

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Patients with pancreatic adenocarcinoma have a poor prognosis, with overall 5-year survival rates ranging from 0.4–8% (12). Surgical resection is the only form of curative treatment; however, only about 10% of patients are candidates for surgery because of the presence of advanced disease at the time of diagnosis (345). Even after curative surgery, cancer recurrence develops within 1–2 years of pancreatic surgery in over 60% of patients, with extrapancreatic recurrence being most frequently located in the liver (678). Most patients thereby qualify for palliative therapy, including systemic chemotherapy and/or radiation therapy (9). However, such options are of limited benefit as pancreatic carcinomas respond poorly to these treatment modalities (1011).
Percutaneous radiofrequency ablation (RFA) has been recognized as a safe and effective local therapy for primary or metastatic liver malignancies (1213141516171819). As most hepatic metastases recurring after surgery in patients with pancreatic adenocarcinoma are small (≤ 3 cm), percutaneous RFA is usually feasible. A few reports have described the promising outcomes of RFA for treatment of hepatic metastasis from pancreatic adenocarcinoma (202122). In this study, we evaluated the safety and efficacy of percutaneous RFA in 60 patients with 94 metachronous hepatic metastasis, arising after curative resection of pancreatic adenocarcinoma. Further, we compared the survival outcomes of RFA treatment with those of chemotherapy for this specific group.
MATERIALS AND METHODS
Patient Population
Our institutional review board approved this study (AMC 2018-1139), and waived the requirement for patient consent due to the retrospective nature of the study. Patients were deemed eligible for RFA if they had less than five recurrent hepatic tumors from pancreatic adenocarcinoma, tumors ≤ 5 cm in maximum diameter, no evidence of vascular invasion, stable extrahepatic metastases (neither decreasing nor increasing in extent or severity by chemotherapy control) or no extrahepatic disease, and tumors that were detectable by ultrasonography (US) or CT with an acceptable and safe path (22). Patients were excluded if they had a recurrent hepatic tumor > 5 cm in maximum diameter, more than five tumors, an Eastern Cooperative Oncology Group performance status of 2–4, vascular invasion, progressive extrahepatic metastases, or coagulopathy (platelet count < 50 × 103/µL; international normalized ratio > 1.5).
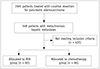
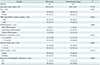
From December 2002 to August 2017, 60 patients (35 men, 25 women; age range, 38–78 years; mean age ± standard deviation [SD], 60 ± 9.1 years) with 94 metachronous hepatic metastases arising from pancreatic adenocarcinoma underwent percutaneous RFA and were included in the present study (Fig. 1). Twenty-eight of the 60 patients have been previously reported (21). Four (6.6%) of the 60 patients with hepatic recurrence and distant metastases received systemic chemotherapy for recurrence prior to RFA. All patients underwent curative resection of their adenocarcinomas, consisting of Whipple surgery in 23 patients, distal pancreatectomy in 20, pylorus-preserving pancreaticoduodenectomy in 15, and total pancreatectomy in two. The stage of the pancreatic ductal adenocarcinoma was classified according to the 8th TNM staging system by American Joint Committee on Cancer. The stages were IA (n = 3), IB (n = 22), IIA (n = 2), IIB (n = 28), and III (n = 5) before the time of curative surgery. The pancreatic adenocarcinomas were well-differentiated (n = 1), moderately differentiated (n = 50), or poorly differentiated (n = 9). For comparisons during the same period, we included 66 patients who received chemotherapy only and met the same eligibility criteria described (Fig. 1). The baseline characteristics of the patients and tumors are summarized in Table 1. The median time between the diagnosis of hepatic metastases and RFA treatment was 0.6 months (range, 1 day–5.6 months). Of the 60 included patients who underwent RFA, 49 had hepatic recurrences only, seven had both hepatic and local recurrences (in the resection areas), and four had hepatic recurrence and distant metastases. Adjuvant chemotherapy was indicated for patients with tumor stages IB or greater taking into account the patient performance status, patient willingness, age, and cost (21). Of the sixty patients, 48 (80%) received adjuvant chemotherapy after curative surgery for pancreatic adenocarcinoma. Tumor sizes ranged from 0.6–5 cm in maximum dimension (median, 1.5 cm). For 17 (28.3%) of the 60 patients, recurrent hepatic tumors were diagnosed histologically according to the results of image-guided percutaneous needle biopsy, while contrast-enhanced CT and/or whole-body positron emission tomography [F-18 Fludeoxyglucose] scans after surgery were used for 43 patients (71.7%).
Radiofrequency Ablation Technique
RFA was performed percutaneously under US, with the patient under conscious sedation (dexmedetomidine 1 µg/kg and remifentanil 1 µg/kg) and local anesthesia with 5–10 mL of 1% lidocaine. Prophylactic antibiotics were not used before the RFA procedure. CT-guided RFA (n = 3) was performed in patients with a poor US window. Artificial ascites using 5% dextrose in water solution was injected in the peritoneal space for 8 patients. Fusion imaging of real time US with CT (n = 3) or MRI (n = 1) was used. A single electrode (ValleyLab, Burlington, MA, USA) (n = 38) or an electrode cluster (ValleyLab) (n = 22) was used, with radiofrequency current being emitted for 12 or 15 minutes using a 200 W generator set to deliver maximum power and employing the automatic impedance control method. Each tumor received 1–4 ablations (mean, 1.5 ablations) per session, according to tumor size and shape. For all tumors ≤ 2 cm in diameter, a single electrode with a 3 cm exposed tip was used (19). For tumors ≥ 2 cm in diameter, a cluster electrode or multiple overlapping insertions of a single electrode were used (19). The endpoint of the RFA was an ablative margin of at least 1 cm (192324). At the end of the RFA procedure, the electrode path was cauterized to prevent bleeding, and tumor seeding during retraction of the electrode.
Follow-Up and Evaluation of Data
All patients were transferred to the CT suite immediately after the RFA procedure, and an immediate post-RFA examination was performed with contrast-enhanced CT, to evaluate success of the ablation, and possible complications. Major complications were defined as any event requiring additional treatment, including an increased level of care, hospital stay beyond observation status (including re-admission after initial discharge), permanent adverse sequelae including substantial morbidity or disability, or death (2526). All other complications were classified as minor. Ablations were considered to be complete, and technical success achieved if the ablation zone completely covered the tumor, and there was no irregular enhancement of the ablated area (26). If residual tumor was present in the ablated area, an additional session of RFA was performed.
Follow-up contrast-enhanced CT was performed one month after ablation and every two-three months thereafter. Repeat RFA was employed to treat local tumor progression, and new intrahepatic focal lesions in patients with less than five tumors with a largest diameter ≤ 5 cm, no vascular invasion, and stable extrahepatic disease.
The terminology and reporting criteria of the Society of Interventional Radiology were used for reporting the follow-up findings (26). Local tumor progression was defined as the appearance of new tumor foci at the edge of the ablation zone, during follow-up contrast-enhanced imaging. Local tumor progression, progression-free survival, and overall survival rates were calculated using the Kaplan-Meier method. Progression-free survival was defined as the time elapsed between treatment initiation, and tumor progression or death from any cause (27). The overall survival periods were measured in months, from the date of diagnosis of hepatic metastasis, and from the time of initial RFA, to a patient's death. The local tumor progression was calculated from initial ablation to the first imaging evidence of local tumor progression. Tumor size was dichotomized relative to the median diameter (1.5 cm), and the local tumor progression curves of study patients were compared, according to the tumor size using log-rank test.
The groups were compared using Student's t test for continuous data and the chi-square (χ2) test for categorical data. Multivariate Cox regression analysis was used to explore possible independent factors (age, sex, TNM stage before curative surgery, pathological grade, tumor number, diameter of the largest tumor, time between surgery and development of recurrence, presence of other metastases outside of the liver) associated with overall survival after RFA. Age, tumor number, and diameter of the largest tumor, were each dichotomized into two groups according to the median values. The time between surgery and development of recurrence was dichotomized into two groups, 1 year or longer and shorter than 1 year (2428), and TNM stage before curative surgery was dichotomized into two groups, ≥ IIB and ≤ IIA. Pathological grade was dichotomized into two groups, well or moderately differentiated, and poorly differentiated. Only variables associated with a p value < 0.1 in the univariable Cox analysis were entered into the multivariable model. Fisher's exact test was used to evaluate the relationship between occurrence of liver abscess and the presence of bilioenteric anastomosis. All statistical analyses were performed using SPSS (version 21; IBM Corp., Armonk, NY, USA). A two-sided p value < 0.05 was considered statistically significant.
RESULTS
Technical Success
Technical success was achieved in 89 of the 94 hepatic tumors (94.6%) after a single session of US (n = 87) or CT (n = 2) guided RFA. In four patients, a residual tumor was detected on immediate follow-up CT, with an additional US guided RFA session then being performed for residual tumors. The one remaining hepatic tumor was not well-delineated on US at the time of RFA, although a residual unablated area was observed on immediate follow-up CT. Secondary RFA under CT guidance was performed on the following day to treat this residual unablated area, resulting in the complete ablation of the residual tumor. The technical success rate of RFA, including additional ablation procedures performed on the same day or a day later, was 100%.
Major Complications
Eight major complications occurred after RFA for 94 tumors (8.5%, 8/94) in 8 of the 60 patients (13.3%, 8/60), although there was no procedure-related mortality. Liver abscesses developed at six ablated areas 3–83 days (median time, 30 days) after RFA. Liver abscesses occurred in 5 of 38 (13.2%) patients with a bilioenteric anastomosis (patients who underwent Whipple surgery or pylorus-preserving pancreaticoduodenectomy), and in 1 of 22 (4.5%) patients without a bilioenteric anastomosis; however, the liver abscesses were not significantly related to the presence of bilioenteric anastomoses (p = 0.399). All six liver abscesses were successfully managed with percutaneous drainage and antibiotic treatment. The remaining two major complications were intraperitoneal hemorrhages that occurred 1 day after RFA of superficially located tumors and required blood transfusion and percutaneous drainage. The major complications in the chemotherapy group were neutropenic fever requiring admission and medical treatment (n = 3), significant cytopenia requiring hold or switch of chemotherapy (n = 7), and severe nausea and vomiting requiring admission and medical treatment (n = 3). The major complication rate between the RFA (13.3%, 8/60) and chemotherapy (19.7%, 13/66) groups was statistically non-significant (p = 0.338).
Local Tumor Progression
During follow-up, local tumor progression of treated lesions was observed in 36 (38.3%) of the 94 tumors, with 5 of these 36 tumors being treated by repeat RFA. The cumulative local tumor progression rates at 6 months, 1 year, and 2 years were 23.3%, 41.2%, and 47.3%, respectively.
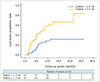
The local tumor progression rates for tumors ≤ 1.5 cm in diameter at 6 months, 1 year, and 2 years after RFA were 12.8%, 28.4%, and 31.5%, respectively, whereas for tumors > 1.5 cm in diameter, the local tumor progression rates at 6 months, 1 year, and 2 years after RFA were 37%, 57.7%, and 66.4%, respectively. The cumulative local tumor progression rate was significantly lower for tumors ≤ 1.5 cm in diameter than tumors > 1.5 cm in diameter (p = 0.001) (Fig. 2).
Overall Survival
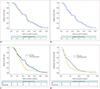
The median follow-up time of the 60 patients in the RFA group, and of the 66 patients in the chemotherapy group was 14.7 (interquartile range, 6.7–17.9 months), and 10.4 months (interquartile range, 7.6–13.4 months), respectively. As of October 2018, 57 of the 60 patients (95%) in the RFA group had died, and 3 (5%) remained alive. Sixty-four of the 66 patients (97%) in the chemotherapy group had died, and 2 (3%) remained alive. The median overall survival periods after RFA and from the time of diagnosis of hepatic metastasis were 12 and 14.7 months, respectively (Fig. 3A, B). The overall survival rates at 6 months, 1, 2, and 3 years after RFA were 75%, 50%, 14.3%, and 0%, respectively, whereas the overall survival rates at 6 months, 1, 2, and 3 years from the time of diagnosis of hepatic metastases in the RFA group were 83.3%, 55%, 16.4%, and 2.1%, respectively. Median overall survival from the initial treatment was higher in the RFA group (12 months) than in the chemotherapy group (9.1 months), but the difference was not statistically significant (p = 0.094) (Fig. 3C). Median progression-free survival from the initial treatment was also higher in the RFA group (5 months) than in the chemotherapy group (3.3 months), but the difference was only marginally significant (p = 0.068) (Fig. 3D).
Multivariate Cox regression analyses showed that the diameter of the largest tumor (hazard ratio [HR], 2.19; p = 0.007), TNM stage before curative surgery (HR, 2.73; p = 0.001), time between surgery and the development of recurrence (HR, 2.26; p = 0.016), and absence or presence of extrahepatic metastasis (HR, 3.37; p = 0.002) were independently associated with overall survival after RFA (Table 2).
During follow-up, 55 of the 60 patients (92%) developed new lesions at other liver sites and/or in distant areas. Of these 55 patients, 14 were treated with RFA, 20 with systemic chemotherapy, three with intra-arterial chemoinfusion, two with systemic chemotherapy and radiation therapy, and one with partial hepatectomy. The remaining 15 patients underwent supportive treatment only (pain or ascites control, biliary drainage).
DISCUSSION
The prognosis for patients with pancreatic adenocarcinoma remains dismal, with reported 5-year survival rates ranging from 0.4–8% (12). Despite treatment by curative resection, local recurrence, and/or liver metastases represent two frequent patterns of recurrence that are largely resistant to current treatments, including chemotherapy and radiation (9293031). Patients with hepatic metastases have a worse prognosis than those with local recurrence, with a shorter survival time (3 months vs. 7 months) (29). Therefore, effective control of hepatic metastasis is an important treatment goal for prolonging survival in such patients (32).
Hepatic resection of metastatic tumors arising from pancreatic adenocarcinoma is an alternative to RFA. However, although surgical resection has been known to be effective in patients with hepatic metastases arising from colorectal, breast, or neuroendocrine primary tumors, the role for hepatic resection in patients with hepatic metastases arising from pancreatic adenocarcinoma is less well defined (33). Hepatic resection of metastatic disease, even if confined to the liver, has been discouraged, largely because of the poor prognosis, and rapid progression of pancreatic adenocarcinoma (33).
To the best of our knowledge, the first application of RFA to the treatment of liver metastasis arising from pancreatic adenocarcinoma was described in a case report by Thomas et al. (20). In this report, percutaneous RFA was performed on one new liver metastasis in a 49-year-old female, who had previously undergone pancreaticoduodenectomy, followed by adjuvant chemoradiation to treat pancreatic adenocarcinoma. RFA was technically successful in this patient, but a large liver abscess occurred 3 weeks later. The abscess was successfully treated by percutaneous drainage, and the patient showed no evidence of either cancer or abscess recurrence 6 months later. This case suggested that RFA can be used to successfully treat hepatic metastases (of limited extent) in patients previously treated for pancreatic adenocarcinoma, but that the incidence of liver abscess is likely to be high because of bilioenteric anastomosis (20).
Park et al. (21) evaluated the clinical feasibility of RFA in 34 patients, with 28 having metachronous hepatic metastasis arising after curative resection of pancreatic adenocarcinoma, and six having a synchronous hepatic metastasis that was detected at the time of surgery. The RFA was performed intraoperatively in the six patients with synchronous hepatic metastasis. All 34 patients had no known metastasis other than to the liver. The median overall survival time from the date of diagnosis of hepatic metastasis was 14 months; however, the authors did not provide overall survival data from the time of RFA. In their multivariate analysis, the diameter of the largest hepatic metastasis (< 2 cm vs. ≥ 2 cm) and the pathology of pancreatic adenocarcinoma (well or moderate differentiation vs. poor differentiation) were significantly associated with overall patient survival from the time of diagnosis of hepatic metastasis. However, the authors did not provide the local tumor progression rate after RFA for each hepatic metastasis.
In the present study, we evaluated the safety and efficacy of percutaneous RFA in 60 patients with 94 metachronous hepatic metastasis, arising after curative resection of pancreatic adenocarcinoma. We found that RFA led to complete tumor necrosis of all 94 tumors (median diameter, 1.5 cm) after one (n = 89) or two (n = 5) sessions of RFA, without any procedure-related mortality. The local tumor progression rate during follow-up after RFA was 38.3%. The cumulative local tumor progression rates at 6 months, 1 year, and 2 years were 23.3%, 41.2%, and 47.3%, respectively. In agreement with previous findings showing that tumor size was significantly associated with local tumor progression after the use of RFA to treat hepatic malignancies (13151934), we found that the local tumor progression rate was significantly lower for tumors ≤ 1.5 cm in diameter than for those > 1.5 cm in diameter (p = 0.001).
We also found overall median survival and 3-year survival rates from the time of initial RFA of 12 months and 0%, respectively, while they were 14.7 months and 2.1%, respectively, from the first diagnosis of liver metastasis. The 14.7 months median survival period we observed (from time of diagnosis) was substantially longer than the 3 months median survival reported for patients conservatively managed for hepatic recurrence, though it is hard to compare directly (2935). In addition, the median overall survival from the initial treatment was also longer in the RFA group (12 months) than in the chemotherapy group (9.1 months) in our study, but the difference was not statistically significant (p = 0.094). However, the present study hinted that a larger study might also find better overall survival in the RFA group than in the chemotherapy group.
In our study, multivariate analysis showed that a large tumor diameter of > 1.5 cm, TNM stage before curative surgery ≥ IIB, a time between surgery and development of tumor recurrence of < 1 year, and the presence of extrahepatic metastasis were all associated with poor overall patient survival from the time of initial RFA. According to our current results, patients with a tumor of small diameter (≤ 1.5 cm), relatively early TNM stage (≤ IIA) before the time of curative surgery, late hepatic recurrence (≥ 1 year after curative resection), and liver-only metastasis benefited most from RFA treatment.
Theoretically, RFA can result in thermal injury to the bile ducts, and can form an inadvertent connection between the biliary tree and the ablation zone. Such ablation zones may become contaminated with enteric bacteria, arriving through bilioenteric anastomoses, thereby resulting in liver abscesses (36). Although we found that liver abscesses after RFA occurred more frequently in patients with (13.2%, 5/38) than without (4.5%, 1/22) bilioenteric anastomoses, the difference failed to reach statistical significance (p = 0.399), probably due to small sample size of our study patients. Thus, monitoring for the possibility of liver abscesses caused by bilioenteric anastomoses must be performed following RFA treatment of hepatic tumors. Further, an aggressive antibiotic prophylaxis regimen in conjunction with routine pre-procedure bowel preparation may provide protection against liver abscesses after locoregional therapy in patients with bilioenteric anastomosis (1937). This issue should be further evaluated in a future study.
This study's limitations include its retrospective nature, which causes it to be vulnerable to a variety of potential biases. Nevertheless, we believe that our results indicate that RFA may play a potential role in the treatment of liver metastases arising from pancreatic cancer, and our data provides support for prospective investigations.
In conclusion, RFA is safe and may offer successful local tumor control in patients with hepatic metastases arising from pancreatic adenocarcinoma. Patients with a tumor of small diameter (≤ 1.5 cm), early TNM stage (≤ IIA) before the time of curative surgery, late hepatic recurrence (≥ 1 year after curative resection), and liver-only metastasis, benefited most from RFA treatment. In our study, RFA provided better survival outcomes than chemotherapy for this specific group with borderline statistical difference.

 XML Download
XML Download