

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The standard treatment for ovarian cancer has been primary debulking surgery, followed by post-operative adjuvant chemotherapy (POAC) with intravenous platinum and taxane every 3 weeks [1]. Recently, phase III trials have established neoadjuvant chemotherapy (NAC), followed by interval debulking surgery (IDS), as a valid alternative for advanced-disease patients whose expected morbidity from immediate surgical intervention is too high or optimal debulking is unlikely [23]. However, ovarian cancer continues to be one of the leading causes of cancer deaths, as 5-year survival rate has only improved slightly from 57.2% to 62.8% during the last 20 years in South Korea [45].
Modulation of the administration schedule from the 3-weekly to weekly administration, termed the dose-dense administration of weekly paclitaxel-based chemotherapy and carboplatin every 3 weeks (ddPC), was proposed as a way to improve outcome [678]. One large scale trial by the Japanese Gynecologic Oncology Group (JGOG 3016) showed a dramatic improvement in both progression free survival (PFS) and overall survival (OS) with weekly administration of paclitaxel. However, none of the results from subsequent trials such as multicenter Italian trial in an ovarian cancer (MITO-7), Gynecologic Oncology Group (GOG) 0262, and ICON8 measured up to the previously reported data on survival. The data on the impact of ddPC in the NAC setting in advanced ovarian cancer patients are limited [9]. In the meanwhile, a systematic method to quantify the pathologic response to NAC has been developed. The chemotherapy response score (CRS) is a newly developed pathologic parameter that grades tumor response to NAC on a scale of 1–3. External validation showed that the CRS may serve as a surrogate marker of prognosis [101112].
Various ways were used to compare the efficacy and toxicity of ddPC with the standard 3-weekly regimen in the NAC setting. Patient characteristics, clinical and pathological response to NAC, surgical and survival outcome, and adverse event were compared. We hypothesized that the ddPC regimen will be tolerable generally and that the dose-dense administration of paclitaxel may lead to improved clinical outcomes at the expense of an increased hematologic toxicity.
MATERIALS AND METHODS
1. Study population
A retrospective review of 90 patients with pathologically confirmed diagnosis of advanced ovarian cancer who received at least 1 cycle of NAC followed by IDS at Yonsei Cancer Hospital between August 2015 and January 2018 was conducted. The study was approved by the Institutional Review Board of Severance Hospital. Informed consent was waived owing to the retrospective analysis of the study (IRB No. #4-2018-0518). The start date was chosen based on the earliest identified patient receiving neoadjuvant ddPC. All patients were histologically confirmed to have International Federation of Gynecology and Obstetrics stage IIIc or IV ovarian, tubal, or peritoneal cancer before starting chemotherapy. All surgical procedures were performed by 1 of 5 gynecologic oncology surgeons at our institution. NAC was performed if at least 1 of the following 3 criteria was met: 1) pulmonary and/or hepatic parenchymal metastasis were observed in preoperative imaging studies, 2) patients were inoperable or the operative risk was too high due to comorbidities, or 3) optimal debulking operation (residual meaning 1 cm or less) was unlikely due to high tumor burden (Fagotti score 8 or higher). Patients were excluded if they had incomplete medical records after having received NAC elsewhere or were transferred to a different hospital (n=3); if they were incidentally diagnosed and proceeded with NAC despite low Fagotti score (n=4); if they received taxotere and carboplatin regimen (n=1); and if they received immunotherapy as part of their treatment (n=6).
At our institution, one clinician administered ddPC to all newly diagnosed ovarian cancer patients undergoing NAC, while all other clinicians administered the standard 3-weekly regimen. The final study population consisted of 23 patients in the ddPC group and 50 patients in the standard chemotherapy group (Fig. 1). All patients received paclitaxel and carboplatin combination chemotherapy, preferably administered in 3 cycles of NAC, followed by IDS, and 3 or more cycles of POAC. Unless otherwise indicated, due to old age, poor performance, and medical conditions, patients in the ddPC group were administered weekly paclitaxel (80 mg/m2) on days 1, 8, and 15 with 3-weekly carboplatin (area under the curve [AUC] of 5–6) on day 1, whereas those in the standard group were administered paclitaxel (175 mg/m2) and carboplatin (AUC of 5–6) every 3 weeks. Dose reduction or regimen change was considered if grade 3 and higher toxicity was observed based on the National Cancer Institute's (NCI) common terminology criteria for adverse events (CTCAE) guidelines.
 | Fig. 1Flow diagram of study population which consists of dose-dense chemotherapy group (n=23) and standard 3-weekly group (n=50).ddPC, dose-dense weekly paclitaxel and 3-weekly carboplatin; NAC, neoadjuvant chemotherapy.
|
At the time of diagnostic laparoscopy and primary surgery, the extent of tumor burden was assessed with the peritoneal cancer index described by Sugarbaker and Fagotti score. With the intent to achieve complete cytoreduction, either through laparoscopy or laparotomy, all patients followed conventional surgical procedures, which included the sampling of peritoneal washing for cytology, a thorough inspection of the abdomen and pelvis (upper abdominal viscera, diaphragm, and retroperitoneal spaces), hysterectomy, bilateral salpingo-oophorectomy, omentectomy, appendectomy, pelvic or para-aortic lymph node dissection, and surgical resection of all macroscopically detectable lesions. The operation was defined as radical if any of the following procedures was involved: bowel resection, diaphragm or other peritoneal surface stripping, splenectomy, partial hepatectomy [13]. All microscopic slides were reviewed by 2 experienced gynecologic pathologists, and histological diagnoses were made based on World Health Organization criteria; after which, 3-tiered CRS scores were calculated as reported in the previous study [14].
Abstracted data included patient demographics, medical comorbidities, American Society of Anesthesiologists (ASA) score, serum cancer antigen-125 (CA 125) levels, and oncologic history including diagnostic procedure, tumor histology and grade, and stage at initial diagnosis. Charts were reviewed for various details regarding NAC such as the initial regimen, number of cycles received, changes in therapy, treatment delays, dose reductions, hospitalization, toxicity, and addition of granulocyte-colony stimulating factor (G-CSF). Grading of toxicity was based on NCI's CTCAE version 4.0. Results from abdominal and pelvic computed tomography (APCT) after initial diagnosis and prior to IDS were reviewed. Surgical records were reviewed for details on the date and the extent of surgery, and residual disease after IDS.
2. Statistical analysis
SPSS statistical software (version 21.0; IBM corp., Armonk, NY, USA) was used for the statistical analyses. Statistical significance was calculated using the Fischer's exact for categorical variables and the student t-test for continuous variables, where applicable. The end points included the PFS, which was defined as the interval between the date of diagnosis and the date of first recurrence. PFS was analyzed with Kaplan-Meier method and log-rank test. A stepwise Cox proportional hazards regression model was used to evaluate the potential impact of prognostic variables on disease recurrence. Covariates included chemotherapy group assignment, age, initial performance score, stage, histologic subtypes, and presence of BRCA mutation, and the number of NAC cycles received. For all analyses, p<0.05 was considered as statistically significant.
RESULTS
1. Patient demographics
A total of 23 patients in the ddPC and 50 patients in standard 3-weekly group were analyzed. Patient and clinical characteristics are shown in Table 1. The median ages and ASA scores of patients in both groups were comparable. Both groups showed a similar proportion of stage IIIc and IV ovarian cancer patients. The median CA 125 levels at presentation were similar: 1,391.2 IU/mL (range: 385.4–3407.5) in the ddPC group versus 1,559.5 IU/mL (range: 67.7–23918.5) in the standard group (p=0.302). Serous carcinoma histology type was found in over 90% of patients. BRCA 1 or 2 mutation status was comparable between both groups.
Table 1
Baseline characteristics of patients
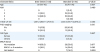
Values are presented as median (range) or number (%).
ASA, American Society of Anesthesiologists; CA 125, cancer antigen-125; FIGO, International Federation of Gynecology and Obstetrics.
![]()
2. Chemotherapy tolerability and toxicity
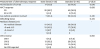
Markers of chemotherapy tolerability are shown in Table 2. Patients in the ddPC and standard group both received a median of 3 NAC cycles (p=0.377). One patient in the ddPC group received IDS after 2 NAC cycles due to severe ascites and exacerbation of underlying comorbidities. Dose was reduced during NAC in 8 patients (34.8%) in the ddPC group and in 2 patients (4.0%) in the standard group (p=0.001).
Table 2
Tolerability and toxicity of NAC

Values are presented as median (range) or number (%).
NA, not available; NAC, neoadjuvant chemotherapy.
![]()
Table 2 demonstrates chemotherapy toxicity according to CTCAE guidelines. Events of grade III and higher neutropenia were observed more often in the ddPC group than in the standard group (82.6% vs. 22.0%, p<0.001). In the ddPC group, 12 patients (52.2%) received red blood cell transfusion, whereas no patient received platelet transfusion. In total, 18 patients (85.7%) in the ddPC group and 14 patients (28.0%) in the standard group received at least 1 cycle of G-CSF replacement; yet there were no events of neutropenic fever. Rates of grade III and higher anemia and lymphopenia were not significantly different, and there was no event of grade III and higher thrombocytopenia. Other non-hematologic toxicities including infection, thrombosis, gastrointestinal, and fatigue were comparable between both groups.
Treatment delay of more than 1 week incurred in 3 patients (13.0%) in the ddPC group due to pancytopenia, whereas no patient in the standard group experienced treatment delay (p=0.028). The difference in the rate of hospitalization was not statistically significant between the 2 groups (17.4% in ddPC group vs. 4.0% in standard group, p=0.074). Indications for hospitalization in the ddPC group included infection (n=4), nausea and vomiting (n=1), and fatigue (n=1). One patient in the standard group was hospitalized for continuation of intravenous antibiotic treatment for infective spondylitis, and underlying diagnosis prior to NAC. All other hospitalized patients were admitted once during NAC and for duration of less than 1 week, and indications for hospitalization included non-neutropenic fever, gastrointestinal symptom, and fatigue. There were no events of small bowel obstruction and intra-abdominal hemorrhage.
3. Response to NAC and surgical treatment
Responses following NAC are demonstrated in Table 3. Normalization of CA 125 occurred more frequently in the ddPC group than in the standard group (73.9% vs. 46.0%, p=0.030). Except for 1 patient in the ddPC group and 5 patients in the standard group, APCT showed partial response findings prior to IDS. The rate of involvement of any radical procedure was comparable between both groups (30.4% vs. 40.0%, p=0.432). Debulking status was also comparable; no residual disease was diagnosed in 9 patients (43.5%) in the ddPC group and in 30 patients (60.0%) in the standard group (p=0.434). In terms of pathological response, omental CRS was reported in 66 out of 73 patients (90.4%). The 2 groups were comparable in terms of omental CRS—score of 3 was observed in 8 out of 20 patients (34.8%) in the ddPC group, compared with 13 out of 44 patients (26.0%) in the standard group (p=0.441). The PFS at 2 years was 36.3% in the ddPC group and 28.4% in the standard 3-weekly group (p=0.454) (Fig. 2). Median PFS was 19.0 months (95% confidence interval [CI]=16.4–21.6) in the ddPC group and 18.0 months (95% CI=13.3–22.7) in the standard 3-weekly group. Cox regression analysis showed that ddPC was not a significant determinant for PFS when all other prognostic variables were considered (hazard ratio=0.911, 95% CI=0.417–1.993) (Table 4); advanced initial cancer stage (p=0.033) and presence of BRCA mutation (p=0.016) were the significant determinants.
Table 3
Response to treatment in terms of blood tests, image studies, debulking status, and CRS
Values are presented as number (%).
APCT, abdominal and pelvic computed tomography; CA 125, cancer antigen-125; CRS, chemotherapy response score; PD, progressive disease; PR, partial response; SD, stable disease.
![]()
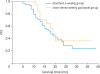 | Fig. 2Kaplan-Meier curves of PFS of patients who are treated with dose-dense administration of weekly paclitaxel combined with 3-weekly carboplatin versus standard 3-weekly paclitaxel and carboplatin chemotherapy regimen.PFS, progression-free survival.
|
Table 4
Multivariate analysis using potential covariates for progression free survival

ASA, American Society of Anesthesiologists; CI, confidence interval; ddPC, dose-dense weekly paclitaxel and 3-weekly carboplatin; HR, hazard ratio.
![]()
DISCUSSION
Dose-dense chemotherapy using weekly paclitaxel and 3-weekly carboplatin regimen was tolerable in all patients in our cohort, yet not without increased events of hematologic toxicity. Contrary to our hypothesis, although the optimal debulking rate was similar to previous reports, the clinical outcomes were not significantly different between the two groups, both immediately and in the long-term. The median months of observation until death or the most recent out-patient visit was 18 months (range: 2–40). Out of 73 patients in total, recurrence was observed in 37 patients (50.7%). PFS in the ddPC group was not superior, and the non-superiority was further shown in the multivariable analysis.
Previously, the potential clinical benefit of ddPC was suggested in the context of breast cancer treatment [15]. The theoretical rationale states that ddPC may improve clinical outcome while minimizing toxicity by effectively targeting highly proliferative tumor cells through increased time and intensity of drug exposure, along with additional antiangiogenic effect [161718]. According to a randomized phase 3 trial by JGOG 3016, the ddPC group was significantly better in terms of both PFS and OS [6]. Nevertheless, results from the following large-scale studies were equivocal. A MITO-7 study, which incorporated a variation in regimen using weekly doses of carboplatin (AUC of 2), showed that the survival outcome of the ddPC group patients was not different from that of the standard group [7]. Another trial by Chan et al. [8] (GOG 0262) showed that the addition of an anti-angiogenic agent such as bevacizumab to the standard regimen offsets the survival benefit incurred by the dose-dense administration of weekly paclitaxel in addition to the 3-weekly carboplatin.
Nonetheless, the questions of the optimal timing of ddPC administration, whether in the first-line, palliative, or neoadjuvant setting, and the selection of the patient subgroup that will benefit the most from the dose-dense schedule are under active investigations. Recently, an improved survival of ddPC in NAC setting has been suggested by Becker et al., [9] alongside a favorable trend towards pathologic complete remission. The most recent meta-analysis on ovarian cancer by Marchetti et al. [19] also showed a statistically non-significant, yet favorable trend towards better clinical outcomes in the ddPC regimen when compared to the standard regimen. As stated above, we were not able to detect a measurable difference in prognosis.
These differences in outcome when compared with previous studies may be explained by the dissimilarity in background characteristics of the patient cohort. For instance, compared to the JGOG 3016 and GOG 0262, our patient cohort had a higher proportion of stage IV ovarian cancer patients [68]. Toxicity-wise, Asian populations have a tendency to be more vulnerable to chemotherapy toxicity, owing to race-specific polymorphisms [20].
Specific to our study was that weekly paclitaxel and 3-weekly carboplatin were utilized in the NAC setting in a single institution where the patient population is homogenous. Moreover, ddPC was provided by one clinician over a short time period, and relatively consistent criteria were used for all patients in determining NAC and evaluating toxicity. Within our NAC setting, ddPC was tolerable with all but 1 patient receiving 3 cycles of NAC, no events of regimen conversion during NAC, and administration of weekly paclitaxel mostly according to the planned schedule with the addition of G-CSF. A similar level of tolerability of ddPC as NAC was also suggested in a retrospective case control study by Becker et al. [9] and a single cohort study by Ebata et al. [21].
Nonetheless, consistently shown in these previous studies was a marked increase in grade III/IV hematologic toxicity—anemia ranging from 41.9% to 45%, neutropenia from 19.0% to 41.9%, and thrombocytopenia from 19.0% to 21.7%. In comparison, our ddPC patient cohort showed less frequent events of anemia (13.0%), thrombocytopenia (0%), and increased events of neutropenia (82.6%), possibly because prophylactic G-CSF was not routinely administered in our institution. Although ddPC was tolerable and most hematologic toxicities could be overcome by transfusion – considering that as many as 90.5% of patients experienced any grade III/IV toxicity – clinicians should carefully gauge as to whether the potential non-significant survival gain is worth the cost of probable toxicity. For the same reason that the ddPC regimen may serve as a cost-effective substitute to adding Bevacizumab to standard 3-weekly chemotherapy regimen as suggested in GOG 0262 [8], the financial cost of managing grade III/IV toxicity and psychological burden to patients may deserve a due consideration.
The limitation of our study includes its design as a retrospective study on a relatively small scale, whereas a small yet homogenous study performed in a well-controlled environment in a single institution could have contributed to the strength of our study. Since the patients in the ddPC group visited the hospital more frequently, there is a possibility of surveillance bias when evaluating chemotherapy toxicity. Future prospective studies may involve stratification of patients based on age, performance score, and ethnicity in order to identify a subgroup of patients who may better tolerate and clinically benefit the most from the weekly administration of chemotherapy. Furthermore, recent investigations on the molecular and genetic subtyping of ovarian cancer may help identify patients who may benefit the most from dose-dense administration of paclitaxel [20].
Moreover, with the option of combination therapy using target therapy and immunotherapy, the differential impact of dose-dense administration of paclitaxel-based NAC on tumor microenvironment, cytokine production, and lymphoid homeostasis may serve as scientific clues to improve clinical outcomes [222324]. Clinicians may further investigate whether ddPC-specific alterations in the hematological profile—what currently appears to be an increased hematologic toxicity—paradoxically serve a prognostic advantage when combined with certain immune modulating drugs.
 XML Download
XML Download