

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cervical cancer is the fourth most common cancer among women worldwide, with an estimated 500,000 new cases and 250,000 deaths in 2012 [1]. The majority of the cases are squamous cell carcinomas (SCCs), followed by adenocarcinomas [2]. The incidence and mortality rates of SCC cases are decreasing [3]. However, despite being a relatively rare histological subtype of cervical cancer, the incidence of uterine cervical adeno/adenosquamous carcinoma (UCAA) in many countries is rising [4]. Therapeutic approaches for cervical cancer result from studies where the majority of the patients had SCC because adenocarcinoma comprises an average of only 10% of the cases [5]. There are few studies investigating UCAA and its treatment options, and thus, the disease is typically treated in a manner similar to SCCs [67]. Adenocarcinomas are more resistant to radiation compared to SCCs, with poorer local control (LC) and overall survival (OS) [68].
Carbon-ion (C-ion) radiotherapy (CIRT) was proposed as a therapeutic option for UCAA. It has been utilized for about 2 decades as an effective therapeutic option for some types of malignancies, like sarcomas, and head and neck tumors [9]. In comparison with photon radiation, C-ion beams possess some biological advantages. C-ion beams deliver a lower entry dose, depositing the majority of their energy at the flight path terminus, yielding an asymptotic dose peak (the “Bragg Peak”) [10] due to which C-ion beams can improve dose localization, which can have great effects on tumors while minimizing normal tissue damage. Moreover, C-ion beams also have biological advantages due to their high-linear energy transfer, which provides a high density of energy deposition per unit length [11]. The CIRT resulted in favorable outcomes in the patients with radio-resistant head and neck tumors, like mucosal malignant melanoma and adenoid cystic carcinoma [1213]. The CIRT showed a 5-year OS of 53%, whereas the standard 3-year OS rate was 26% in unresectable chondrosarcoma [1415]. These successes provide a rationale for the application of CIRT for treating UCAA that is resistant to conventional radiotherapy (RT) and accumulating evidence has shown that CIRT holds promise as an effective therapeutic option for treating UCAA [9161718].
Programmed cell death-ligand 1 (PD-L1) is expressed in various types of cancers and is the major ligand for programmed cell death-1 (PD-1), which is an immune checkpoint expressed on the surface of activated T-cells [19]. The PD-1/PD-L1 blockade immunotherapy is widely accepted and has been used against various types of cancers to improve the survival of the patients who respond to the immune checkpoint inhibitors. PD-L1 expression in tumors has been shown to predict clinical outcomes in some tumors, and negative associations of tumor PD-L1 expression with prognosis have been reported for several cancers [2021222324]. Although there were many studies reporting the clinical relationship between PD-L1 expression and clinical outcome in cancer, clinical significance of PD-L1 expression in UCAA after CIRT remains unknown.
In this study, we investigated the impact of PD-L1 expression on UCAA in CIRT using human UCAA cells and clinical samples from patients before CIRT started (pre-CIRT) and after 12 Gy irradiation (post-12Gy-C). We also evaluated the association of PD-L1 expression with clinicopathologic parameters and clinical outcomes in UCAA patients receiving CIRT.
MATERIALS AND METHODS
1. Cell culture, irradiation, and drug treatment
HeLa cells, the human cervical adenocarcinoma cells, were purchased from RIKEN cell bank (Tsukuba, Japan). SiHa cells, the human cervical SCC cells, were purchased from American Type Culture Collection (Manassas, VA, USA). The cells were cultured in Eagle's Minimum Essential Medium (Wako, Osaka, Japan) with 10% fetal bovine serum (GE healthcare, Chicago, IL, USA). The cells were maintained in a humidified incubator with 5% CO2. X-ray irradiation was performed using TITAN (Shimadzu, Kyoto, Japan). Exponentially grown cells were irradiated with X-ray at a dose rate of 0.9–1.0 Gy/min. C-ion beam irradiation was performed at the Heavy Ion Medical Accelerator in Chiba (National Institute of Radiological Sciences, Chiba, Japan). A linear energy transfer value of up to 70 keV/μm was used for C-ion (290 MeV/nucleon). A Chk1 inhibitor (1 μM TCS 2312; Tocris Bioscience, Bristol, UK) was added 1 hour prior to irradiation with X-ray or C-ion, and the cells were incubated until they are harvested.
2. Flow cytometry analysis
Cancer cells were incubated for 48 h after exposure to X-ray or C-ion irradiation in the presence or absence of Chk1 inhibitors and then harvested for flow cytometry analysis. Adherent cells were harvested by shaking in 2 mM ethylenediaminetetraacetic acid-phosphate buffered saline without trypsinization. Collected cells were washed with ice-cold fluorescence-activated cell sorting solution and then stained with anti-PD-L1 antibody (1:10; BioLegend, San Diego, CA, USA) for 20 minutes at 4°C. Subsequently, the cells were treated with secondary antibody (1:200, Alexa Flour® 647 Conjugate; Cell Signaling Technology, Danvers, MA, USA) for 20 minutes at 4°C. Dead cells detected by propidium iodide were excluded from the analysis. Flow cytometry analysis was performed on CytoFLEX (Beckman Coulter, Inc., Brea, CA, USA). The mean fluorescence intensity (MFI; PD-L1/isotype) is calculated by diving MFI of PD-L1 by MFI of isotype control.
3. Western blotting
Immunoblotting was performed by using the whole cell lysates, sampled 2 hours after irradiation. Cells were lysed on ice in 2× Laemmli sample buffer (Bio-Rad, Hercules, CA, USA) with 5% 2-mercaptoethanol (Nacalai tesque, Kyoto, Japan). Cell lysates were boiled for 10 minutes at 95°C. Equal amounts of protein samples were separated by sodium dodecyl sulfate polyacrylamide gel electrophoresis and protein bands were transferred to a polyvinylidene fluoride membrane (Merck Millipore, Burlington, MA, USA). The membranes were blocked with Bullet Blocking One for Western Blotting (Nacalai tesque) for 5 minutes at room temperature and then incubated with the indicated primary antibodies by gently shaking at room temperature for 1 hour. Membranes were washed twice with Tris-buffered saline containing 0.1% Tween 20 and incubated with the corresponding secondary antibodies. For detecting Chk1 and phosphorylated Chk1, phospho-Chk1/2 antibody sampler kit (1:1,000 dilution; Cell Signaling Technology) was used. For detecting β-tubulin, anti-β-tubulin antibody (1:1,000 dilution; Wako) was used. Goat anti-rabbit IgG-horseradish peroxidase conjugate (Bio-Rad) was used as a secondary antibody. The signal was detected using Chemi-Lumi One Super (Nacalai tesque). Image acquisition was performed using GENE GNOME (Syngene, Frederick, MD, USA). Quantitation of the band intensity was performed using ImageJ 1.51 (National Institute of Health, Bethesda, MD, USA) [25].
4. Patient populations
Out of the 55 UCAA patients who received CIRT in a previous clinical trial [17], 33 patients who were subjected to pre-CIRT and post-12Gy-C tumor biopsy were enrolled. All participants were from a single center. The eligibility criteria were: i) patients with histologically proven stage IIB–IVA UCAA according to the International Federation of Gynecology and Obstetrics who were previously untreated, ii) patients between 20 and 85 years of age, and iii) patients with an Eastern Cooperative Oncology Group performance status of 0–2. The exclusion criteria included: i) patients, who had para-aortic lymph node of diameter ≥1.0 cm, measured according to computed tomography (CT) images, ii) patients suspected of distant metastasis by CT, and iii) patients with a severe pelvic infection, psychological illness, severe diabetes mellitus, or active double cancer. All of them were followed up for at least 6 months. Abdominal and pelvic CT scans, pelvic magnetic resonance imaging (MRI), and fluorodeoxyglucose positron emission tomography (PET)-CT scans for accurate staging were performed on all the patients. Tumor size was assessed by pelvic examination and MRI. We measured the dimensions of the cervical tumors using T2-weighted MRI images [17]. Approval for this study was obtained from our Institutional Review Board (National Institute of Radiological Sciences Certified Review Board, NIRS 17-030). All procedures performed involving human samples, performed in this study, were in compliance with the Declaration of Helsinki.
5. CIRT
Customized cradles were individually made for all patients, and the patients were immobilized with a low-temperature thermoplastic sheet during CT for treatment planning and during irradiation. All patients underwent a set of 5-mm-thick CT images for 3-dimensional treatment planning using HIPLAN software (National Institute of Radiological Sciences, Chiba, Japan). The patients were administered CIRT for 4 days/week (Tuesday to Friday). Gray relative biological effectiveness [Gy (RBE)], which was defined as the physical doses multiplied by the RBE of the C-ions, was used to express the radiation dose calculated for the target volume and surrounding normal structures. The patients were treated in a dose-escalation manner described in a previous clinical trial [17]; the total radiation doses administered to the cervical tumor were: 62.4, 64.8, 68.0, 71.2, or 74.4 Gy (RBE) in 20 fractions. The first 12 out of all 20 fractions were treated with a fixed-dose schedule, and the treatment consisted of whole-pelvic irradiation of 36.0 Gy (RBE) in the 12 fractions and local boost with dose-escalation from 26.4 to 38.4 Gy (RBE) in 8 fractions [17].
6. Biopsies
Tumor biopsy specimens were collected twice from each patient; the specimens were collected at least 4 weeks before CIRT and after 12 Gy (RBE)-irradiation in 4 fractions 1 week after starting CIRT. The specimens were formalin-fixed, paraffin-embedded, sectioned for microscopic examination, and stained with hematoxylin and eosin. For histological diagnosis, we re-assessed all tumor specimens according to the World Health Organization classification in 2014 [26]. The pathologies were reviewed by multiple pathologists from our and another hospital.
7. Immunohistochemical analysis
After formalin-fixed and paraffin-embedded tissue samples of 4 μm-thick sections were treated with xylene and ethanol, antigen retrieval was performed in ethylene glycol and sodium azide, pH 9.0, at 120°C for 20 minutes. The sections were then incubated with anti-PD-L1 (clone E3L1N; Cell Signaling Technology) at a 1:100 dilution and with anti-CD8 (clone C8/144B; Dako, Glostrup, Denmark) at a 1:400 dilution overnight at 4°C. Subsequently, the sections were treated with secondary antibody at room temperature for 30 minutes. The slides were incubated with the SignalStain DAB (Cell Signaling Technology) and counterstained with hematoxylin. They were observed under the microscope (Keyence, Osaka, Japan), and the images were collected. Tumor PD-L1 expression was defined as positive when staining of the tumor-cell membrane (at any intensity) was observed in ≥1% of the cells, and as negative when no staining or positive staining was detected in <1% of the cells. We set a threshold of 1% based on a previous phase III trial involving an anti-PD-1 agent and another study [2728]. CD8+ lymphocyte infiltration was defined as positive when there were ≥30 CD8+ lymphocytes in a 40× field of view. Two independent investigators assessed the expressions and the infiltrations.
8. Statistical analysis
Student's t-test was used in in vitro studies. The pre-CIRT and post-12Gy-C changes in PD-L1 expression were analyzed by the McNemar test. LC, progression-free survival (PFS), and OS were assessed by the Kaplan-Meier method and the log rank test was used for comparison. Statistical significance was set at p<0.05. Statistical Package for Social Science, software version 24.0 (IBM Inc., Armonk, NY, USA) was used for all the analyses.
RESULTS
1. Enhanced PD-L1 expression by C-ion beam in human UCAA and cervical SCC cells
To investigate whether C-ion beam alters PD-L1 expression in human UCAA cells, HeLa cells were irradiated with C-ion beam at different doses. PD-L1 expression was enhanced in a dose-dependent manner by C-ion beam 48 hours after irradiation, as well as X-ray that was used as reference; a significant difference was observed between C-ion and X-ray at 5 Gy of irradiation in HeLa cells (Fig. 1A). The expression was significantly enhanced at 5 and 10 Gy of C-ion beam irradiation compared to non-irradiation in HeLa cells (Fig. 1B). Phosphorylation of Chk1 was observed in HeLa cells irradiated with C-ion as well as with X-ray 2 hours after irradiation, and higher levels of Chk1 phosphorylation was found in C-ion compared to X-ray (Fig. 1C). The expression of PD-L1 was decreased by approximately 40% in presence of a Chk1 inhibitor (1 μM) when irradiated with 5 Gy of C-ion, which was significant (p<0.05) in HeLa cells (Fig. 1D). The expression of PD-L1 was upregulated by C-ion beam 48 hours after irradiation, and its upregulation was suppressed in the presence of a Chk1 inhibitor (1 μM) with a significant difference (p<0.05) in SiHa as well as HeLa cells (Fig. 1E).
Fig. 1
PD-L1 expression in cells irradiated. (A) PD-L1 in HeLa. (B) PD-L1 in HeLa after C-ion irradiation. (C) Quantified blots for phosphorylated Chk1, Chk1, and β-tubulin (loading control) in HeLa. (D, E) C-ion-induced PD-L1 in HeLa (D) and SiHa (E) with Chk1 inhibition.
APC, antigen-presenting cell; C-ion, carbon-ion; DMSO, dimethyl sulfoxide; MFI, mean fluorescence intensity; PD-L1, programmed cell death-ligand 1; SEM, standard error of the mean.
*p<0.05; †p<0.01.

2. PD-L1 expression in UCAA samples receiving CIRT: enhancement of PD-L1 expression by CIRT
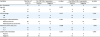
To investigate the clinical relevance of the enhanced PD-L1 expression by C-ion beam in human cervical adenocarcinoma cells, we evaluated PD-L1 expression in UCAA samples from patients. The patient characteristics are summarized in Table 1. The median age was 60 years (range, 33–85 years). Adenocarcinoma occurred in 29 (88%) patients, including 15 (45%) with endocervical adenocarcinoma, usual type, 6 (18%) with mucinous carcinoma, not otherwise specified, 1 (3%) with mucinous carcinoma, gastric type, 1 (3%) with mucinous carcinoma, intestinal type, and 1 (3%) with mucinous carcinoma, signet-ring cell type, 3 (9%) with endometrioid carcinoma, 1 (3%) with clear cell carcinoma, and 1 (3%) was unknown. Four (12%) patients had adenosquamous carcinoma. The median maximum tumor diameter was 5.3 cm (range, 3.4–11.8 cm). Thirteen (39%) of the patients had stage IIB disease, 19 (58%) had stage IIIB disease, and 1 (3%) had stage IVA disease. Regional lymph node metastasis was observed in 13 (39%) patients by CT imaging or MRI. The total dose of CIRT was 62.4 Gy (RBE) in 2 (6%) patients, 64.8 Gy (RBE) in 3 (9%) patients, 68.0 Gy (RBE) in 6 (18%) patients, 71.2 Gy (RBE) patients in 8 (24%), and 74.4 Gy (RBE) in 14 (42%) patients. The median follow-up duration was 33.7 months (range, 6.2–177.3 months). We conducted PD-L1 staining using clinical UCAA samples (Fig. 2). In 15 of the 33 (45%) UCAA specimens obtained from patients, pre-CIRT PD-L1 membrane reactivity was detected. The remaining 18 (55%) were characterized by the complete absence of membrane staining with <1% immunoreactivity. On the other hand, in 22 of the 33 (67%) UCAA specimens obtained from patients, post-12Gy-C PD-L1 membrane reactivity was detected. Post-12Gy-C PD-L1 expression was significantly elevated compared to the pre-CIRT PD-L1 expression (Fig. 2E, p=0.046). Eight out of eighteen patients whose expression of PD-L1 was determined to be negative pre-CIRT were determined to be positive for PD-L1 expression post-12Gy-C. On the other hand, one out of fifteen patients whose expression of PD-L1 was determined to be positive pre-CIRT was negative for PD-L1 expression post-12Gy-C. The relationship between clinical parameters or pathologic features and the frequency of PD-L1 reactivity before or after the initiation of CIRT are shown in Table 2. There was no significant difference in PD-L1 expression with regard to age, clinical stage, histological subclassification, maximum tumor size, or lymph node metastasis.
Table 1
Patient characteristics (n=33)

Fig. 2
PD-L1 staining and changes in PD-L1 status pre-CIRT and post-12Gy-C. (A) PD-L1 staining with a membranous pattern. (B) Negative PD-L1. (C, D) PD-L1 staining of specimens from the same patient before CIRT (C) and after 12 Gy of CIRT (D). The inset at a higher magnification. (E) Change in PD-L1 status pre-CIRT and post-12Gy-C.
CIRT, carbon-ion radiotherapy; PD-L1, programmed cell death-ligand 1.

Table 2
The relationship between clinical parameters or pathologic characteristics and the frequency of PD-L1 reactivity before or after the starting of CIRT
3. Correlation between PD-L1 expression and clinical outcomes
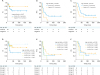
We investigated whether the status of PD-L1 expression correlated with clinical outcomes, such as LC, PFS, and OS in UCAA after CIRT. First, 3 groups (group 1: PD-L1 positive pre-CIRT and post-12Gy-C; group 2: PD-L1 negative pre-CIRT but positive post-12Gy-C; group 3: PD-L1 negative pre-CIRT and post-12Gy-C) were analyzed (Fig. 3). Although group 3, which was PD-L1 negative throughout, was prone to be better in LC and worse in PFS and OS in comparison with the other 2 groups, there were no significant differences in the clinical outcome among the 3 groups. Next, we investigated a correlation between clinical outcome and PD-L1 status before and after the starting of CIRT. Kaplan-Meier analysis revealed that the LC, PFS, and OS of the patients with positive and negative pre-CIRT PD-L1 expression showed no significant difference (Supplementary Fig. 1). In contrast, patients with positive post-12Gy-C PD-L1 expression had a longer PFS than those with negative PD-L1 expression (p=0.008); however, the LC and OS between the 2 groups showed no significant difference (Fig. 4A-C). Furthermore, we classified the patients into 4 groups on the basis of the status of PD-L1 and CD8+ lymphocyte infiltration in the post-12Gy-C tumor tissues (Fig. 4D-F). These include group A (PD-L1 positive with CD8+ lymphocyte infiltration), group B (PD-L1 positive with no CD8+ lymphocyte infiltration), group C (PD-L1 negative with CD8+ lymphocyte infiltration), and group D (PD-L1 negative with no CD8+ lymphocyte infiltration). Although there were significant differences between group A and group D in PFS (p=0.016), and between group B and group D in PFS (p=0.003), no significant difference, other than the 2 pairs, was found between the 2 groups selected from the 4 groups. There was no correlation between the total irradiation doses of CIRT and LC, PFS, and OS (Supplementary Fig. 2).
Fig. 3
Survival curves of patients with UCAA in 3 groups. Group 1: PD-L1 positive pre-CIRT and post-12Gy-C; Group 2: PD-L1 negative pre-CIRT but positive post-12Gy-C; Group 3: PD-L1 negative both pre-CIRT and post-12Gy-C. (A) LC (p=0.685). (B) PFS (p=0.052). (C) OS (p=0.321).
CIRT, carbon-ion radiotherapy; LC, local control; OS, overall survival; PD-L1, programmed cell death-ligand 1; PFS, progression-free survival; UCAA, uterine cervical adeno/adenosquamous carcinoma.

Fig. 4
Clinical outcome. (A-C) Patients with UCAA biopsied post-12Gy-C, with positive (blue, n=22) or negative (orange, n=11) PD-L1. (D-F) PD-L1/lymphocyte status and clinical outcome. Groups A (n=8), B (n=14), C (n=4), and D (n=7). (A, D) LC. (B, E) PFS. (C, F) OS.
CIRT, carbon-ion radiotherapy; LC, local control; OS, overall survival; PD-L1, programmed cell death-ligand 1; PFS, progression-free survival; UCAA, uterine cervical adeno/adenosquamous carcinoma.
DISCUSSION
In this study, we found that PD-L1 expression was upregulated by C-ion beam in human UCAA HeLa and cervical SCC SiHa cells via activated Chk1 pathway. To investigate the clinical relevance of these findings, we examined the pre-CIRT and post-12Gy-C changes of PD-L1 expression in UCAA using clinical specimens to investigate the impact of PD-L1 expression on clinical outcome in patients with UCAA. We found that CIRT enhanced PD-L1 expression in 8 out of 18 patients with UCAA (44%) who were negative for PD-L1 before CIRT. We also found that the PD-L1 post-12Gy-C expression was significantly related to the extension of PFS, but not LC or OS. There was no significant relationship between the pre-CIRT PD-L1 expression and LC, PFS, or OS.
Our in vitro data revealed that C-ion beam enhanced the PD-L1 expression in HeLa cells as well as X-ray. This study indicated that C-ion induced PD-L1 expression more than X-ray. A recent report showed that X-ray irradiation upregulated PD-L1 expression via the ATM/ATR/Chk1 pathway induced by DNA double strand break (DSB) [29]. Given that DSB is formed by C-ion as well as X-ray irradiation, it is reasonable that PD-L1 expression is promoted by CIRT probably through the same mechanism. Therefore, we examined the phosphorylation status of Chk1, which is induced by DSB, in HeLa cells irradiated with C-ion. Higher levels of phosphorylated Chk1 were observed in cells irradiated with C-ion compared to X-ray. Further, Chk1 inhibition reversed the PD-L1 upregulation by C-ion. In SiHa cells, similar results were obtained. These data strongly suggest that upregulation of PD-L1 expression by C-ion beam depends on the Chk1 pathway that is activated by DSB.
This study indicated that group 3, which was PD-L1 negative throughout, tended to be better in LC than the other 2 groups that showed PD-L1 positivity throughout or converted to a positive status for PD-L1 post-12Gy-C. Similarly, tumors negative for PD-L1 post-12Gy-C had better LC than those positive for PD-L1. These results suggest that PD-L1-negative UCAAs are well controlled in tumor growth at the irradiated sites after CIRT. This is presumably because the cells are sensitive to infiltrated cytotoxic T-cells due to the absence of a PD-L1 inhibitory signal.
We found that patients with positive post-12Gy-C PD-L1 expression significantly had a longer PFS. This finding suggests that UCAA positive for PD-L1 post-12Gy-C may be relatively indolent, or PD-L1-negative UCAA may have a potential of invasiveness and metastasis. Given that tumors evade the host immune response through PD-L1 expression, the results of the present study may be paradoxical. There are many contradicting reports regarding PD-L1, and thus, the prognostic value of PD-L1 remains controversial. Reportedly, renal cell carcinoma patients with PD-L1 expression were at significant risk of rapid cancer progression and accelerated rates of mortality [21]. Pancreatic cancer patients with PD-L1 expression had a significantly poorer OS than the PD-L1 negative patients [24]. In contrast, it has been reported that PD-L1 expression in tumor cells is associated with better prognosis in some tumors [30313233]. The PD-L1 negative Merkel cell carcinomas were independently associated with a poor OS [31]. PD-L1 expression had a better correlation with relapse-free survival in patients with surgically resected stage I lung adenocarcinomas [33]. We analyzed the 4 groups classified on the basis of the status of PD-L1 and CD8+ lymphocyte infiltration. However, the reason for better PFS post-12Gy-C PD-L1 positive group was unknown. Further studies may be needed to address this issue.
The result that post-12Gy-C PD-L1 expression in UCAA was enhanced, is consistent with previous reports showing that PD-L1 expression in cancer cells is transiently upregulated following irradiation in an immunocompetent mouse model [3435]. In a clinical setting, after RT, the PD-L1 expression was induced in soft tissue sarcoma after pre-operative RT [36]. In contrast, the percentage of PD-L1-positive locally advanced non-small cell lung cancer cells significantly decreased after concurrent chemo-RT [37]. These works and our present study using CIRT strongly suggest ionizing radiation (IR) can alter PD-L1 expression in tumor cells. However, as the 2 clinical works showed contradictory results, the alteration of PD-L1 expression after RT may be modified by clinical factors, such as types of cancer, duration of treatment, and dose fractionation. Elucidating the mechanism(s) of PD-L1 expression after IR will provide new insights into the causal relationship between IR and PD-L1 expression.
Our findings indicate that because CIRT can induce PD-L1 expression, anti-PD-1 antibody therapy may be effective in UCAA patients showing a higher PD-L1 expression post irradiation using C-ion beams. Indeed, a meta-analysis reported that PD-L1 expression in cancer cells is a promising candidate as a selection marker [38]. A combination of CIRT and immunotherapy targeting the PD-L1 pathway may be useful for UCAA patients.
The limitation of this study is that a small number of patients were analyzed. The numbers of UCAA patients received CIRT are still limited in a single institution. One may argue that our cohort in this study might have an older average than the usual for UCAA [39]. Though the correlation between age and PD-L1 expression in cervical cancer is unclear, it is reported that there was no association between bladder cancer patients' age and the expression of PD-L1 [40]. Multi-center study may be needed to obtain definitive results.
In conclusion, we showed that CIRT could enhance the PD-L1 expression in UCAA. We also found that PD-L1 expression could be a possible predictor for PFS in patients with UCAA treated with CIRT. This study warrants further investigation and supports the utilization of immune checkpoint inhibitors with a combination of CIRT for treating patients with UCAA.
 XML Download
XML Download