inclusion criteria were as follows: 1) Diagnosis of COPD based on irreversible airflow limitation (post-bronchodilator forced expiratory volume 1 second [FEV1]/forced vital capacity [FVC] ratio < 0.7); 2) smoking history of > 10 pack-years, 3) age ≥ 40 years, and 4) availability of serum uric acid data at baseline. Exclusion criteria were: 1) Acute exacerbation of COPD, 2) lower respiratory infection within the 8 weeks before initial screening for enrolment, or 3) presence of other pulmonary diseases including asthma or requirement of oxygen therapy. Our analysis was based on the initial data of the KOLD (including age, gender, body mass index [BMI], St. George's respiratory questionnaire [SGRQ], Charlson comorbidity score, and smoking habits), laboratory findings (white blood cell count, neutrophil, lymphocyte, eosinophil, neutrophil–lymphocyte ratio [NLR], uric acid, creatinine, and protein), and lung function (FEV1, FVC, 6 minute walking distance [6MWD], diffusion capacity of the lungs for carbon monoxide [DLCO], and degree of dyspnea [modified Medical Research Council, mMRC]).
We examined underlying diseases and medications of all subjects. Hyperuricemia was defined as a serum uric acid level of > 7.0 mg/dL. All subjects were observed from the date of first registration to the final follow-up or death. To analyze the effect on mortality and acute exacerbation, all-cause mortality at the time of the last observation and time to first exacerbation were evaluated. Additionally, we investigated clinical factors that may be associated with serum uric acid levels in patients with COPD.
Statistical analysis
Continuous variable data are expressed as mean ± standard deviation for normally distributed values and as median (interquartile range) for skewed variables. χ2 and unpaired t-tests were used to perform intergroup comparisons. Correlations were analyzed using Spearman's rank correlation coefficient to determine significant factors associated with uric acid levels. For analysis of mortality risk factors, the hazard ratio (HR) with 95% confidence interval (CI) was calculated as the relative risk of all-cause mortality. Cox regression models of univariate and multivariate analyses were used to evaluate the effect of hyperuricemia on all-cause mortality and acute exacerbation in patients with stable COPD. The covariates used to calculate HR and Spearman's rank correlation coefficient were age, BMI, comorbidities, laboratory findings, and lung function. Kaplan-Meier survival curves were generated and log-rank tests were performed to evaluate the impact of hyperuricemia on all-cause mortality and time to first exacerbation. All statistical analyses were performed using R software version 3.2.2 (R foundation for Statistical Computing, Vienna, Austria), and P values < 0.05 were considered statistically significant.21
RESULTS
We recruited 251 patients from the KOLD cohort. After the application of inclusion and exclusion criteria, 1 patient was excluded due to goat and 4 due to chronic kidney disease as these conditions could affect serum uric acid levels. A total of 246 cases met the criteria, 6 of which were women. This number of women would not provide a representative dataset for the population of women with COPD; therefore, we excluded women and a total of 240 men with stable COPD were finally enrolled. The mean age of subjects was 66.4 ± 7.7 years, and the median follow-up time was 5.9 years. Table 1 shows the baseline demographic characteristics of the study population according to serum uric acid levels. Compared with nonhyperuricemia, patients with hyperuricemia exhibited an increased prevalence of hypertension (hyperuricemia, 48.9% vs. nonhyperuricemia, 30.6%; P = 0.027). There were no significant differences in lung function or laboratory findings between the groups.
Table 1
Baseline demographic data and results of lung function and laboratory tests for the study population
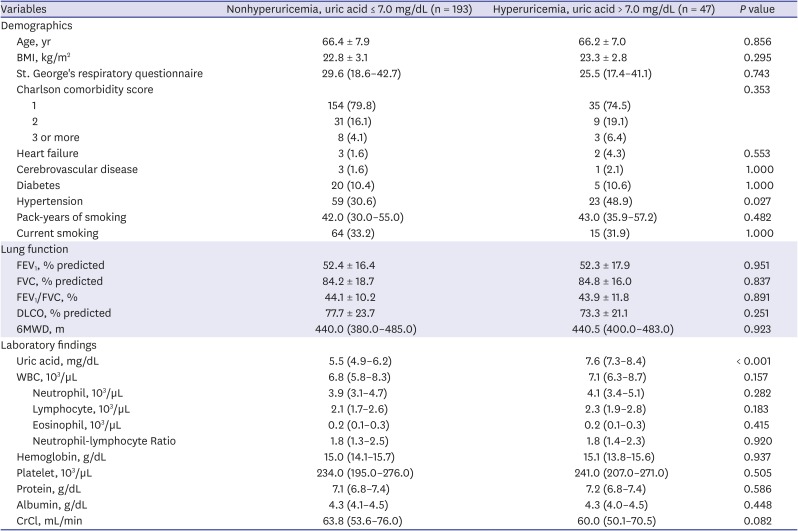
Continuous data are presented as mean ± standard deviation or median (interquartile range), categorical data as numbers (%).
BMI = body mass index, mMRC = modified medical research council dyspnea scale, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, DLCO = diffusing capacity of the lung for carbon monoxide, 6MWD = 6-minute walk distance, WBC = white blood cell, CrCl = Creatinine clearance estimate by the Cockcroft-Gault Equation.
Association between serum uric acid levels and potential confounders
Table 2 shows the results of Spearman's rank correlation coefficient analysis for serum uric acid level according to demographic factors, laboratory findings, and pulmonary function test results. Uric acid level was found to be positively correlated with BMI and serum protein and negatively correlated with NLR. These confounders were statistically significant but rather weak.
Table 2
Association of serum uric acid level with clinical cofounders
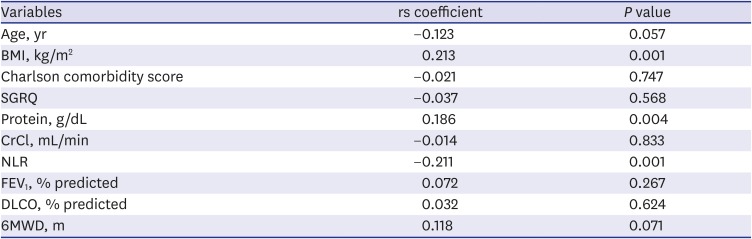
rs = Spearman's rank correlation coefficient, BMI = body mass index, SGRQ = St. George's Respiratory, CrCl = creatinine clearance estimate by Cockcroft-Gault Equation, NLR = neutrophil-lymphocyte ratio, FEV1 = forced expiratory volume in 1 second, DLCO = diffusing capacity of the lung for carbon monoxide, 6MWD = 6-minute walk distance.
Relationship of hyperuricemia with mortality and acute exacerbation
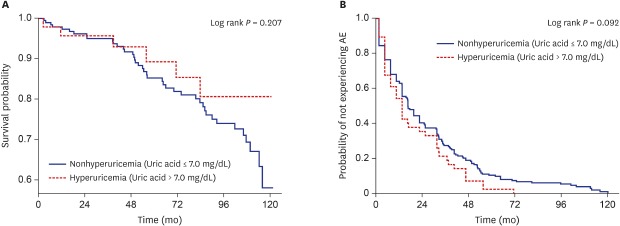
The Kaplan–Meier survival curve revealed no statistically significant differences between the 2 groups in terms of all-cause mortality (P = 0.207) (Fig. 1A) and time to first exacerbation (P = 0.092) (Fig. 1B) in men with stable COPD. In the univariate Cox regression model, hyperuricemia was not associated with an increased risk of all-cause mortality (HR, 0.580; 95% CI, 0.250–1.370; P = 0.213). In the multivariate Cox regression model, old age, low BMI, and low DLCO were associated with a higher risk of mortality (Table 3). In the multivariate Cox regression model, hyperuricemia was not an independent predictor of acute exacerbation (HR, 1.383; 95% CI, 0.977–1.959; P = 0.068). Old age, high SGRQ score, and low FEV1 were associated with a higher risk of acute exacerbation (Table 4).
Fig. 1
Comparison of survival and time to first exacerbation curves according to uric acid level.
Kaplan–Meier survival curves assessing the influence of hyperuricemia on (A) overall mortality and (B) time to first exacerbation in patients with stable chronic obstructive pulmonary disease. P value from log-rank test.
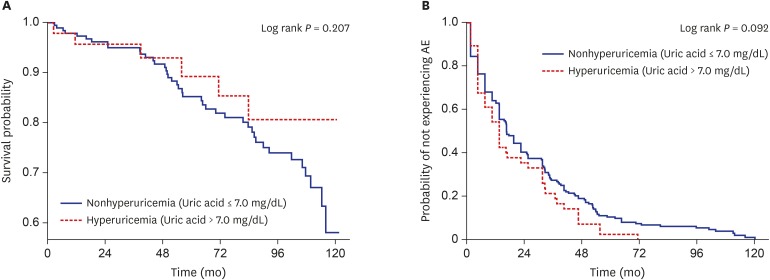
Table 3
Risk factors for mortality by Cox proportional hazards model
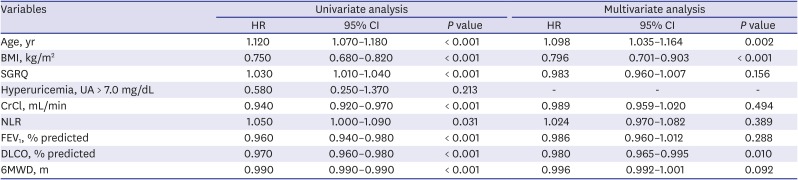
Cox proportional hazard analysis was used to identify independent risk factors for mortality.
HR = hazard ratio, CI = confidence interval, BMI = body mass index, SGRQ = St. George's Respiratory Questionnaire, UA = uric acid, CrCl = creatinine clearance estimate by the Cockcroft-Gault Equation, NLR = neutrophil–lymphocyte ratio, FEV1 = forced expiratory volume in 1 second, DLCO = diffusing capacity of the lung for carbon monoxide, 6MWD = 6-minute walk distance.
Table 4
Risk factors for acute exacerbation of chronic obstructive pulmonary disease by Cox proportional hazards model
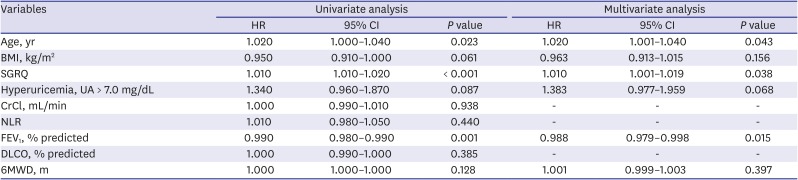
Cox proportional hazard analysis was used to identify independent risk factors for mortality.
HR = hazard ratio, CI = confidence interval, BMI = body mass index, SGRQ = St. George's Respiratory Questionnaire, UA = uric acid, CrCl = Creatinine clearance estimate by the Cockcroft-Gault Equation, NLR = neutrophil–lymphocyte ration, FEV1 = forced expiratory volume in 1 second, DLCO = diffusing capacity of the lung for carbon monoxide, 6MWD = 6-minute walk distance.
DISCUSSION
To the best of our knowledge, this is the first study to evaluate the influence of hyperuricemia on long-term outcomes in men with stable COPD. We investigated clinical factors that may be associated with serum uric acid levels and the effect of hyperuricemia on all-cause mortality and acute exacerbation in this population. Serum uric acid level was found to be negatively associated with systemic inflammation, defined by the neutrophil–lymphocyte ratio. Cox regression analysis showed that hyperuricemia was not associated with increased risk of mortality. Age, BMI, and DLCO, which were previously known as risk factors, were identified as risk factors for mortality. Hyperuricemia was not found to be an independent predictor for acute exacerbation.
Chronic inflammation is an important factor in the pathophysiology of COPD. Although various cytokines and mechanisms have been investigated, the exact mechanism of the development of systemic inflammation in the context of COPD remains unclear.22 Systemic inflammation increases with disease progression and can lead to various comorbidities such as cerebrovascular disease and osteoporosis.23 Uric acid is a powerful scavenger of reactive oxygen species that removes > 60% of the systemic reactive oxygen species7. Although hyperuricemia can act as an anti-inflammatory factor, it can also act as a proinflammatory factor. Thus, the role of hyperuricemia in systemic inflammation remains controversial. In patients admitted with acute exacerbation of COPD, hyperuricemia has been shown to be an independent predictor of mortality and to be associated with a higher risk of acute exacerbation at the 1-year follow-up.1819 However, these studies only evaluated short-term outcomes of limited sample sizes of patients with acute exacerbation.
During acute exacerbation of COPD, serum uric acid has been shown to be elevated, in line with other inflammatory markers, and to induce a proinflammatory effect. However, the cause-effect relationship between serum uric acid and inflammation in patients with COPD remains to be established. The NLR has been identified as an important biomarker of systemic inflammation in the context of COPD and can predict COPD progression as well as outcomes.24 This marker exhibits a similar pattern as systemic inflammation, in that it is increased in the case of COPD compared with the general population, and increases further with disease progression.25 Therefore, if uric acid does indeed act as a proinflammatory factor, NLR should increase with increasing serum uric acid levels. However, we observed a negative correlation between serum uric acid levels and NLR, with no significant difference in NLR between the groups. This discrepancy with the literature indicates that uric acid is not a proper predictor of long-term outcome in stable patients with COPD. Uric acid might, therefore, play a different role in stable COPD. The precise mechanism underlying the association of uric acid and systemic inflammation in stable COPD is not yet known. Further studies are required to explore this.
High uric acid has been shown to be a predictor of mortality and future exacerbations in patients with acute exacerbation of COPD.1819 However, in the present study, we did not identify any associations of hyperuricemia with mortality or future acute exacerbation among stable men with COPD, nor did we find a statistically significant association of uric acid with SGRQ, FEV1, DLCO, or 6MWD, which are long-term prognostic factors of COPD.262728 This demonstrates that uric acid is not an adequate biomarker in the context of stable COPD. Previous studies have also failed to demonstrate consistent results regarding the association of serum uric acid with respiratory symptoms and lung function in the case of stable COPD or in the general population. A cross-sectional study of 367 smokers with COPD and 136 smokers with normal lung function showed lower serum uric acid to be associated with a greater severity of COPD.29 Conversely, the Copenhagen City Heart Study and Copenhagen General Population Study of 1,14,979 individuals revealed high plasma urate to be associated with decreased lung function and increased risk of respiratory symptoms and COPD.30 Together, these studies reveal that there is no consensus on the utility of serum uric acid level as a prognostic marker for patients with stable COPD and that hyperuricemia may not be predictive of long-term outcome.
In patients with COPD, uric acid levels are influenced by various factors, such as age, BMI, alcohol consumption, and nutritional status.31 In the present study, we found BMI to be associated with serum uric acid level and to be an independent predictor of all-cause mortality. Interestingly, hyperuricemia did not show any statistically significant association with either mortality or risk of future acute exacerbation. Table 2 details the correlations of serum uric acid level with clinical cofounders; those which have statistical significance show rather weak correlation, suggesting that serum uric acid is influenced by various conditions. Thus, serum uric acid levels exhibit different trends according to disease and clinical status. Serum uric acid does not, therefore, appear to be a reliable biomarker in patients with stable COPD.
The present study has some limitations which should be mentioned. First, this was a retrospective cohort study and the inherent limitation of this should be considered in the interpretation of results. Additionally, our findings cannot be generalized to all patients with stable COPD due to the all-men population and exclusion of subjects without baseline data of serum uric acid at the time of enrolment. Second, we excluded patients who were previously diagnosed with gout or chronic kidney disease. However, we could not exclude all patients with factors that may affect serum uric acid levels, such as alcohol consumption, poor diet, and high fructose intake. Third, the present study used NLR as a single indicator of systemic inflammation; thus, this may represent a limitation in the precise assessment of inflammation. However, NLR has proven to be an important inflammatory marker in the context of COPD and has been shown to be positively correlated with other systemic inflammatory markers such as C-reactive protein and interleukin-6.32
In conclusion, among men with stable COPD, serum uric acid level is negatively associated with systemic inflammation. Hyperuricemia is not an independent predictor of all-cause mortality or future acute exacerbation of COPD in this population. These results contradict those of previous studies on patients with acute exacerbation of COPD.
 XML Download
XML Download