

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Implant installation in the anterior maxillary area is a challenging procedure for clinicians because of its high functional and aesthetic demands. Meticulous treatment planning is necessary to achieve ideal positioning of the implant fixtures [1]. The maxillary incisive papilla, which is situated above the incisive foramen, is an important landmark for arranging the teeth and for providing upper anterior anesthesia [23]. The incisive foramen has a long oval shape, and its diameter varies from 2 mm to 1 cm [456]. In addition, it leads upwards to the incisive canal, through which the nasopalatine nerve and artery descend to the incisive foramen [78].
The incisive foramen is located posterior to the central maxillary incisors, near the midline of the palate [9]. Alveolar bone resorption in the anterior maxilla has been reported to increase after extraction; consequentially, thin residual bone and an enlarged incisive foramen are factors that make implant placement difficult in the region of the maxillary central incisors [101112].
In general, serious complications resulting from surgical injury to the maxillary incisive papilla and incisive canal have not been reported. However, hematoma has been reported 1 week after tooth extraction [13]. Additionally, altered sensation has been detected during the first week after damage of the nasopalatine nerve, but the nerve recovered its normal function within 1 month [14]. However, although unlikely, contact between the nervous tissue and an implant could potentially lead to unsuccessful osseointegration [5].
In order to mitigate the aforementioned risk, it is necessary to assess the location and shape of the incisive foramen prior to implant placement. The aim of this study was to compare the diameter of the incisive foramen and the horizontal and vertical distance from the alveolar bone to the incisive foramen with and without the central incisors by analyzing data collected using cone-beam computed tomography (CBCT).
MATERIALS AND METHODS
This retrospective study included patients who underwent CBCT imaging for various reasons between January 2011 and June 2017. Only patients older than 20 years were included, as the growth of the maxilla and mandible is completed around the age of 20 [15]. The study protocol was approved by Daejeon Dental Hospital at Wonkwang University (approval No. W1717/001-001). Inclusion and exclusion criteria were as follows:
Inclusion criteria
1) Patients who underwent CBCT imaging with a 102×102 mm field of view
2) Patients who were over 20 years old
Exclusion criteria
1) Patients who received implant surgery at the maxillary incisor site
2) Patients with low-quality imaging, such as scattering along bony borders
3) Patients with suspected pathological lesions, such as cysts, in the anterior maxillary region
Patients were divided into 2 groups: patients with central incisors and patients without at least one central incisor.
Measurement of incisive foramen diameter, horizontal bone thickness anterior to the incisive foramen, and vertical bone height coronal to the incisive foramen
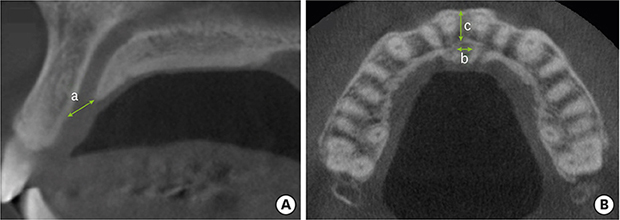
The anteroposterior diameter of the incisive foramen was measured by defining the length of the line connecting the border of the incisive foramen on the mid-sagittal cross-section where the middle of the incisive canal was observed. To assess the anterior maxillary bone thickness, we measured the distance from the anterior point of the incisive foramen to the buccal border of the alveolar crest. The mediolateral diameter of the incisive foramen on the axial plane was measured (Figure 1). The axial cross-section to be used for measurements was selected as the first slice that revealed the intact palatal wall of the incisive foramen when scanning from bottom to top. Lastly, the height of the alveolar bone to the anterior border of the incisive foramen on the sagittal plane was measured (Figure 2). A single researcher took all measurements. Intraexaminer consistency was determined to have a kappa value of 0.96, demonstrating a high level of reliability. The person who measured the diameter and distance did not participate in the statistical analysis. CBCT images were acquired using an Alphard device (Asahi Roentgen, Kyoto, Japan), with a 102×102 mm field of view, tube voltage of 80 kV, current of 85 mA, exposure time of 17 seconds, and slice thickness of 1 mm. The images were transformed using a PACS system (PiView STAR™; INFINITT, Seoul, Korea). The examiner analyzed the CBCT images using a monitor with 1,280×1,024 screen resolution under room lighting.


Statistical analysis
Data were analyzed using SPSS version 18.0 for Windows (SPSS Inc., Chicago, IL, USA). Mean values and standard deviations were obtained for all measurements. Homogeneity of variance was validated using the Levene test, and it could therefore be assumed that the variance of the population was homogeneous. Differences in measurements between patients with and without central incisors were compared using the independent t-test. Differences in the diameter of the incisive foramen in patients of various age groups were evaluated using analysis of variance. For all data, P values <0.05 were considered to indicate statistical significance.
RESULTS
Diameter of incisive foramen
Of the 203 patients included in the study, 36 were excluded. Of the 167 patients who remained, 99 were men and 68 were women, ranging in age from 20 to 84 years (mean, 54.66 years). The anteroposterior diameter of the incisive foramen was 4.79±1.26 mm, which was significantly larger than the mediolateral diameter (3.29±1.09 mm) (P<0.001). The incisive foramen was oval-shaped in the anteroposterior direction (Table 1). In addition, the diameter of the incisive foramen in the patients with central incisors was 4.61±1.26 mm in the anteroposterior direction and 3.22±0.95 mm in the mediolateral direction, which was smaller than that in the patients without at least one central incisor (5.21±1.15 mm in the anteroposterior direction; 3.52±1.45 mm in the mediolateral direction). However, there was no statistically significant difference in the mediolateral diameter between the 2 groups (P=0.126) (Table 1).
Table 1
Anteroposterior and mediolateral diameters (mm) of the incisive foramen according to the presence or absence of the central incisors

| Diameter of IF | Presence (n=128) | Absence (n=39) | Total (n=167) | P-value |
|---|---|---|---|---|
| Anteroposterior diameter | 4.61±1.28 | 5.21±1.15 | 4.79±1.26a) | 0.010b) |
| Mediolateral diameter | 3.22±0.95 | 3.52±1.45 | 3.29±1.09 | 0.126 |
Values are expressed as mean±standard deviation. All P values were obtained from the independent t-test for between-group comparisons.
IF, incisive foramen.
a)Statistically significant difference between the anteroposterior and mediolateral diameters of the incisive foramen (P<0.001); b)Statistically significant difference according to the presence or absence of the central incisors (P<0.05).
The diameter of the incisive foramen tended to increase with age in both measured directions, but the differences were not statistically significant (Table 2). Additionally, in both measured directions, the diameter was larger in men than in women, but this difference similarly lacked statistical significance (Table 2).
Table 2
Anteroposterior and mediolateral diameters (mm) of the incisive foramen according to age and sex

Horizontal and vertical bone thickness anterior and coronal to the incisive foramen
The width from the anterior point of the incisive foramen to the buccal border of the alveolar crest was 7.73±1.37 mm in the patients with central incisors, which was significantly larger than that in patients without at least one central incisor (6.89±1.31 mm) (P<0.001) (Table 3). Additionally, the height of the alveolar crest to the anterior border of the incisive foramen was 6.42±1.31 mm in the patients with central incisors, which was larger than that in the patients without at least one central incisor (5.96±1.26 mm); however, the difference between groups was not significant (Table 4).
Table 3
Width from the buccal border of the incisive foramen to the facial aspect of the buccal bone plate according to the presence or absence of the central incisors (n=167)

| Horizontal width of bone | Presence (n=128) | Absence (n=39) | Total | P value |
|---|---|---|---|---|
| Width from the IF buccal border to the facial aspect of buccal bone plate (mm) | 7.73±1.37 | 6.89±1.31 | 7.78±2.15 | 0.000a) |
Table 4
Height of the alveolar crest to the anterior border of the incisive foramen according to the presence or absence of the central incisors (n=167)

| Vertical height of bone | Presence (n=128) | Absence (n=39) | Total | P value |
|---|---|---|---|---|
| Height of the alveolar crest to the anterior border of the IF (mm) | 6.42±1.31 | 5.96±1.26 | 6.31±1.07 | 0.178 |
Description of nasopalatine canal shape
The shape of the nasopalatine canal showed a wide variety of patterns, among which the most prevalent shape was cylindrical. Most of the canals had a larger diameter near the incisive foramen than at the middle of the canal, and as a result, the diameter of the nasopalatine canal was wider and the bone was thinner near the incisive foramen.
DISCUSSION
When planning implantation, clinicians should carefully consider the anatomical limitations, especially in the anterior maxillary area, since they frequently encounter an insufficient labio-oral dimension of the residual ridge and facial concavity [16]. In addition, due to the apical and lingual progression of alveolar ridge resorption, the incisive foramen is often located near the alveolar ridge area [17]. The incisive canal contains the nasopalatine nerve, the terminal branch of the descending nasopalatine artery, fibrous connective tissue, fat, and small salivary glands [78]. Therefore, prior to implantation, it is necessary to take care to ensure that the nerve branches and blood vessels passing through the central incisor are kept intact. Kraut and Boyden [18] used computed tomography to analyze the location of the maxillary central incisor implant and incisive foramen. In his study, in 4% of the 84 cases, the incisive foramen was in a position that could affect the implantation in the vicinity of the central incisor. To prevent possible complications, we must recognize the morphology of the incisive foramen and surrounding bone, and the distance from the region of implantation to the relevant anatomical landmarks should be determined.
The region of the anterior maxilla is aesthetically, phonetically, and functionally important. In the present study, the anteroposterior diameter of the incisive foramen was measured as 4.79±1.26 mm, and the mediolateral diameter was measured as 3.29±1.09 mm. This is similar to the results of a study by Salemi et al. [19] in that the incisive foramen was found to be oval-shaped, with a larger anteroposterior than mediolateral diameter. In addition, the diameters in the patients without central incisors were 5.21±1.15 mm in the anteroposterior direction and 3.52±1.45 mm in the mediolateral direction, which were larger than the anteroposterior and mediolateral diameters of 4.61±1.28 mm and 3.22±0.95 mm, respectively, in the patients with central incisors. These findings resemble the results of a study conducted by Asumi et al. [13], which showed that the main reason for enlargement of the incisive foramen was tooth loss and atrophy of the alveolar ridge. Since the implant is not placed at the center of the anterior maxillary bone, care should be taken regarding perforation on both the buccal and lateral sides, considering the elliptical shape of the incisive foramen and the nasopalatine canal.
In addition, Mardinger et al. [20] reported that the incisive canal tended to enlarge with age and after central incisor extraction. Although no statistically significant differences were found in this study with regard to age, in both groups and at both measurement sites, incisive foramen diameter tended to increase with age. Thus, the enlargement of the incisive foramen in both groups depends on not only tooth loss, but also age-related changes in the surrounding bone. These 2 trends suggest that the patients without central incisors may have been younger than those with intact central incisors. In actuality, in the present study, the age of the patients with central incisors was lower than that of those without central incisors (53.9 years and 57.3 years, respectively), although this difference was not statistically significant.
The measured distance from the buccal border of the incisive foramen to the facial aspect of the buccal bone plate was 7.73±1.37 mm in the patients with central incisors, which was significantly larger than the 6.89±1.31 mm observed in the patients without central incisors. The vertical height from the anterior bone crest to the incisive foramen was 6.42±1.31 mm in the patients with central incisors and 5.96±1.26 mm in the patients without central incisors, although there was no significant difference between the groups. This is considered to have been due to the absorption and atrophy of the alveolar ridge arising from maxillary central incisor loss, similar to the results of previous studies [212223]. Eventually, when maxillary central incisor loss occurred, the distance from the incisive foramen became closer to the alveolar crest.
On the sagittal plane, the nasopalatine canal can have various shapes, such as cylindrical and funnel-like. However, regardless of shape, a similar tendency to have a wider diameter near the incisive foramen than at the middle of nasopalatine canal was observed [24]. In summary, the altered proximity of the incisive foramen is caused by changes in the pathway and diameter of the nasopalatine canal, which runs from the nasal cavity to the incisive foramen, as well as vertical and horizontal bone atrophy due to tooth loss. This can be an important precaution to keep in mind regarding anterior implants. The significant sensory disturbances due to invasion of the nasopalatine nerve and vessel are not yet well elucidated, but it should be recognized that bleeding and the decrease of the osseointegration area caused by perforation may result in additional problems, such as decreased implant support and infection. Even apart from implantation, surgical processes involving the palatal area of the anterior maxilla may benefit from prior identification of the horizontal and vertical locations of the incisive foramen. When anesthetic is injected directly under the incisive papilla, identifying the location of the incisive foramen using CBCT imaging before the injection can provide guidance for the operating surgeon to avoid damaging nerve branches and blood vessels by excessive penetration of the anesthesia needle into the incisive canal.
Ultimately, atrophy of the maxillary alveolar ridge and enlargement of the incisive foramen occur after maxillary incisor extraction. Therefore, when an implant is placed, it may cause invasion of the buccal dehiscence or incisive foramen, and it is difficult to set the implant in an aesthetically and functionally ideal position; thus, guided bone regeneration and distraction osteogenesis should be considered after loss of the central incisors. It is also necessary to identify the bone morphology and the location of the incisive foramen through CBCT and to determine accurate placement before implantation. In fact, both the location of the incisive foramen and the nasopalatine canal configuration should be carefully evaluated by CBCT during the diagnostic process.
This study has several limitations. First, it was a cross-sectional study, so it did not reveal the effect of changes in bone morphology or age within the same individual at different times. Thus, an additional longitudinal study is necessary to clarify these findings. Second, the measurements in this study were performed by only 1 person, leading to the possibility of a certain level of subjectivity. Lastly, the number of samples was small, because many samples, especially in the patients without central incisors, were difficult to measure accurately due to poor computed tomography images or artifacts. Therefore, it is possible that the statistical power of this study was reduced by the small number of patients without central incisors. Therefore, further studies with larger populations are needed.
 XML Download
XML Download