

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Periodontal plastic surgery is an important component of periodontal treatment [1]. Within this category of surgery, root coverage procedures are not only performed for aesthetic purposes, but also constitute an alternative technique to treat cervical injuries, eliminate plaque-retentive factors, and improve dentin sensitivity [23].
Among the various surgical techniques suitable for the treatment of gingival recession, subepithelial connective tissue grafts (SCTGs) are widely used for treating both single and multiple recessions due to the relatively high predictability of root coverage [24567].
The harvest of SCTGs, which involves separation of the epithelial tissue from the connective tissue, can be performed in different ways. One option is to raise a full- or partial-thickness flap, and another is joint excision of the epithelium and connective tissue, with subsequent separation of these closely-related tissues [2456].
The areas of choice for SCTG harvest are the palate, the tuft of the maxilla, and edentulous areas with sufficient tissue thickness. The most commonly used area is the palate, in locations limited to positions distal from the canines to the first molar, due to its vascular anatomy and distribution of tissue thickness [89].
The overall mean thickness of the palatal masticatory mucosa was found to be 3.83±0.58 mm (range, 2.29–6.25 mm) [10]. On average, the tissues of interest for grafting techniques have 0.41-mm-thick epithelium [11] and 2- to 4-mm-thick lamina propria [12]. Fewer than 50% of patients with mucogingival problems have an adequate fibrinous palatine thickness for the removal of connective tissue by conventional techniques. In other cases, it is necessary to remove epithelial tissue together with connective tissue, and subsequent de-epithelialization is performed with a scalpel blade, a technique described by Bosco and Bosco [29]. In this technique, a previously delimited portion of full-thickness tissue is removed and sectioned outside the mouth with the use of a scalpel blade, thereby dividing the epithelial tissue from the connective tissue. Then, the portion containing the epithelial tissue and a thin layer of connective tissue is repositioned in the donor area [2].
Epithelial tissue can also be removed through abrasion, which is indicated for the removal of melanic pigmentation in gingival tissue. In this technique, the goal is for the maximum amount of epithelium to be removed under direct visualization. This procedure is done using a high-speed diamond bur under abundant irrigation, until a bleeding surface is visualized [131415].
Some studies have presented histological evaluations of SCTGs. In 2003, Harris [16] analyzed 32 SCTGs, all removed by the technique of parallel incision, and a histological analysis explored the presence or absence of epithelial remnants, the mean depth of the tissues present in the graft, and the proportion of each tissue in relation to the total area of the graft. In 80% of the grafts analyzed, the presence of an epithelial remnant was reported, and an analysis of a wide range of parameters relating to the composition of the epithelial remnants led to the conclusion that the connective tissue grafts collected and evaluated were uniform.
The importance of the epithelial remnant and its clinical impact has been studied by some authors [45617], who suggested that the presence of epithelial tissue in SCTGs may result in the formation of epithelial cysts. In a 1999 study, Harris [18] also reported the possibility that a groove could form between the SCTG and the tooth surface, hindering the process of regeneration by the development of the epithelial remnant, which becomes continuous to the outer layer of the epithelium.
There are no reports in the literature on the histological composition of SCTGs harvested using different techniques, justifying the need for this novel study.
The objective of this split-mouth study was to conduct a histological evaluation and comparison of 2 different ways of removing the epithelial tissue from SCTGs in terms of the presence of epithelial remnants and the composition of the tissues present in the graft through an evaluation of the area, thickness, and proportion in relation to the total area of the graft of each tissue type.
MATERIALS AND METHODS
This study was approved by the Ethics Committee in Research of the Pontifical Catholic University of Paraná (PUCPR) (No. 1.601.764).
Ten patients were selected at the dental clinic of PUCPR who presented at least 2 teeth in different hemiarches with gingival recession of ≥2 mm and no loss of interproximal attachment, classified as RT1 according to Cairo et al. [1920] Patients with systemic disease and those who had detrimental oral habits were excluded from the study [21]. All the patients signed a form indicating that they provided free and informed consent; this form contained comprehensive information about this study.
The selected patients received instructions for oral hygiene and basic periodontal treatment prior to the surgical procedures, including scaling and root planing [22]. Acetate mouthguards with a thickness of 1.33 mm (Whiteness®, FGM, Joinville, Brazil) were also produced and used in the postoperative period to improve patients' comfort.
Surgical procedures
SCTGs were removed from 2 regions of the palate in each patient, in the area between the distal face of the canine and the maxillary first molar (a split-mouth design). A single surgeon performed all surgical procedures. At one of the surgical sites, after removal of the SCTG, de-epithelialization was performed by using a scalpel blade, as described by Bosco and Bosco [2]. At the other surgical site, de-epithelialization was performed using the abrasion technique, rapidly followed by removal of the SCTG [14]. Both procedures were performed in the same session in order to avoid carrying out 2 separate operations; this aspect of the protocol also had the methodological advantage of enabling the comparison of 2 samples collected from each patient at the same time.
The samples were classified according to the technique used to remove the epithelial tissue from the SCTG: 1) B: blade; 2) A: abrasion.
The recipient site was prepared by prior root scaling and scraping of the involved tooth using a #7–8 periodontal curette (Hu-Friedy, Chicago, IL, USA). Local anesthesia was performed at the surgical sites using an anesthetic with a vasoconstrictor agent at a concentration of 1:100,000 (Mepiadre 100, DFL, Rio de Janeiro, Brazil) [2]. With the aid of a No. 15 scalpel blade, an intrasulcular incision was made, keeping the papillae intact and creating an envelope in the tissue surrounding the root surface that was the recipient area of the SCTG [6]. Incisions were made using a No. 15 blade at in the donor site, delimiting the area of the graft to be harvest [2] and also to facilitate a clear view in procedures using the abrasion technique [14]. The dimensions of the donor area were measured using a millimeter periodontal probe (Hu-Friedy) as shown in Figure 1A.
Figure 1
(A) Use of a millimeter periodontal probe to determine the dimensions of the tissue in the donor area. (B) Flap containing epithelial tissue, connective tissue, and submucosal tissue being removed from the donor area. Care was taken to maintain a uniform thickness of the graft and to keep the periosteum as intact as possible. (C) Use of a No. 11 blade to separate the epithelial tissue from the connective tissue.

After the incisions were made, in the procedures where the de-epithelialization was performed with a blade, the full- or partial-thickness flap was raised and removed from the palate, and care was taken to maintain a uniform thickness of the SCTG (Figure 1B). The graft was then sectioned using a No. 11 scalpel blade (Swann-Morton, Sheffield, UK) outside the oral environment and on the sterile field to separate the epithelial tissue from the SCTG [2], as shown in Figure 1C. Observation was used to determine whether the extent of de-epithelization was sufficient.
In the de-epithelialization procedures performed using the abrasion technique [14] a high-speed diamond bur (3053 FG, KG Sorensen, Cotia, Brazil) and abundant irrigation were used, with careful handling to ensure that the epithelium was removed evenly. The graft thickness was standardized according to clinical parameters (namely, visualization of a uniform and bleeding surface; Figure 2) indicating total removal of the epithelium. In regions that appeared to contain only connective tissue, the graft was incised with the aid of a No. 11 blade and removed from the donor area. This standardization was efficient, as shown by the absence of any statistically significant differences in the thickness of the grafts.
Figure 2
(A) Diamond bur used in the abrasion procedure. The flat structure aids in the removal of the epithelial tissue. (B) Removal of the epithelial tissue using a high-speed diamond-tip drill and abundant irrigation.

For hemostasis of the donor areas, bismuth subgallate [23] was used intraoperatively. In addition, an acetate mouthguard was produced for the patient to use in the postoperative period, in order to ensure utmost comfort.
The size of the SCTGs removed was sufficient to carry out root coverage (Figure 3A) and to obtain a sample of the graft, measuring 3 mm in width and 10 mm in length (Figure 3B), for histological processing. In order to standardize the edge of the SCTG at which histological sections were made, a small incision was performed on the opposite side of that used for histology. The side of the graft chosen for the histological sections was the length of a long axis pointing to the patient's teeth in order to palatal tissue with a composition closer to that of gingival tissue, with a relatively high quantity of collagen fibers and a relatively low content of glandular and fat tissue (Figure 4).
Figure 3
(A) SCTG removed. (B) SCTG, measuring 10 mm in length and 3 mm in width, with the 14 standardized measurements to be used in the histological analysis.
SCTG: subepithelial connective tissue graft.

Figure 4
Schematic drawing showing the portion of the graft with the standardized measurements for use in the histological analysis. The section was obtained along the long axis of the graft with the region of choice facing the teeth of the patient. To identify the edge to be used for histology, a small incision (*) was performed on the opposite edge.

SCTGs with standardized dimensions for histological analysis were placed in a 10% formalin solution and sent for histological processing [16]. The portion of the graft used for root coverage was positioned in the envelope created previously in the recipient area. Digital compression was performed with gauze to stem the bleeding and to stabilize the SCTG [2].
The SCTG was stabilized by suturing (Mononylon Ethicon, Johnson & Johnson, São Paulo, Brazil), which was maintained for 7 days.
As systemic postoperative medication, 750 mg of paracetamol was administered every 6 hours for 3 days. For local use, 0.12% chlorhexidine digluconate mouthwash was prescribed (Periogard®, Colgate-Palmolive, São Paulo, Brazil) for use every 12 hours for 4 weeks [2].
Histological analysis
All the steps involved in processing the samples for histological analysis were performed at the Laboratory of Experimental Pathology of PUCPR.
The SCTG samples removed from the palate were fixed in 10% formalin solution for 24 hours, processed, and embedded in paraffin. Histological sections with a thickness of 4 µm were made in the direction of the long axis of the specimen, facing the teeth of the patient. The sections were stained with hematoxylin and eosin.
The slides obtained were digitalized using the ZEN 2.3 Lite Program (ZEISS Microscope Software ZEN Lite, ZEISS, Oberkochen, Germany) in 3% of a ×20 lens. The images were analyzed using the Image Pro Plus 4.5 program (Media Cybernetics, Inc., Silver Spring, MD, USA) (Figure 5). The following parameters were measured:
Figure 5
Histological image of a sample from group A analyzed in the Image Pro Plus 4.5 program, where tools were used to make measurements of the studied variables (3% of a ×20 lens).

1) The presence of an epithelial remnant, through direct visualization of present epithelial tissue.
2) Thickness of the epithelium, lamina propria, and submucosal tissue when present, through measurements at 5 points using the “grid mask” and “measurements” tools. The mean value of the 5 measurements was obtained for each of the tissue types.
3) The area of epithelium, lamina propria, and submucosal tissue present, through semi-automated segmentation in which the proportion of each tissue type was calculated in relation to the total area of the sample.
Statistical analysis
SPSS version 23.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses. To evaluate the reproducibility of the variables, the measurements were carried out at 2 distinct times. The Dahlberg error for the variables of this study was consistently lower than 0.1%, indicating reliable reproducibility of the measurements. The Student's t-test for paired samples indicated no statistically significant difference between the mean values of the variables between the time points, confirming the absence of systematic error in the measurements.
To compare the samples in terms of the presence of epithelial remnants between groups A and B, the Z test for differences between 2 proportions was applied. In order to determine whether the mean values of the variables differed according to the technique employed, the Kolmogorov-Smirnov test of normality and the Levene test for homogeneity of variance were applied. For variables presenting a normal distribution, the parametric Student's t-test for independent samples was applied. For variables that did not present a normal distribution, the non-parametric Mann-Whitney U test for independent samples was used. In the variables where the Student's t-test was applied for independent samples and the Levene test showed heterogeneous variance, the Student's t-test for independent samples was used with the Aspen-Welch correction for degrees of freedom. For all the tests, the significance level was set at 5%.
RESULTS
Presence of epithelial remnants
In group A (Figure 6) (n=10), the presence of an epithelial remnant was observed in 2 samples (20%), while in group B (n=10), 4 samples (40%) showed an epithelial remnant (Figure 7). When the 2 groups were compared, no statistically significant difference was observed (Table 1).
Figure 6
(A) Histological section of a sample from group B where no epithelial remnant was present (hematoxylin and eosin staining; 3% of a ×20 lens). (B) Histological section of a sample from group B where an epithelial remnant was present (*) (hematoxylin and eosin staining; 3% of a ×20 lens).



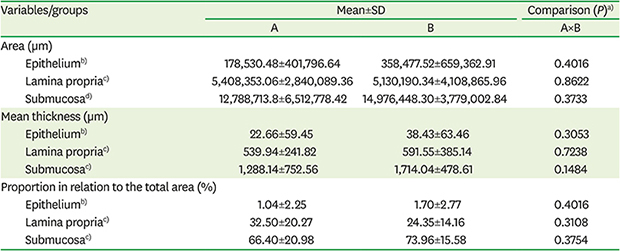
Area
No statistically significant differences between the groups were found in the mean area of all 3 tissue types (epithelium, lamina propria and, submucosa) (Table 2).
Table 2
Composition of grafts
Mean thickness
The mean thickness based on the 5 measurements performed for each of the tissues was calculated. No statistically significant differences between the groups were found for any of the 3 tissue types (Table 2).
Proportion in relation to the total area
The proportion of epithelium, lamina propria, and submucosal tissue relative to the total area of the graft was calculated. No statistically significant differences were observed between groups A and B for all 3 tissue types evaluated (Table 2).
Regarding graft composition, the largest area, average depth, and proportion in relation to the total area was found for the submucosa, followed by the lamina propria and epithelium.
DISCUSSION
This study demonstrated no statistically significant histological differences between the 2 techniques (abrasion and blade) of removing epithelial tissue, and when the tissue types constituting the SCTGs were evaluated, the area and thickness of each tissue type were not significantly different between groups A and B.
The presence of an epithelial remnant was histologically observed in some samples from both groups evaluated, but without a statistically significant difference between the groups. The mean thickness of the epithelial tissue of the palate is 0.41 mm [11]. For both techniques, the depth of epithelial removal is under visual control [214], and in groups A and B, the mean thickness of the epithelial remnants was 0.02±0.04 mm and 0.04±0.06 mm, respectively (note that the values in Table 2 are in micrometers). Although histological evaluations were performed in this study, the findings are of important clinical relevance as they reflect different techniques that were performed in surgical procedures in the selected patients. Some authors have suggested that the presence of an epithelial remnant can have a meaningful clinical impact because it possibly results in the formation of cysts [152425] or halts the process of periodontal regeneration through development of the remnant in epithelial invaginations [17]. Wei described the formation of a persistent bulky tissue with a thick white discharge after an SCTG procedure [26], and Vastardis presented 3 cases of abscess formation [27]. However, several authors have evaluated the presence of epithelial remnants (and even the presence of all the epithelial tissue) in SCTGs, and reported that there were no clinical differences [45617]. It is suggested that future studies should also evaluate the clinical parameters of the 2 techniques, including whether cyst formation occurs in cases with an epithelial remnant, in order to compare such data with the histological findings.
The main purpose of SCTGs is to increase the predictability of root coverage, bringing long-term stability and preventing relapse through transformation of the gingival biotype [2829]. In this study, when the composition of the grafts was evaluated in terms of the thickness, area, and proportion in relation to the total area of each tissue type, the values varied considerably.
Few studies have assessed the composition of SCTGs. In a 2003 study by Harris [16], only a single technique for SCTG removal was used, which makes it very useful for a comparative study using 2 different techniques.
Zucchelli [9] reported that the technique of graft removal with diamond drill de-epithelialization was considered more difficult both surgically and biologically due to bleeding and difficult visualization. Furthermore, superficial tissue necrosis may occur when rotating instruments are used, impairing the vascular exchange between the connective tissue and the flap. This finding was not observed in any of the samples of this study. In addition, in the present study, another type of drill was used (a flat diamond bur with a thickness of 2 mm), which allowed greater uniformity in epithelial removal. Using this drill in combination with abundant irrigation resulted in easy visualization of the operative field.
Although a greater amount of connective tissue would be expected without the presence of epithelial remnants [17] and submucosa [30], Harris [16] found a broad range of results, with no statistical significance, in a histological evaluation of the thickness, area, and proportion in relation to the total area of SCTGs of each tissue type in procedures performed using parallel incision; those results therefore agree with the findings of this study. In addition, in all the grafts performed by Harris (n=32), root coverage was obtained without reports of unfavorable clinical findings [16].
As there was no statistically significant difference between the techniques, the abrasion technique may be preferable because it is technically easier, requires less training, and is more flexible as a procedure. Epithelial removal with a blade, as described by Bosco and Bosco [2], is technically more difficult in our experience because it involves an incision outside the buccal region n unstable soft tissue, making it challenging for the incision to be performed precisely, in contrast with Zucchelli's report [16].
In conclusion, in a histological evaluation of SCTGs in which the epithelial tissue was separated by the abrasion and blade techniques, for all the variables studied, no significant differences were observed in the composition of the SCTGs.
 XML Download
XML Download