

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Vitamin D deficiency is currently recognized as a worldwide epidemic.12 Because vitamin D deficiency has been linked with various non-musculoskeletal diseases (including several cancers, cardiovascular disease, and infectious or autoimmune diseases) as well as musculoskeletal disease (including rickets, osteopenia, and osteoporosis),2 maintaining sufficient vitamin D levels is an important health issue.
While the ideal concentration of vitamin D for maintaining optimal health depends on the endpoint,3 numerous clinical guidelines target serum 25-hydroxyvitamin D (25[OH]D) concentrations of 20 ng/mL and have recommended vitamin D supplement doses of 400–800 IU/day in order to reach this target.4 Sunlight is a key factor that determines vitamin D levels5 and is estimated to generate the equivalent of around 2,000 IU of vitamin D when a fair-skinned individual is exposed to 20–30 minutes of sunlight on the face and forearms during midday. Repeating this sunlight exposure 2–3 times a week is sufficient to maintain adequate vitamin D levels in the UK during summer months.67
However, there is no clear evidence on whether the current guidelines for sunlight exposure are optimal for persons with vitamin D deficiency or insufficiency. Some clinical studies have failed to observe a meaningful increase in serum 25(OH)D levels after sunlight exposure,89 while others reported a significant increase.1011 Furthermore, there are only a small number of randomized controlled trials on sunlight exposure,81011 probably due to ethical issues with knowingly exposing subjects to harmful ultraviolet (UV) radiation. Additionally, few clinical trials have compared the effect of sunlight exposure and vitamin D supplementation on vitamin D levels.1011 Therefore, this study was performed to evaluate the effectiveness of sun exposure and vitamin D supplements on serum vitamin D levels among Koreans with vitamin D insufficiency or deficiency.
METHODS
Study design
This study was designed as a randomized clinical trial without blinding. Eligible participants were randomly assigned to one of three parallel arms: daily living, sunlight exposure, and vitamin D supplementation groups. Allocation ratio by group was 1:1:1. The intervention was administered for 4 weeks, from July 2016 to August 2016, corresponding to the summer months in Korea.
Study participants
Study participants were recruited through advertisements in Kyungpook National University, Daegu, Korea from April 2016 to June 2016. The eligibility criteria were individuals aged 20–49 years with serum 25(OH)D levels < 20 ng/mL at the time of screening. The exclusion criteria were currently taking vitamin D supplements for the prevention or treatment of vitamin D deficiency, contraindications for vitamin D supplementation (e.g., nephrolithiasis), sensitivity to sunlight exposure, diagnosed uncontrolled endocrine disease or malignancy, and pregnancy.
Interventions
Stratified simple randomization was used and the stratification variables were gender (men or women) and age group (20–29, 30–39, and 40–49 years old). A project investigator generated the random allocation sequence using an Excel program, and a researcher enrolled participants and assigned participants to each intervention.
1) The daily living group maintained a usual daily life pattern without any intervention for 1 month. Recommendations were made to increase sunscreen use and wear covering clothing to block sunlight as much as possible. 2) The sunlight exposure group received sun exposure at least 3 times a week during daylight (between 10:00 A.M. and 3:00 P.M.) on 20%–30% of their body surface area for about 30 minutes per session as described in guidelines for vitamin D deficiency.1213 Participants were recommended to expose as much body surface area as possible with at least hands, arms, and legs exposed, while protecting the eyes, face, and neck. 3) Vitamin D supplementation group were administered 600–800 IU/day of vitamin D supplements taken orally with meals according to the recommendations of the US Institute of Medicine14 and UK National Health Service.12 Use of sunscreen and wearing covering clothing were recommended to block as much sunlight as possible.
Data collection and measurements
Questionnaire surveys and blood sampling were conducted at baseline and at the 4th week follow-up visit. The questionnaire was administered by trained interviewers, and included demographic and socioeconomic characteristics, health behaviors, and medical history. Participants were asked to keep a diary to track time spent outdoors every day, in order to estimate sunlight exposure, and frequency of dietary intake of vitamin D-rich foods (including salmon, mackerel, tuna, shiitake mushrooms, milk, eggs, and cereals). In the sunlight exposure group, good compliance was defined as sun exposure for more than 12 days over the 4-week study period according to the protocol.
Height and weight were measured in the standing position with only light clothes and without shoes. Body mass index (BMI, kg/m2) was calculated as weight divided by height squared. Venous blood was collected after an overnight fast of at least 8 hours. Parathyroid hormone (PTH) level was measured by ECLIA (Cobas 8000 e602; Roche, Germany). Serum 25(OH)D was analyzed by CLIA (Unicel DXI, Beckman, Brea, CA, USA). Serum 1,25-dihydroxyvitamin D3 (1,25[OH]2D) was analyzed by radioimmunoassay (Dream Gamma-10; Shin-Jin Medics, Goyang, Korea).
Outcomes
The primary study endpoint was the change in serum 25(OH)D levels over the intervention period across the three groups. In addition to this, we also evaluated changes in serum 1,25(OH)2D and PTH levels.
Sample size estimation
The following formula was used to calculate the sample size in each group:

n, sample size per group; δ, difference between mean change in experimental group and mean change in control group; s, standard deviation of outcome variable.
Assuming a between-group 25(OH)D difference of 10 ng/mL, standard deviation of 10 ng/mL, α-level of 0.05 for a two-tailed test, power of 80%, and lost to follow-up rate of 20%, 20 participants were required for each group.
Statistical analysis
Differences of general and clinical characteristics among the three groups at baseline were tested using Kruskal-Wallis test for continuous variables and χ2 test or Fisher's exact test for categorical variables. Differences of outcome variables between baseline and follow-up were tested using the Wilcoxon signed-rank test. All analyses were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). A P value of less than 0.05 was considered statistically significant.
Ethics statement
The study protocol was reviewed and approved by the Institutional Review Board of Kyungpook National University (KNU 2016-0049) and registered with the Clinical Research Information Service in Korea (KCT0002671). Written informed consent was obtained from all study participants after full explanation of the purpose and nature of all procedures. All study participants who completed the intervention received a financial incentive, equal to approximately 90 USD.
RESULTS
General and clinical characteristics at baseline
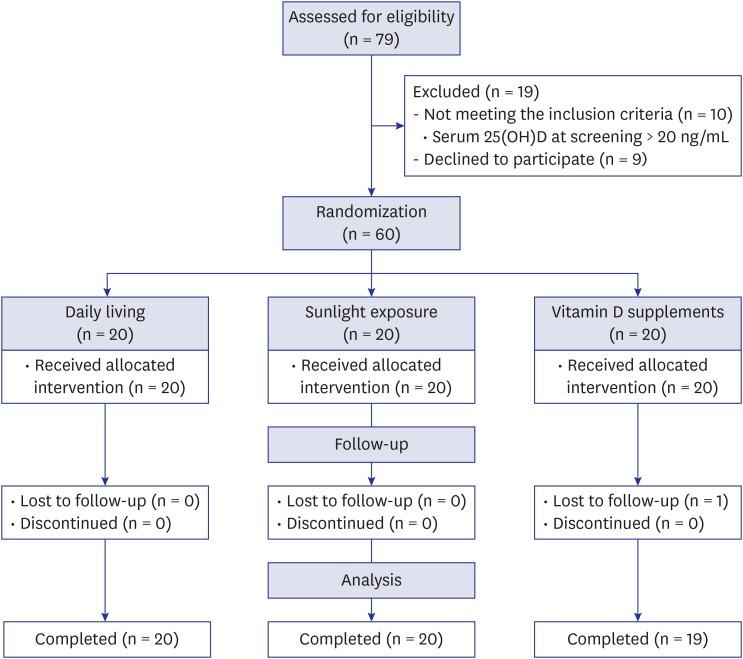
Twenty participants were initially allocated to each group. After excluding participants who were lost to follow up (n = 1), participants who completed the intervention of daily living, sunlight exposure, and vitamin D supplementation were 20, 20, and 19, respectively (Fig. 1).
Fig. 1
Flow chart of the allocation and intervention used in this study.
25(OH)D = 25-hydroxyvitamin D.
The baseline characteristics of participants (n = 59, 31 men and 28 women) are shown in Table 1. The median age was 33 years old with median BMI of 23.2 kg/m2. Among participants, the education level was higher than a college degree in 81.4%, 32.2% were current smokers, and 20.3% were physically inactive. Median time spent outdoors on weekdays and weekends was 0.8 and 1.5 hours/day, respectively. There were no statistically significant differences in gender, age, education level, smoking status, physical activity level, BMI, time spent outdoors on weekdays or weekends, frequency of dietary intake of vitamin D-rich foods, or sunscreen use among the three intervention groups. Serum 25(OH)D, 1,25(OH)2D, and PTH at baseline were not statistically different among the three groups. There were 9 participants (4 in the daily living group, 3 in the sunlight exposure group, and 2 in the vitamin D supplementation group) who had serum concentrations of 25(OH)D < 20 ng/mL during the screening test, but ≥ 20 ng/mL at baseline examination.
Table 1
Baseline characteristics of study participants
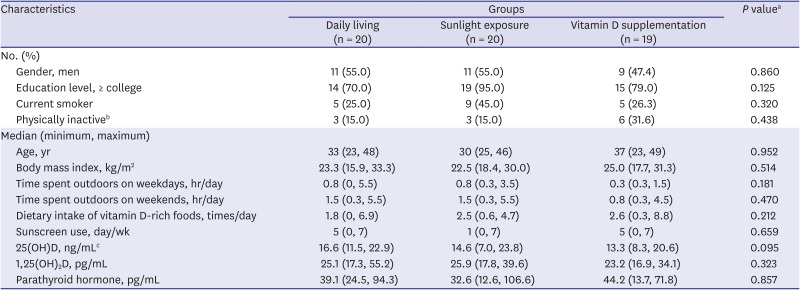
Missing values were substituted by the median value of each variable: the numbers of missing were n = 1 for education; n = 2 for outdoor activity.
25(OH)D = 25-hydroxyvitamin D, 1,25(OH)2D = 1,25-dihydroxyvitamin D3.
aP value for between-group differences were calculated by Kruskal-Wallis test for continuous variable and χ2 test or Fisher's exact test for categorical variables; bLow physical activity was categorized by the definition of the International Physical Activity Questionnaire; cThere were 9 participants who had serum concentrations of 25(OH)D < 20 ng/mL at the screening test, but ≥ 20 ng/mL at baseline examination (4 in daily living group, 3 in sunlight exposure group, 2 in vitamin D supplementation group).
Primary endpoint: changes in serum 25[OH]D levels over 4 weeks
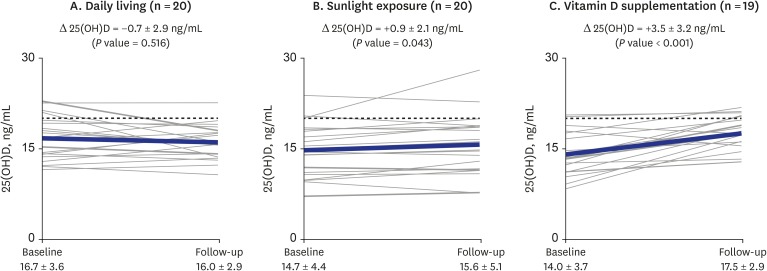
Fig. 2 shows the changes in serum 25(OH)D levels from baseline to follow-up. The largest change in serum 25(OH)D was observed in the vitamin D supplementation group wherein serum 25(OH)D increased from 14.0 ng/mL to 17.5 ng/mL (+3.5 ng/mL, P < 0.001). Although the sunlight exposure group also showed a significant increase in serum 25(OH)D during the follow-up assessment, the absolute increase was less than one-third of that in the vitamin D supplementation group (+0.9 ng/mL, P = 0.043). When the analysis was restricted to 17 subjects with good compliance rates who were exposed to sunlight for more than 12 days across the study period according to the protocol requirements, the results were not different (+0.8 ng/mL). Conversely, the daily living group showed no difference in serum levels (−0.7 ng/mL, P = 0.516). The participants who had a > 20 ng/mL level of serum 25(OH)D at the follow-up timepoint included one in the daily living group, two in the sunlight exposure group, and five participants in the vitamin D supplementation group.
Fig. 2
Changes in serum 25(OH)D (ng/mL) levels among all study participants based on the group.
The thin solid line ( ) indicates change in each individual's level of vitamin D; thick solid line (
) indicates change in each individual's level of vitamin D; thick solid line ( ) indicates the mean change in 25(OH)D level of the group; dotted line (
) indicates the mean change in 25(OH)D level of the group; dotted line ( ) indicates the cutoff value (20 ng/mL) of vitamin D insufficiency. P value for differences between baseline and follow-up were calculated using the Wilcoxon signed-rank test.
) indicates the cutoff value (20 ng/mL) of vitamin D insufficiency. P value for differences between baseline and follow-up were calculated using the Wilcoxon signed-rank test.
) indicates change in each individual's level of vitamin D; thick solid line () indicates the mean change in 25(OH)D level of the group; dotted line () indicates the cutoff value (20 ng/mL) of vitamin D insufficiency. P value for differences between baseline and follow-up were calculated using the Wilcoxon signed-rank test.25(OH)D = 25-hydroxyvitamin D.
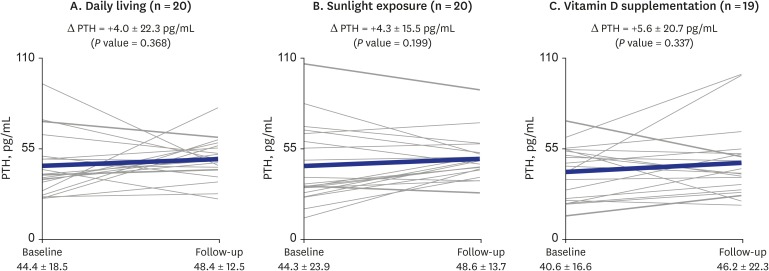
In contrast to the 25(OH)D results, 1,25(OH)2D levels increased from baseline to follow-up similarly in all three groups (Fig. 3). Although the largest increase was observed in the vitamin D supplementation group (+10.2 pg /mL, P < 0.001), increases in the 1,25(OH)2D levels were also observed in both the sunlight exposure and daily living groups (+7.7 pg/mL, P < 0.001; +6.5 pg/mL, P = 0.022). Conversely, none of the three groups showed differences in PTH levels between baseline and follow-up (Fig. 4).
Fig. 3
Changes in serum 1,25(OH)2D (pg/mL) levels among all study participants based on group.
The thin solid line () indicates the change in each individual's level of vitamin D; thick solid line () indicates the mean change in 1,25(OH)2D level of the group. P value for differences between baseline and follow-up were calculated using the Wilcoxon signed-rank test.
) indicates the change in each individual's level of vitamin D; thick solid line () indicates the mean change in 1,25(OH)2D level of the group. P value for differences between baseline and follow-up were calculated using the Wilcoxon signed-rank test.1,25(OH)2D = 1,25-dihydroxyvitamin D3.
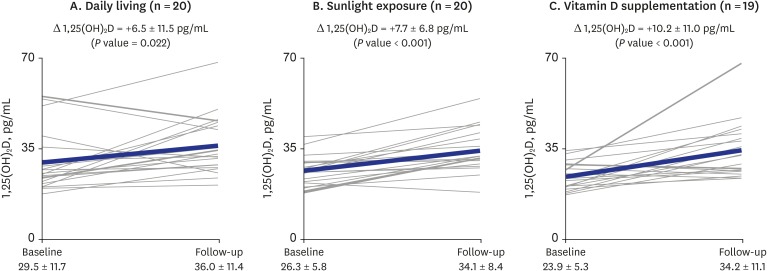
Fig. 4
Changes in serum PTH (pg/mL) levels among all study participants based on the group.
The thin solid line () indicates the change in each individual's level of vitamin D; thick solid line () indicates the mean change in PTH level of the group. P value for differences between baseline and follow-up were calculated using the Wilcoxon signed-rank test.
) indicates the change in each individual's level of vitamin D; thick solid line () indicates the mean change in PTH level of the group. P value for differences between baseline and follow-up were calculated using the Wilcoxon signed-rank test.PTH = parathyroid hormone.
DISCUSSION
In the sunlight exposure group, increase in serum concentrations of 25(OH)D was statistically significant, but the absolute value of this increase was small. In particular, 1 month of sunlight exposure failed to increase serum concentrations of 25(OH)D above 20 ng/mL in most participants. These findings suggest that current guidelines for recommended sunlight exposure may not be sufficient to raise vitamin D levels to adequate concentrations.
In the current study, the sunlight exposure group was instructed to expose 20%–30% of their total body surface area for about 30 minutes per session, at least 3 times between 10:00 A.M. and 3:00 P.M. during the summer. When skin types responding to UV radiation exposure were classified on a scale ranging from type I (pale white) to type VI (deeply pigmented dark brown to black), skin type III was found to be the most common (48.8%) in Korea, followed by types IV (22.2%) and V (17.8%).15 Even though this study did not evaluate skin pigment among study subjects, our protocol would have been sufficient to meet current guidelines, because individuals with type V skin types are advised to maintain 25 minutes of daily sunlight exposure at lunchtime, with exposed forearms and lower legs, in the months of June through August in the UK.16
Besides skin pigmentation, vitamin D skin photosynthesis can be affected by a variety of factors that include sunscreen use, age, season, latitude, and time of day.13 However, we believe that the known vitamin D synthesis-related factors cannot explain why sunlight exposure failed to increase the levels of 25(OH)D above 20 ng/mL in the current study. Firstly, as this study was performed during the summer in a Korean city located at 34 °N latitude, neither season nor latitude can explain our findings. Moreover, the concentrations of 7-dehydrocholesterol in the skin decreases with age, and the capacity to photosynthesize vitamin D3 among the elderly is shown to be markedly diminished when compared with that of younger individuals17; however, our study participants were healthy young adults. Finally, the usage of sunscreen was only permitted on the face and participants were advised to expose 20%–30% of their body surface area to sunlight without sunscreen use.
Our findings are consistent with those of some previous clinical studies in which no increase or only slight increases in serum 25(OH)D levels after sunlight exposure were observed.89 However, as other studies have reported the increase of serum 25(OH)D levels after 2–3 months of sunlight exposure,1011 it is possible that a period of 1 month may be insufficient to restore vitamin D levels among persons with vitamin D insufficiency or deficiency.
As published data indicate that 80%–90% of vitamin D is obtained from sunlight,18 our findings can be interpreted such that current guidelines for sunlight exposure may not be sufficient to increase vitamin D levels. Another explanation is that vitamin D deficiency can exist despite sufficient exposure to sunlight due to unknown causes that ultimately block vitamin D synthesis. As the prevalence of low vitamin D status was high even in countries located around the equator where sun exposure is abundant throughout the year,1 and because sunlight exposure was estimated to explain only 29% of the variance in serum 25(OH)D concentrations during the summer to autumn period among Dutch elderly populations,19 we speculate that the latter explanation may be more plausible.
More specifically, during the vitamin D synthesis process, sunlight exposure is involved only in the initial step, the conversion of 7-dehydrocholesterol to vitamin D3, taking place in the epidermis.20 The synthesis of 25(OH)D, a biomarker of vitamin D levels in humans, requires 25-hydroxylation in the liver and formation of 1,25(OH)2D, the biologically active form of vitamin D, requires 1α-hydroxylation in the kidney.
Enzymes in the cytochrome P450 system are involved in the synthesis and catabolism of 25(OH)D and 1,25(OH)2D, with CYP2R1 and CYP27B1 playing an important role in the synthesis while CYP24A1 plays a catabolic role.21 Therefore, if the 25(OH)D level is low even with adequate sunlight exposure, the low serum concentrations of 25(OH)D may be explained by impairment of 25-hydroxylation or increased catabolism of 25(OH)D. As the cytochrome P450 system is induced or suppressed by a wide range of xenobiotics,22 we speculate that exposure to xenobiotics may be involved in propagating the current epidemic of vitamin D deficiency.
Supporting this idea, common environmental chemicals including DDT, PCBs, phthalate, and bisphenol A were related to low vitamin D levels in humans.23242526 Low serum concentrations of 25(OH)D among cigarette smokers27 can also be interpreted from the viewpoint of cytochrome P450 system involvement because cigarette smoke is a well characterized example of chemical mixtures. Furthermore, the cytochrome P450 system can also explain the link between air pollution and vitamin D deficiency because air pollution is another example of heterogeneous chemical mixtures,28 although the decreased amount of UVB reaching the earth's surface because of air pollution is currently considered to be the main mechanism linking air pollution and vitamin D deficiency.29
In our study, vitamin D supplements effectively increased vitamin D levels. Even though the cytochrome P450 system may be impaired by various environmental pollutants, the high absolute amount of vitamin D3 in the vitamin D supplementation group may help to overcome the functional impairment of the cytochrome P450 system, leading to an increase in the level of 25(OH)D. However, 25(OH)D may not be the only beneficial compound produced during the course of vitamin D metabolism. For example, metabolic products of vitamin D3 or 7-dehydrocholesterol via the cytochrome P450 system can also be biologically active.3031 Therefore, restoration of systemic vitamin D metabolism through sunlight exposure may be an important measure against vitamin D deficiency. Future studies on why UVB failed to sufficiently increase 25(OH)D levels should be performed.
The current study has several limitations. First, a period of 4 weeks may be insufficient to increase 25(OH)D levels through sunlight exposure among persons with vitamin D insufficiency or deficiency. Even though vitamin D supplements were more effective than sunlight exposure in increasing 25(OH)D levels, 1 month was not a sufficient length of time to adequately increase 25(OH)D levels. Second, the compliance with protocol in the sunlight exposure group was assessed through self-reporting in a diary, not by objective tools such as a dosimeter. However, previous studies reported a substantial correlation between sunlight exposure assessed by questionnaires and dosimeter measurements.3233 Third, the sample size was insufficient to conduct stratified analysis according to covariates (including gender, age, and obesity) that are known to be associated with vitamin D levels. Fourth, we did not consider genetic factors; genetic variations in some enzymes have been reported to be associated with vitamin D insufficiency.34
Our findings showed that the generally recommended sun exposure guidelines were not sufficient to raise vitamin D levels to optimal concentrations among individuals with vitamin D insufficiency or deficiency. Considering the high prevalence of vitamin D deficiency among countries near the equator, this failure may not be the result of insufficient exposure time to sunlight; rather, it is suggestive of other underlying causes that may explain the worldwide epidemic of vitamin D deficiency. Research on why sunlight exposure fails to increase 25(OH)D levels is necessary to effectively prevent vitamin D deficiency.
 XML Download
XML Download