

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Image-guided core needle biopsy (CNB) is considered the gold standard diagnostic modality for breast lesions and a reliable alternative to surgical excisional biopsy (12345). Many studies have reported that percutaneous ultrasonography (US)-guided CNB has several advantages over stereotactic or surgical biopsy. It is less invasive, less expensive, and faster to perform; further, it can be performed in real time while still allowing accurate assessments without exposure to ionizing radiation (467). Many studies also have proven that US-guided 14-gauge CNB provides optimal diagnostic information for breast lesions with low fals-enegative rates and accuracy comparable to that of surgical biopsy (3568). Furthermore, the number of breast imaging studies utilizing screening mammography and US has increased, resulting in increased lesion detection and biopsy recommendation. Therefore, US-guided CNB has been increasingly performed since its introduction. However, its subsequent utilization has led to concerns about an unnecessary increase in the number of biopsies associated with benign biopsy results.
In the United States, more than 1 million breast biopsies are performed annually, and approximately 80% of cases are benign (910). However, data are limited on which lesions have been increasingly biopsied over time. US-guided CNB would be cost-ineffective and would be of clinical insignificance if the increasing number of biopsies does not lead to increased breast cancer detection. With the number of total biopsies increasing over time, the malignancy rate in the results of CNB must be kept constant or increase in order to ensure that unnecessary biopsies are not performed.
The purpose of this study was to examine annual trends in breast lesion characteristics (e.g., lesion size, the Breast Imaging-Reporting and Data System [BI-RADS] category established by the American College of Radiology, and pathologic findings) and the malignancy rate based on a large series of US-guided CNB over a 12-year study period.
MATERIALS AND METHODS
Study Population
This study was conducted with the approval of the Institutional Review Board (4-2019-0636), and the requirement for informed consent was waived.
From January 2005 to December 2016, 22667 consecutive US-guided 14-gauge CNBs for breast lesions from 211986 breast US procedures were performed at our institution. We retrospectively reviewed the biopsy results to analyze the annual trends in US-guided CNB. Proven malignancies assessed as BI-RADS category 6 lesions (n = 282), male patients (n = 62), and lesions with non-diagnostic pathologic results (e.g., adipose tissue only or cell paucity) (n = 26) were excluded from this study. Finally, a total of 22297 breast masses of 17241 patients (mean age, 45.7 ± 11.6 years; range, 11 to 92 years) were included in this study.
Biopsy Procedure
US-guided 14-gauge CNB was performed using the free-hand technique and a high-resolution US unit with 5–15-MHz linear transducers (HDI 5000 or 3000 or iU22, Philips' Advanced Technology Laboratories, Bothell, WA, USA; or LOGIQ 9 or LOGIQ E9, GE Healthcare, Milwaukee, WI, USA). Each procedure was performed with the patient in the supine position under local anesthesia. A 14-gauge automated core biopsy needle with a spring-loaded biopsy gun (Promac 2.2 L, Manan Medical Products, Northbrook, IL, USA), a 14-gauge Tru-Cut needle with a 22-mm throw (SACN biopsy needle; Medical Device Technologies, Gainesville, FL, USA), or a 14-gauge dual-action semiautomatic core biopsy needle with a 22-mm throw (Stericut with a coaxial needle, TSK Laboratory, Tochigi, Japan) was used. All biopsies were performed by one of 42 radiologists with less than 2 years of experience who was in fellowship training, or by one of six radiologists with 2 or more years of clinical experience who was a specialist in breast imaging and biopsies. At least four or five core samples per lesion were routinely obtained.
Data Analysis
The radiological and pathologic findings of US-guided 14-gauge CNB were obtained from medical records. Breast lesions were classified based on the lesion size, BI-RADS category on US, and pathologic results of CNB. Each variable was categorized as follows: lesion size as ≤ 10 mm, >10 to ≤ 20 mm, >20 to ≤ 30 mm, >30 to ≤ 40 mm, or > 40 mm; BI-RADS category on US (category 1 to 5); pathologic results of CNB as benign (neither malignant nor high-risk), high-risk (e.g., atypia, including atypical ductal hyperplasia, lobular neoplasia, radial sclerosing lesions, and possible phyllodes tumors), or malignant (e.g., ductal carcinoma in situ [DCIS] and invasive cancer). The malignancy rates for DCIS and invasive cancer were calculated as proportions among all biopsied breast masses of DCIS and invasive cancer, respectively, diagnosed using US-guided 14-gauge CNB. The total malignancy rate was calculated as the total proportion of both DCIS and invasive cancer among all biopsied cases.
To assess overall trends over time in CNB based on the lesion size, BI-RADS category, and pathologic results, the Mantel-Haenszel chi-square test and Poisson regression analysis were performed. The Cochran-Armitage test was performed for trends in the malignancy rate and the Cochran-Mantel-Haenszel test was performed to adjust variables. A generalized linear model with an identity link for normal distribution was used to calculate the odds ratio (OR) for associations between the calendar year and each variable. OR was interpreted as the number of times each indicator increased each year. Analyses were performed with a computerized statistic program (SAS, version 9.4, Cary, NC, USA or SPSS, version 23.0, IBM Corp., Armonk, NY, USA), and a p value of less than 0.05 was considered statistically significant.
RESULTS
Time Trends in CNB Based on the Lesion Size, BI-RADS Category, and Pathology
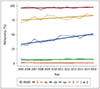
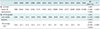
Both the total number of US scans and US-guided CNBs increased significantly during the study period while the proportion of US-guided CNBs to the total number of US scans decreased 0.952 times per year (OR = 0.952 per year, 95% confidence interval [CI]: 0.948, 0.956, p < 0.001) (Table 1). Table 2 shows distributions of US-guided 14-gauge CNB based on the lesion size and BI-RADS category. Table 3 shows the distribution of US-guided 14-gauge CNB based on the pathologic results. Figure 1 illustrates distributions US-guided 14-gauge CNB based on the lesion size, BI-RADS category, and pathologic results. With the Poisson regression analysis, we found statistically significant trends in all variables (p < 0.001, respectively), except for BI-RADS categories 1 and 2. BI-RADS category 3 lesions showed a statistically significant decreasing trend of 0.979 times per year (95% CI: 0.970, 0.988; p < 0.001). The number of BI-RADS category 1 or 2 lesions also decreased to 0.951 times per year without statistical significance (95% CI: 0.902, 1.002; p = 0.058), and the rest of the variables showed an increasing trend over time. Among all biopsied cases, the proportion of high-risk and DCIS lesions increased while the proportion of benign lesions decreased over time (Fig. 2).
Unadjusted and Adjusted Time Trends in the Malignancy Rate
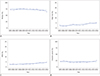
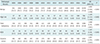
For the malignancy rate, the unadjusted results showed significantly increasing trends in rates of total malignancy (p < 0.001), DCIS (p < 0.001), and invasive cancer (p = 0.039). After adjusting for the BI-RADS category, the increasing trends in rates of total malignancy (p < 0.001) and DCIS (p < 0.003) remained significant, but the rate of invasive cancer did not show a statistically significant increasing trend (p = 0.215). Figure 3 shows the time trend line (by linear regression) in the rate of total malignancy based on the BI-RADS category. The increasing trends in the malignancy rate were statistically significant in BI-RADS categories 4a (p < 0.001), 4b (p = 0.001), and 4c (p = 0.046) for DCIS, BI-RADS category 4b (p = 0.024) for invasive cancer, and BI-RADS categories 4a (p = 0.020), 4b (p < 0.001), and 4c (p = 0.002) for total malignancy (Table 4).
DISCUSSION
Our results show that in a large series (n = 22297) of US-guided CNBs for breast lesions, the overall number of both US scans and US-guided CNBs increased from 2005 to 2016. The increase in the total number of US scans performed may partly contribute to the increase in the number of biopsies; however, the proportion of US-guided CNBs among the total number of US scans decreased over time. One possible reason for this proportional decrease is revisions made to BI-RADS during the study period. The 5th edition of BI-RADS released in 2013 had several changes in the US section to include newer technology, such as elastography, and some additional descriptors in its lexicon (1112). There were several studies in which additional sonoelastography led to downgrading of BI-RADS 4a masses, potentially reducing the number of unnecessary biopsies (131415). In our study, the decreasing rate of biopsies over time might be partly attributed to efforts made to reduce the number of unnecessary biopsies with various novel techniques, such as elastography.
Our analysis revealed that only BI-RADS category 3 lesions decreased significantly over time in terms of both the total number and percentage (26.7% in 2005 to 7.6% in 2016) among the total biopsied lesions. The total malignancy rate among BI-RADS category 3 lesions remained at approximately 1% throughout the study period. This observation is encouraging as otherwise there might have been more unnecessary patient cost and anxiety caused by biopsy because of the high rate of benign lesions in the biopsy results for BI-RADS category 3 lesions. One possible explanation for this may be the efforts to downgrade BI-RADS category 3 lesions by radiologists at our institution. Since March 2010, we have trained our radiologists to downgrade certain lesions found using supplemental screening US to BI-RADS category 2 in efforts to reduce the false-positive rate (16). In a previous study, the downgrade criteria reduced the BI-RADS category 3 rate from 28.3% to 12.6% without loss of cancer detection, and the biopsy rate also decreased significantly over 3 years. Despite using different inclusion criteria in the two studies, our results showed that the decrease in the BI-RADS category 3 rate was most prominent and persistent from 2011 to 2016, which fit the timeframe in which the downgrade criteria were first incorporated into the clinical practice at our institution.
The total malignancy rate in the results of US-guided CNB slightly increased over time with statistical significance, and this trend persisted after adjusting for the BI-RADS category. These results were consistent with our initial assumption that the malignancy rate in the results of CNB should be constant or increase in order to ensure that unnecessary biopsies were not performed. Among cases of total malignancy, the rate of DCIS showed an increasing trend during our study period. This observation can be attributed to the widespread use of screening mammography, which reveals clinically occult pre-invasive disease, and advances of other diagnostic imaging modalities, such as US and magnetic resonance imaging (171819). In addition, improved resolution and technique have enabled visualization of microcalcifications on US, thus increasing the detection rate of DCIS using US-guided biopsy, which was formerly diagnosed using stereotactic-guided biopsy (202122).
When lesions were classified based on the BI-RADS category, the total malignancy rates of BI-RADS category 4a, 4b, and 4c lesions showed slightly increasing trends over time. Because BI-RADS category 4 on US indicates a lesion suspected with malignancy for which biopsy is recommended, the aforementioned result may correlate with decreased false-positive results in the US findings of breast lesions. Our results showed that the malignancy rate based on the BI-RADS category generally matched the stratification of positive predictive values for each BI-RADS category during the past 12 years, with an exception in year 2008 (92.9% in BI-RADS 5). BI-RADS suggests a positive predictive value of less than 2%, 3–10%, 11–50%, more than 95% for categories 3, 4a, 4b, 4c, and 5, respectively (11).
In 2005, a community population-based trend study was performed on the frequency and malignancy rate of breast biopsies, similar to our study (23). However, many subjects of this past study underwent surgical biopsies, which are no longer recommended as the initial diagnostic approach (24). In addition, unlike our study, there was no BI-RADS classification for US lesions, which is now used in clinical practice. Thus, our study better reflects the latest clinical management approaches chosen for breast lesions compared with the previous study. Another recent study described time trends in minimally invasive breast biopsy for 9 years (25); however, this study primarily analyzed geographic/ethnic variations in breast biopsy and did not assess malignancy rates relating to unnecessary biopsies and cost-ineffectiveness in the clinical practice, while our study focused on the malignancy rate of breast biopsies.
Our study has a few limitations. First, this study was retrospectively conducted at a single tertiary hospital; therefore, its results cannot be generalized immediately to other populations. Further multicenter studies are required before our results can be applied to general clinical circumstances. Second, there was no standard diagnostic reference, such as surgical excision or follow-up data, to confirm the pathologic results of CNB. However, US-guided 14-gauge CNB is a reliable diagnostic modality that allows accurate assessments (467). A previous study at our institution showed reliable sensitivity (95.4%) and no false-positive results for US-guided CNB from 2005 to 2012 (8). Third, we did not classify US-guided CNB based on the indication of biopsy (e.g., screening or diagnostic clinical setting), which would potentially affect trends.
In conclusion, we found an overall slightly increasing trend in the malignancy rate in the results of US-guided 14-gauge CNB for breast lesions and an increase in the total number of biopsies performed from 2005 to 2016. This trend persisted after adjusting for the BI-RADS category. We could also observe the efforts made to avoid unnecessary biopsies during the 12-year study period with a large population at a single institution.



 XML Download
XML Download