

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Thyroid-associated orbitopathy (TAO), also known as Graves' ophthalmopathy, is one of the most common autoimmune inflammatory orbital diseases (12). Expansion of extraocular muscles (EOMs) and orbital fat is the most prominent finding, and is responsible for various clinical symptoms, such as proptosis, diplopia, and restricted eye movement (134). Furthermore, the crowding of orbital tissues at the orbital apex as well as increased retrobulbar pressure and optic nerve stretching could result in compressive optic neuropathy, which is the most serious ophthalmic complication of TAO (45). The disease process can be divided into two distinct phases: the active inflammatory phase and the inactive fibrotic phase. Treatment strategies differ significantly between the two phases. Active inflammatory disease is usually considered to be sensitive to anti-inflammatory treatments, while only surgical treatment can rescue the inactive fibrotic disease (13).
Recently, magnetic resonance imaging (MRI) techniques have been increasingly applied in evaluating TAO by virtue of its superior soft tissue contrast with no ionizing radiation (678). Thickness or volume measurements of orbital tissues can help with inspecting the degree of involvement of TAO and can improve diagnostic accuracy (67). Signal intensity on T2-weighted images and contrast-enhanced images can assist in staging and deciding treatment (8). However, the overall accuracy for disease staging is still limited from 55.6% to 71.2% (6789).
Diffusion tensor imaging (DTI), which provides quantitative information about the microstructural integrities of highly oriented tissues, has been increasingly applied for assessing various orbital diseases, such as glaucoma, optic neuritis, and others (10111213). However, studies that apply DTI to assess microstructural changes in TAO patients are still limited (1415), with only two small sample studies (with 20 TAO cases) focusing on EOMs and optic nerves, respectively. Moreover, in previous studies, single-shot echo-planar imaging (ss-EPI) sequences were commonly used for obtaining orbital DTI (1112131415). However, ss-EPI is apt to susceptibility artifacts, such as signal-intensity drop-out, geometric distortion, and overall T2*-induced image blurring, especially in poor magnetic field homogeneity and high field strengths (16). As a potential alternative, readout-segmented EPI (rs-EPI, developed by Porter & Mueller (17)), where k-space is divided into a few, segments along the readout direction, has attracted more attention. It has been proven to be useful for improving image quality along with superior normal anatomical structure distinction, compared to ss-EPI (1618). To our knowledge, no studies have specifically applied rs-EPI-based DTI in the evaluation of TAO until now.
Therefore, our study aims to investigate the ability of rs-EPI-based DTI in assessing microstructural changes of EOMs and optic nerves in TAO patients as well as in evaluating disease activity.
MATERIALS AND METHODS
Patient Population
This study was approved by our Institutional Review Board and the informed consent requirement was waived due to its retrospective nature. From February 2017 to December 2017, 35 consecutive TAO patients who underwent orbital MRI for pre-treatment assessment were enrolled in this study. TAO was clinically diagnosed if eyelid retraction occurred in association with objective evidence of thyroid dysfunction or abnormal regulation, exophthalmos, optic nerve dysfunction, or EOM involvement. If eyelid retraction was absent, thyroid dysfunction associated with exophthalmos, optic nerve dysfunction, or EOM involvement was adopted (19). Patients who had undergone radiotherapy and surgical decompression or had inadequate image quality were excluded.
Disease activity was assessed based on the modified 7-point clinical activity score (CAS) (20) and determined for each eye. The eye was considered in the active phase when CAS ≥ 3 and was otherwise classified into the inactive phase. A total of 38 eyes were defined as active and 32 as inactive. Disease severity was assessed by using the modified 17-point NOSPECS classification (20). Three categories were defined as follows: mild (score from 0 to 3), moderate (4 to 7), and severe (8 to 17). Fifty eyes were classified as moderate, followed by twelve mild and eight severe. No patients were diagnosed with dysthyroid optic neuropathy. Additionally, 22 healthy subjects were enrolled and underwent the same MRI protocol.
Magnetic Resonance Examination
Magnent resonance (MR) scans were performed on a 3T MR scanner (Skyra, Siemens Healthineers, Erlangen, Germany) with a 20-channel head coil. Each person was instructed to look at a fixed site with both eyes closed to reduce motion-related errors. DTI was acquired on an oblique axial plane using an rs-EPI sequence. The imaging parameters were as follows: repetition time (TR)/echo time (TE), 2000/83 msec; field of view (FOV), 220 mm; matrix, 190 × 171; slice thickness, 3 mm; slice number, 10; readout segments, 5; non-collinear gradient encoding directions, 30; b = 0 and 1000 s/mm2. The total imaging time was 5 minutes and 34 seconds.
Conventional imaging protocols included axial T1-weighted imaging (TR/TE, 635/6.7 msec), and axial, coronal, and sagittal T2-weighted imaging (TR/TE, 4000/75–117 msec) with fat suppression. Other parameters were as follows: FOV, 200 mm; matrix, 320 x 320; slice thickness, 3 mm.
Imaging Processing
rs-EPI-based DTI images were postprocessed using DSI Studio software (http://dsi-studio.labsolver.org). The ‘DTI’ reconstruction method was used to model the eigenvectors, and pixel-by-pixel maps of fractional anisotropy (FA), mean diffusivity (MD), axial diffusivity (AD), and radial diffusivity (RD) were then automatically obtained. For placing regions of interest (ROIs) on the EOMs, polygonal ROIs were manually drawn on all consecutive axial slices including the medial and lateral EOMs in each orbit, avoiding the surrounding fatty tissue. We followed a similar method with the optic nerve and carefully positioned polygonal ROIs at the level of the intra-orbital optic nerve (Fig. 1).
All ROIs were drawn independently by 2 neuroradiologists (reader 1: 8 years of experience; reader 2: 4 years of experience) who were blinded to the clinical condition and study design. The measurements of the two readers were used to calculate the inter-observer reproducibility. Additionally, to assess intra-observer reproducibility, reader 1 re-assessed all the DTI images, spaced at least 1 month apart. The average of the two measurements of reader 1 was applied into the statistical analysis.
Statistical Analysis
All numeric data were averaged and reported as the mean ± standard deviation. The chi-squared test was applied to compare differences between sex, medication, smoking history, and disease severity categories between groups. The independent-samples t test was used to compare differences between age, disease duration, and rs-EPI-based DTI parameters of the medial and lateral EOMs as well as the optic nerve between groups. Multivariate logistic regression analysis was used to evaluate the predictive value of significant variables for determining the active phase by using a forced-entry process. The odds ratios and their 95% confidence intervals were calculated. Receiver operating characteristic curve analysis was performed to evaluate the diagnostic efficiency of the identified parameters for the active phase.
Intraclass correlation coefficients (ICC) with 95% confidence intervals were used to evaluate the inter- and intra-observer reproducibility of the measurements, and a two-way ICC with random rater assumption was applied. It was interpreted as follows: < 0.40, poor; 0.40–0.60, moderate; 0.61–0.80, good; ≥ 0.81, excellent. A p value of less than 0.05 indicated statistical significance. All statistical analyses were carried out using the SPSS software package (v. 23.0, IBM Corp., Armonk, NY, USA).
RESULTS
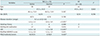
Detailed clinical and demographic information of the study population is displayed in Table 1. There were no significant differences in sex distribution or age between TAO and healthy control (HC) groups and between active and inactive TAOs, nor were there in antithyroid medication or smoking history between active and inactive TAOs (all p > 0.05). The mean disease duration was 6.5 months (range, 2 to 24 months), and it was significantly shorter in active TAOs than inactive ones (4.6 ± 2.3 vs. 8.9 ± 5.9 months, p < 0.001). The mean CAS was 4.6 ± 1.0 in active TAOs and 1.3 ± 0.8 in inactive ones (p < 0.001). The mean modified NOSPECS score was 5.2 ± 2.0 and 5.3 ± 1.3 in active and inactive TAOs, respectively (p = 0.621). A significant difference was found in disease severity categories between active and inactive groups (p = 0.022).
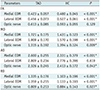
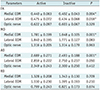
Excellent intra- and inter-observer reproducibility were obtained when measuring all rs-EPI-based DTI parameters (ICC ranged from 0.861 to 0.993). TAO patients showed significantly lower FA and higher MD, AD, and RD than HCs (all p < 0.001) for both the medial and lateral EOMs, except for the AD value of the lateral EOMs (p = 0.619) (Table 2, Fig. 2). Active phase TAO patients had significantly higher FA, MD, and AD (p < 0.005) than those in the inactive phase for the medial EOMs, whereas only FA showed a significant difference regarding the lateral EOMs (p = 0.018) (Table 3, Fig. 2). In the optic nerve, MD, AD, and RD were significantly lower in TAO patients than HCs (all p < 0.05), while FA showed no significant difference (p = 0.129) (Table 2, Fig. 3). Neither FA nor diffusivity differed significantly between active and inactive phases (both p > 0.05) (Table 3, Fig. 3).
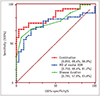
Multivariate analysis showed that the MD of medial EOMs and disease duration were significant indicators for predicting the active phase (p = 0.035, 0.010; respectively), and the FA of medial EOMs demonstrated a nearly significant result (p = 0.05). A higher MD of medial EOMs and shorter disease duration were related to the active phase (β = 10.355, −0.561; respectively). The combination of MD of medial EOMs and disease duration showed optimal diagnostic efficiency for disease activity (area under the curve, 0.855; sensitivity, 68.4%; specificity, 96.9%) (Fig. 4).
DISCUSSION
In this study, almost all the diffusivity values of EOMs were significantly higher in TAO patients than those in HCs, which was in agreement with previous studies (2122). Furthermore, active patients showed significantly higher diffusivity of medial EOMs than inactive patients. Diffusivity measures the magnitude of diffusion of water molecules within the tissue, which is dominated by interstitial space (23). The active phase is histologically characterized by mononuclear cell infiltration, fibroblast proliferation, and edema in EOMs. By contrast, the inactive phase is characterized by interstitial fibrosis, collagen deposition, and fat infiltration (13). As previous studies stated, diffusivity could increase in edematous muscle and decrease in fibrotic and fatty infiltrated tissue (22232425). Therefore, it is not surprising that active patients have higher diffusivity than inactive ones. However, this finding might be contradictory to several prior studies (1421). Politi et al (21). discovered that the normalized diffusivity of EOMs showed a tendency to increase more in the active phase than in the inactive phase, but this was not statistically significant. In another study, diffusivity values of medial EOMs significantly differed only between acute (disease duration ≤ 6 months) and chronic stages, but not between the active and inactive phases (14). A possible reason for this discrepancy might be the more widened gap of CAS values between active and inactive groups in our study than in the previous two studies. Additionally, the usage of semi-quantitative measurement (diffusivity normalized to thalamus) in the previous study might also have an effect.
FA is another widely used DTI parameter. FA measures the fraction of the magnitude of diffusivity, which reflects fiber integrity and is related to the architecture and the strength of the muscle (2627). In our study, EOMs of TAO patients exhibited lower FA than HCs. This is likely associated with cell lysis, fibrous disruption, or loss of EOMs in TAO patients (14). Furthermore, EOMs of active patients had higher FA values compared to inactive ones, which is a unique finding that has not previously been reported. Previously, Cheung et al (25). discovered decreased FA in mild collagen deposition. Abdullah et al (28). also reported decreased FA in diffuse myocardial fibrosis. Considering that fibrosis and subsequent collagen deposition are also characteristic features of EOMs in inactive TAO, it was not unexpected that inactive patients would show decreased FA compared to active patients.
In our study, multivariate analysis along with clinical factors revealed that MD of medial EOMs and disease duration were significant predictors in combination for disease activity with optimal determining efficiency. In addition, FA of medial EOMs demonstrated a marginal significance in predicting the active phase. Therefore, on the basis of our preliminary results, rs-EPI-based DTI derived diffusivity and FA of EOMs, especially of medial EOMs, could be adopted as potential imaging biomarkers for diagnosing TAO and determining activity in patients with TAO.
In terms of microstructural changes in the optic nerve, our study indicated significantly decreased diffusivity in TAO patients compared to HCs, which was consistent with a prior study (15). In addition, Yamada et al (29). found that the diffusivity of the optic chiasm was also decreased significantly in intra- and parasellar tumor patients, and they attributed this change to tumor compression of the optic chiasm starting from the occurrence of the tumor up until treatment. Although the exact mechanisms of dysthyroid optic neuropathy are still not understood, the most widely accepted hypothesis is mechanical compression and ischemia (15). Thus, our present result might also reflect the effects of compression and the relatively long-term change on the optic nerve in TAO patients (29). However, in terms of FA, there is a discrepancy between our study and that of Lee et al (15). They found that FA increased significantly in TAO patients, while our study showed no significance. We thought that this discrepancy might be partially related to the different constitution of patient groups between the two studies. More specifically, patients of a more severe category were included in their study (20%) compared to ours (11%). In addition, changes in FA values under different scan parameters might also be responsible. For instance, an FA value could be larger when applying a smaller voxel size or decreased diffusion gradient directions (3031). Therefore, further research with more unified parameters along with a larger sample size should be performed to clarify the exact change of FA in the optic nerve of patients with TAO.
Our study exhibited good to excellent inter- and intra-observer reproducibility for all measurements of rs-EPI-based DTI parameters. The satisfactory reproducibility might be attributed to the following reasons. First, an rs-EPI sequence was used for the DTI scan. Given that it has been proven to be superior in reducing ghosting artifacts and improving image quality compared to conventional ss-EPI, the better visualization of EOMs and the optic nerve contributes to less measurement bias. Second, as a previous study indicated that inter-observer variability caused by ROI placement could be effectively reduced by a larger ROI approach (32), we used large, polygonal, and strip-like ROIs on consecutive slices, which could objectively represent the overall change of the evaluated subject. By contrast, in previous studies, hot-spot or regional ROIs were usually used for measuring quantitative parameters of EOMs and optic nerves (111233). These ROI selection methods were prone to sampling bias.
Our study has several limitations. First, our study population was relatively small. Second, we didn't conduct post-treatment assessment because this is a retrospective study and complete follow-up information was not available for every patient. However, we believe that our results could be a strong basis for further larger prospective studies. Third, while evaluating EOMs, only the medial and lateral bundles were measured because of the axial scan for the DTI sequence. Lack of information on inferior EOMs might be a major drawback of our study. Additional DTI scans in the coronal plane or even using non-EPI diffusion sequences with less air-bone susceptibility artifacts and distortion would be helpful for assessing all EOMs and the optic nerve simultaneously (3435).
In conclusion, our preliminary results suggest that rs-EPI-based DTI is helpful in detecting microstructural changes of EOMs and optic nerves and can improve the diagnostic accuracy of TAO. rs-EPI-based FA and diffusivity of EOMs, especially the MD of medial EOMs, can serve as an indicator of disease activity.



 XML Download
XML Download