

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hepatocellular carcinoma (HCC) is the sixth most common cancer worldwide, and the third most common cause of death due to cancer (1). Recent advances in imaging technology enable HCC to be diagnosed without biopsy if a tumor nodule is greater than 1 cm in diameter and shows typical arterial enhancement with delayed washout on dynamic computed tomography (CT) or magnetic resonance imaging (MRI). However, it is still difficult to make a correct diagnosis using imaging techniques or biopsy for sub-centimeter-sized HCCs, because diagnostic accuracy decreases with the diminishing size of nodules due to false-positive results, such as small hemangiomas, regenerative nodules, arterioportal shunts, and inadequate specimens (2345678). Diagnosis using thin-section, whole-explant correlation following transplantation has been established as a standard reference to diagnose HCC; however, it remains a treatment option for only a limited number of patients (910). In addition, a complete correlation between pathology and imaging findings is difficult to perform in clinical practice. Consequently, the characteristics or behavior of sub-centimeter-sized HCCs are not well understood.
Early diagnosis of HCC remains important for improving the disease prognosis. The development of cone-beam computed tomography (CBCT) using a flat-panel detector has increased the detection of hypervascular HCC nodules, when used in conjunction with standard digital subtraction angiography (DSA), during transcatheter arterial chemoembolization (TACE) (111213). CBCT-hepatic arteriography (CBCT-HA) can better visualize tumor-feeding vessels, as well as provide better information regarding tumor vascularity, as compared with CT, because it provides high lesion-to-background contrast and spatial resolution (1415161718).
This study proposes a novel reference standard for hypervascular HCC, established by CBCT-HA and two-year imaging follow-up, and discusses its clinical implication on tumor staging and understanding the intrahepatic distant recurrence (IDR) in relation to dynamic CT.
MATERIALS AND METHODS
Patient Selection
The present study was retrospective in nature, which was approved by our Institutional Review Board, and the informed consent was waived. The study included 276 patients suspected of having HCC, on the basis of the clinical presentation and radiologic findings, and who were referred to undergo their first TACE treatment, between June 2009 and June 2010. A total of 89 patients were excluded (54 patients who underwent CT at an outside hospital, 25 patients who underwent CT with more than a two-month interval between TACE, and 10 patients with inadequate dynamic CT protocol). We then selected 187 patients who underwent dynamic liver CT at our hospital, less than two months before TACE. We also excluded 22 patients with diffuse HCC (n = 9), more than 10 HCC lesions (n = 5), portal vein thrombosis (n = 3), or extrahepatic metastasis (n = 5), as seen on initial CT. With regard to performing CBCT-HA before chemoembolization, we excluded 51 patients that required multiple injections for whole-liver scanning, due to a separate hepatic arterial supply. In addition, we also excluded 11 patients with blurring on CBCT-HA images, due to motion artifact. Of the remaining 103 patients, we excluded four patients who did not undergo chemoembolization in the initial session, due to the absence of hypervascular HCC seen on CBCT-HA. Therefore, the final study group consisted of 99 patients (81 men and 18 women; mean age 63.6 ± 8.3). The mean time interval between initial CT and the CBCT was 19 days (0–59 days).
Clinical Follow-Up
In all 99 patients, dynamic liver CT was performed every three months, in addition to the clinical surveillance used to detect tumor recurrence after the initial TACE. During the two-year follow-up period, if a hypervascular HCC was newly suspected, TACE was performed with CBCT assistance in routine clinical practice. Laboratory data included aspartate transaminase, alanine transaminase, albumin, total bilirubin, prothrombin time/international normalized ratio, and platelet count. The serum tumor marker alpha-fetoprotein (AFP) level was also evaluated every three months, in addition to radiologic examinations.
CBCT Techniques
TACE procedures were performed using a CBCT-capable angiography unit (AXIOM Artis dTA/VB30, Siemens Healthineers, Erlangen, Germany), with a 30 × 40 cm, flat-panel detector. Before C-arm scanning, selective arterial DSA of the celiac trunk or common hepatic artery was performed (5-Fr RH catheter, Cook, Bloomington, IN, USA), to examine the vascular anatomy and blood flow. Following DSA, C-arm CT images of the hepatic artery were obtained during a single breath-hold, and with 211° of circular trajectory, for eight seconds (5-Fr RH catheter; 4-Fr Glidecath, Terumo, Tokyo, Japan; 2.7-Fr Radio Star, Taewoong Medical Co., Gimpo, Korea; 2.4-Fr MicroFerret, Cook). Contrast-enhanced images were acquired using undiluted, iodinated contrast medium (iopamidol; Pamiray 300, Dongkook Pharmaceutical, Seoul, Korea), at a flow rate of 1.5–6 mL/s for 12 seconds, with a 4- or 6-second x-ray delay. The CBCT-HA acquisition protocol was: 0.5° increment; 512 × 512 matrix in projections; 210° total angle at approximately 26° per second; a system dose of approximately 0.36 µGy per frame; and a total of 419 projections. The raw datasets from the angiography system were transferred to a dedicated external workstation (Leonardo with DynaCT, Siemens Healthineers), where the two-dimensional axial, coronal, and sagittal multiplanar reformation images were reconstructed with 1-mm slice thickness and three-dimensional volume-rendering, or where the maximum intensity projection images were reformed.
Novel Reference Standard to Identify Hypervascular HCCs at the Initial and during the Follow-Up Period
In order to confirm hypervascular HCCs, two radiologists (with 20 years of clinical experience in interventional radiology, and with 4 years of clinical experience in radiology) retrospectively reviewed all CT and CBCT-HA images at the initial presentation, as well as consecutive CT, MRI, and CBCT-HA images obtained during a two-year follow-up period, by consensus opinion. In addition, the same radiologists retrospectively reviewed the formal reports of all 99 patients, in order to evaluate whether the diagnosis of HCC was made in the initial dynamic CT.
The two ways to identify HCC at the initial presentation were as follows. First, we evaluated whether the compact iodized oil uptake was observed on consecutive follow-up CT scans for hypervascular nodules presented on the initial CT or CBCT-HA, and treated with TACE at the initial session. A nodule was considered HCC if nodular iodized oil uptake was continued for at least one year of follow-up. Second, we reviewed the initial CBCT-HA images and determined whether a hypervascular focus was pre-existing at the recurrence site for IDR developed during a two-year follow-up period. Matched pre-existing hypervascular foci on CBCT-HA were considered HCCs at the initial presentation with interval growth. IDR was defined as the development of new lesions that were not detected in initial dynamic CT, and was determined from confirmative findings in subsequent dynamic CT or MRI, and treatment with TACE.
HCC Categorization Based on Mode of Detection
On the retrospective review of formal reports of the initial dynamic liver CT, the two radiologists categorized initial i.e., HCCs into three groups, based on the mode of detection for HCC (i.e., how and when HCCs were detected during clinical and imaging follow-up). Group I consisted of nodules reported as definite or probable HCCs on initial dynamic CT. Group II consisted of HCCs additionally detected on CBCT-HA, and treated with CBCT-assisted TACE. Group III consisted of HCCs that pre-existed as hypervascular foci on initial CBCT-HA, and showed interval growth on follow-up CT or MRI. Group III HCCs were suspected after interval growth during the follow-up period, and were subsequently treated with TACE (Fig.1).
Impact of CBCT-HA and Two-Year Clinical Follow-Up on Initial Tumor Stage and IDR
We assessed the influence of CBCT-HA and two-year clinical follow-up on initial tumor stage (American Joint Committee on Cancer/Union for International Cancer Control [AJCC/UICC] tumor, node and metastasis [TNM] staging system and Milan criteria) (1920). We also analyzed IDR that occurred during the two-year follow-up period. For all IDR nodules, we sought to identify HCCs presented in the initial CBCT-HA, and to calculate the proportion of IDR that pre-existed in the initial CBCT-HA.
Statistical Analysis
The basic clinical characteristics and radiologic evaluation of patients were described as the mean value, with standard deviations and frequencies. All statistical analyses were performed using Statistical Package for Social Science (SPSS version 19.0, IBM Corp., Armonk, NY, USA).
RESULTS
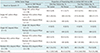
The baseline characteristics of the 99 patients are summarized in Table 1. During two-year follow-up, a total of 405 nodules, except for disseminated recurrence in five patients, were confirmed as hypervascular HCCs. Of the total 405 HCCs, 297 HCCs in 99 patients were identified as present in the initial examination, and 108 HCCs occurred de novo during the follow-up period. Of the initial 297 HCC lesions in 99 patients, 40 patients had a single lesion, 24 had 2 lesions, 11 had 3 lesions, 7 had 4 lesions, 14 had 5 to 10 lesions, and 3 had more than 10 lesions on CBCT-HA. Of the total 297 initial HCCs, 142 (47.8%) lesions were larger than or equal to 1 cm and 155 (52.2%) lesions were smaller than 1 cm. The mean diameter of all HCCs was 13.3 ± 12.3 mm.
HCC Categorization Based on Mode of Detection
Of the 297 HCCs, 149 (50.2%) lesions in 92 patients were Group I lesions, detected on initial dynamic CT, and treated with TACE; 74 (24.9%) lesions in 24 patients were Group II lesions, additionally detected on CBCT-HA, and treated with TACE; and the remaining 74 (24.9%) lesions in 39 patients were Group III lesions that pre-existed as hypervascular foci on initial CBCT-HA, and showed interval growth on follow-up CT or MRI (Table 2, Fig. 2). The mean diameter of each group of HCCs was 19.1 ± 14.9 mm (Group I), 8.2 ± 3.3 mm (Group II), and 6.4 ± 2.9 mm (Group III). The average HCC size after the interval growth of Group III HCCs was 11.4 mm, and the mean growth interval was 10.1 ± 6.8 months. Figure 3 illustrates an example of a patient with both group I, II, and III nodules.
Based on the dynamic CT, the initial T stages of HCC for all patients were T1a in 45 patients, T1b in 20 patients, T2 in 31 patients, and T3 in 3 patients. According to Milan criteria, the initial stages were single HCC within Milan in 61 patients, single HCC beyond Milan in 4 patients, multiple HCCs within Milan in 24 patients, and multiple HCCs beyond Milan in 10 patients.
Impact of CBCT-Based Novel Standard on Initial Tumor Staging and IDR
The initial T stages based on CBCT-HA with Group II lesions were T1a in 35 patients, T1b in 19 patients, T2 in 41 patients, and T3 in 4 patients. According to Milan criteria, the initial stages were single HCC within Milan in 50 patients, single HCC beyond Milan in 4 patients, multiple HCCs within Milan in 34 patients, and multiple HCCs beyond Milan in 11 patients. T stages were changed from T1a to T2 in 10 patients, from T1b to T3 in 1 patient, and Milan criteria were changed from within to beyond in 4 patients, in comparison with initial CT staging.
Based on our reference standard including Group II and III lesions, the initial T stages were T1a in 23 patients, T1b in 17 patients, T2 in 54 patients, and T3 in 5 patients. By Milan criteria, the initial stages were single HCC within Milan in 38 patients, single HCC beyond Milan in 2 patients, multiple HCCs within Milan in 30 patients, and multiple HCCs beyond Milan in 29 patients. T stages were changed from T1a to T2 in 20 patients, from T1b to T2 in 2, and T1b to T3 in 2. By Milan criteria, 17 patients changed from within to beyond the criteria.
According to our definition of IDR (new lesions not detected in initial dynamic CT), including Group II, III, and de novo HCCs, the number of IDR lesions was 148 in 50 patients and 256 in 68 patients during the one-year and two-year follow-up, respectively. Among the IDR lesions, 120 (81.1%) of one-year IDR (n = 148) and 148 (57.8%) of two-year IDR (n = 256) were present in the initial CBCT-HA (Table 3).
If IDR is alternatively defined as the development of new lesion after initial TACE, the 74 lesions in Group II should be excluded from IDR lesions. According to this definition, the number of IDR lesions was 74 in 42 patients and 182 in 64 patients during one-year and two-year follow-up, respectively. Among the IDR lesions by excluding Group II lesions, 46 (62.2%) of one-year IDR (n = 74) and 74 (40.7%) of two-year IDR (n = 182) were present in the initial CBCT-HA.
Table 3 summarizes the initial stages according to the dynamic CT and CBCT-based novel standard, and the proportion of pre-existing HCCs in initial CBCT-HA to IDR.
DISCUSSION
The current study demonstrated the role of CBCT-HA in depicting additional HCC lesions to CT, during the initial chemoembolization session. Using CBCT-HA, 74 (24.9%) HCC lesions (Group II) were additionally detected and treated at initial TACE, and another 74 (24.9%) lesions (Group III) were confirmed to be HCCs with interval growth during two-year clinical follow-up. Previous studies have reported that CBCT showed diagnostic accuracy, comparable or superior to dynamic CT (2122). Iwazawa et al. (22) showed that CBCT depicts hypervascular HCCs smaller than 10 mm in diameter more accurately than biphasic multidetector computed tomography (MDCT) (Az = 0.830 vs. 0.618, p < 0.001). Higashihara et al. (21) also reported that the mean area under the alternative free-response receiver operating characteristic did not differ significantly between MDCT and CBCT (mean Az, 0.83 vs. 0.85, p = 0.32). In their reports, the standard of reference for HCC was based on the findings of accumulation of iodized oil in a tumor seen on unenhanced CT. In our study, because of applying two-year follow-up results to the initial CBCT-HA findings, additional HCCs could be diagnosed. Therefore, our reference standard for HCC using CBCT-HA and two-year clinical follow-up has been proven to have the potential to depict early-stage subclinical HCCs.
Our study results indicate that adding CBCT-HA may have a clinical impact on tumor staging, and further affect the therapeutic decision-making at the initial diagnostic workup. After applying CBCT-HA findings to CT, progression in the initial T stage was found in 11 patients, and change in the Milan criteria was found in 4 patients. These results suggest that changes in tumor staging due to additional nodules seen on CBCT-HA during chemoembolization, would affect patient prognosis and long-term survival. Regarding the initial staging analyses of HCC, recent studies have reported the usefulness of gadolinium ethoxybenzyl-diethylenetriaminepentaacetic acid (Gd-EOB-DTPA)-enhanced MRI, on staging and decision-making regarding treatment options for HCC (232425). In the study by Jin et al. (23), new HCC lesions were additionally detected by Gd-EOB-DTPA-enhanced MRI in 17.3% of patients. In addition, the HCC stage has been reported to be revised in 11.5% of patients after Gd-EOB-DTPA-enhanced MRI using the Barcelona Clinic Liver Cancer staging system (26). Yoo et al. (24) also reported that 33.3% of treatment decisions were changed after additionally using Gd-EOB-DTPAenhanced MRI in patients with early-stage HCC. In their study, 12.1% of patients eligible for liver transplantation exceeded the Milan criteria, after detecting additional HCC by Gd-EOB-DTPA-enhanced MRI. Similarly, our study results demonstrated that 11% of patients changed in the initial T stage and 4% of patients changed in Milan criteria after using CBCT-HA due to the detection of small, barely visible intrahepatic HCC on CT.
In our study, CBCT-HA during TACE with two-year imaging and clinical follow-up allowed the establishment of novel reference standard for hypervascular HCC, which included many sub-centimeter-sized HCCs which pre-existed initially, but clinically manifested as IDR on CT. This study helps to understand the nature of IDR and early stage HCC development. Our study showed that 120 of 148 (81.1%) and 148 of 256 (57.8%) of IDR during the one-year and two-year follow-up already existed on initial CBCT-HA, respectively. In theory, intrahepatic recurrence of HCC is attributable to two different mechanisms: metastasis in the early phase, and de novo primary HCC in the late phase. A previous study by Imamura et al. (27) reported that different variables associated with metastatic recurrence were responsible for early (< 2 years) phase recurrence; however, those related to elevated carcinogenesis contributed to late (≥ 2 years) phase recurrence, that also provided epidemiological evidence for the hypothesis. Our study results suggested that a large proportion of the HCCs, which were considered intrahepatic recurrences by metastasis in the early phase, may have been present initially without demonstration in conventional CT.
This study had several limitations. First, a selection bias was inevitable due to the retrospective design; our patient population had at least one possible HCC lesion suspected at the prior surveillance examination. Second, a pathologic confirmation for the diagnosis of HCC was not used in our study. Instead, we established the novel reference standard for the diagnosis of HCC using CBCT-HA, and long-term follow up data with typical imaging features observed in dynamic CT or MRI after interval growth, and persistent iodized oil uptake after TACE, in addition to elevated AFP. No pathologic proof was provided; however, we assumed that methods established for the diagnosis of HCC, including pre-existing hypervascular foci, would be the only practical methods used in a clinical setting. Third, extrahepatic collateral supplying HCC was not depicted on CBCT-HA because of the intra-arterial injection of contrast media into the common hepatic artery, and a limited field of view of CBCT; consequently, we excluded patients with multiple injections required for whole liver scanning. Furthermore, the motion artifact more severely affects the quality of CBCT-HA than MDCT images. These limitations could decrease the performance of CBCT-HA; however, they can be overcome in clinical practice by a careful search for extrahepatic collaterals together with adequate patient cooperation. Last, IDR can alternatively be defined as the development of new lesion after initial TACE from a clinical point of view, as described in the Results section. Therefore, further research is needed on this different interpretation of IDR.
In conclusion, CBCT-HA during chemoembolization with two-year imaging and clinical follow-up allowed the establishment of novel reference standard for hypervascular HCCs. The high spatial and contrast resolution of CBCT-HA enabled the confirmation of many sub-centimeter-sized, faintly vascularized HCC nodules that pre-existed initially, but clinically manifested as IDR. These factors help in understanding the nature of IDR and the early development of HCC, as well as the clinical implications of changes in tumor staging and treatment decision.





 XML Download
XML Download