

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
National health insurance in Korea began to cover emergency and critical care ultrasound examinations in July 2019.1 This could lead to more acute care by physicians who use more point-of-care ultrasound (POCUS) and reduce the financial burden on the patients. The Society of Emergency and Critical Care Imaging (SECCI) has summarized and provided recommendations on the desirable use of POCUS in emergency and critical care setting under the Korean Health Insurance System.
POCUS is an ultrasound examination that is performed at the bedside, and it is interpreted directly by the clinician.2 Therefore, POCUS is a powerful adjunct to clinical assessment. The certainty of the presumptive diagnosis that is derived from the medical history, and physical examination can be confirmed by the information provided using POCUS. Additionally, POCUS can be an effective tool for monitoring patients and for procedure guidance. Although the main purpose of POCUS is slightly different between intensivists and emergency physicians, the capability to recognize and resuscitate critically ill patients is a defining trait in both specialties.3 For critically ill patients, such as those with thoracoabdominal trauma, cardiac arrest, respiratory difficulty, chest pain, or shock, bedside multi-organ POCUS is now extensively used as an adjunct that provides many pieces of information to guide clinical decision-making during the initial and undifferentiated phases.4
In this article, we will review all types of clinically integrated, single/multi-focused, and single organ/multi-organ POCUS for emergency physicians and intensivists. All acute care physicians should use the following procedure: 1) stabilize the unstable patients; 2) make a differential diagnosis; and 3) monitor the patient to tailor the ongoing management. In each step, POCUS is a useful modality.
SCOPE OF PRACTICE FOR POCUS
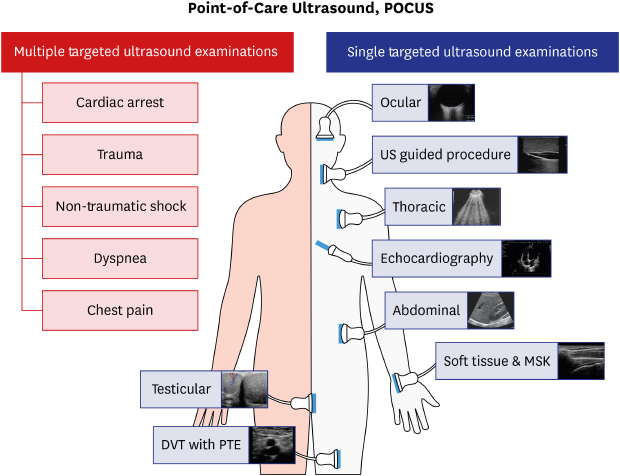
Emergency and intensive care physicians will perform basic ultrasonography using POCUS as designated by health insurance. Physicians also need to maintain a level of skills and attain the same scan proficiency.5 POCUS can be divided into single-targeted ultrasound examinations (STU, one or two scanning sites) and multiple-targeted ultrasound examinations (MTU) depending on the purpose. The key components of POCUS are considered and are described below (Fig. 1).

SINGLE-TARGETED ULTRASOUND EXAMINATIONS (STU)
Point-of-care cardiac ultrasound
The point-of-care echocardiography (POCE) uses a limited number of standard echocardiography views to rapidly assess cardiac anatomy and function in the critically ill patient.6 Generally, the five standard views include the parasternal long-axis, parasternal short-axis, apical four-chamber, subcostal and suprasternal notch views that are scanned.7 The examination can be performed in a few minutes, and it is generally combined with other aspects of POCUS, such as thoracic ultrasound, Focused Assessment with Sonography for Trauma (FAST) and evaluation for abdominal aortic aneurysm (AAA) and deep vein thrombosis (DVT).8910
Thoracic ultrasound
Thoracic ultrasound is performed on patients with dyspnea and pleuritic chest pain. Bedside thoracic ultrasound should be considered to be an image modality that can be used initially for patients who are in respiratory failure in the emergency or intensive care unit (ICU) because it is fast, safe, and informative compared with anteroposterior chest X-ray, and it demonstrates a similar performance compared with computed tomography.1314 Since Lichtenstein announced the Bedside Lung Ultrasound in Emergency protocol in 2008, numerous papers have shown the usefulness of lung ultrasound in many clinical scenarios.15 Thus, lung ultrasound is strongly recommended for detecting pneumothorax, alveolar-interstitial syndrome, pulmonary consolidation and pleural effusion.1617
Evaluation for DVT with pulmonary embolism
To differentiate the cause of pulmonary embolism, evaluation for DVT is needed. Hypotensive patients with pulmonary embolism have typical ultrasound findings, such as enlarged right ventricle, D-shaped left ventricle, and the presence of DVT. The POCUS DVT examination can be performed rapidly using the two-dimensional compression method without a Doppler study.1819
Abdominal ultrasound
The main applications in abdominal ultrasound include bowel, trauma, biliary, urinary tract, and AAA.20 A patient who has right upper quadrant (RUQ) pain in an emergency should be evaluated with abdominal POCUS to detect if the pain is of biliary origin. POCUS for acute cholecystitis is as accurate as ultrasound that is performed by a radiologist and cholescintigraphy.21 Use of POCUS for RUQ pain allows emergency physicians to determine if the origin of the pain is biliary colic. Sonographic tenderness in the gallbladder (GB) area, size, and presence of gallstone, GB wall thickening and pericholecystic fluid collection can be evaluated using abdominal POCUS, including common bile duct pathology. Renal POCUS helps to manage acute kidney injury and nephrolithiasis. In obstructive uropathy patients, hydronephrosis can be diagnosed with ultrasound.22 Emergency physicians can determine rapid and efficient disposition of patients with renal colic without radiation exposure using renal POCUS. Additionally, POCUS of the aorta includes measuring the shape and diameter of the abdominal aorta as well as inspection for a dissection flap. Emergency physicians can identify a ruptured AAA with a high sensitivity and specificity.23 In the emergency department, the primary concern for the women who are of their reproductive age and who have pelvic pain is ovarian torsion or ovarian cyst rupture. POCUS becomes the primary modality for its evaluation because it is difficult to diagnose based on symptoms and physical examination.24
Ultrasound-guided procedure
It is already well-known that ultrasound-guided procedures are accurate and safe methods.2526 It is especially very useful for critically ill patients in the emergency department and the ICU because physicians have to perform various procedures at the bedside.272829 The ultrasound-guided procedure can be used in central and peripheral venous catheterization, arterial catheterization, thoracentesis, paracentesis, pericardiocentesis, arthrocentesis, nerve block, confirming of endotracheal intubation, site marking for surgical airway, abscess drainage and foreign body removal.30
Testicular ultrasound
Acute scrotal pain accounts for approximately 0.5% of all patient complaints in the emergency department.31 In the emergency department, POCUS is used to diagnose testicular problems such as hydrocele, varicocele, testicular torsion, epididymitis, orchitis, and hernias, and also to evaluate scrotal trauma. Misdiagnosis of testicular torsion can lead to organ damage and compromise fertility, and testicular ultrasound is a useful rapid diagnostic tool.32
Soft tissue and musculoskeletal ultrasound
Soft tissue and musculoskeletal ultrasound is used to evaluate soft tissue infection, fracture, dislocation, muscle injury, foreign body, tendon injury, and joint effusions.3334353637 Ultrasound could diagnose some fractures including injuries that are difficult to diagnose using conventional radiography, such as scaphoid, sternum, occult rib, and some avulsion fractures. Additionally, ultrasound could identify radiolucent foreign materials such as glass or wood.33 Screening with ultrasound by an emergency physician could reduce costs, time requirements, and radiation exposure.
Ocular point-care-of ultrasound
Optic nerve sheath diameter is a well-known parameter of increased intracranial pressure.3839 Additionally, ocular POCUS would be useful for evaluation for traumatic eye injuries and visual disturbances. Emergency physicians can evaluate the anatomy of the eye via a dynamic POCUS study of the eyes, such as location of the lens, presence of a foreign body, and presence of vitreous detachment.4041
MULTIPLE TARGETED ULTRASOUND EXAMINATIONS (MTU)
Ultrasound in cardiac arrest
The transthoracic cardiac ultrasound in cardiac arrest patients can be performed within 10 seconds of stopping chest compressions for a pulse check, and this should not be associated with delays in chest compressions.42 If the heart cannot be visualized within seconds after the chest compressions are stopped, POCUS should be aborted. POCUS can be subsequently attempted using a different approach after five cycles of chest compressions. The subcostal approach is recommended first, and if the heart is not observed, the parasternal and apical approach can be the next option. 43 POCUS examinations of the thorax, abdomen, and inferior vena cava can be performed during chest compressions. In cardiac arrest patients, identifying the potential to reverse this condition cause might improve resuscitation outcomes. POCUS can provide guidance for better resuscitation using the information described below.44 We can differentiate true cardiac arrest rhythm45 such as pulseless electrical activity and false cardiac arrest rhythm using the sonographic cardiac activity in patients with no pulse. The prognosis for return of spontaneous circulation is improved when there is organized sonographic cardiac activity.46 If cardiac contractility is absent following a reasonable period of cardiopulmonary resuscitation, this indicates a limited probability for return of spontaneous circulation.45474849
POCUS for the evaluation of non-traumatic shock
POCUS provides real-time physiologic information in a patient with shock. Emergency and critical care physicians obtain guidance to differentiate between the type of shock, impact of management, and non-invasive monitoring by interpretation through POCUS. Shock has an estimated mortality rate of 36%–60%, depending on the type of shock.50 Rapid evaluations for etiology, monitoring, and rapid correction are important to decrease the mortality rate and improve patient safety. The categories of shock are quantitative shock (decreased flow: hypovolemic, cardiogenic, obstructive; decreased oxygen carrying capacity: anemia, hypoxemia) and distributive shock (sepsis, anaphylaxis). POCUS allows for rapid identification of the type of shock and it has been proposed as a first-line evaluation modality.51 In the assessment of patients with undifferentiated hypotension, hemodynamic assessment with POCUS for preload, cardiac function, and afterload has become an accepted diagnostic and monitoring tool.46525354 POCUS can be a risk reduction tool through its emergent diagnostic imaging capacity, shortening time to definitive therapy, and its use in therapeutics or in physiological monitoring.30
Ultrasound in chest and abdominal trauma
POCUS is useful as an initial diagnostic tool to identify free fluids in dependent locations within the peritoneal cavity in abdominal trauma patients.55 Immediate laparotomy is usually performed in unstable patients with intraperitoneal hemorrhage that is quickly identified by POCUS without CT scan.56 However, POCUS should not be used to replace more sensitive tests in patients with impaired abdominal or chest trauma symptoms. Multidetector computed tomography (MDCT) is highly sensitive for solid organ injury and intraperitoneal or intrathoracic bleeding and is the study of choice if the patients are hemodynamically stable. POCUS at the initial examination and resuscitation of trauma patients is known as FAST, which is a standard screening test that is performed on trauma patients.57 Evaluation of pericardial effusion, an intraperitoneal test, right and left flank and pelvic examinations are performed to locate free fluid in the abdominal cavity. In many cases, extended FAST (E-FAST) is performed to find a pneumothorax. FAST is most helpful when the results are positive, and when the time to definite treatment is decreased. FAST is generally performed during the “C” portion, which evaluates circulation and hemorrhage in a primary survey of Advanced Trauma Life Support. A low-frequency (2.5 to 5 MHz) curvilinear or phased array probe is appropriate. The standard sequence of FAST is pericardial, right flank (hepatorenal view or Morison's pouch), left flank (perisplenic view), pelvic (retrovesical views), and thoracic (pneumothorax and hemothorax evaluations).58 The use of MDCT in hemodynamically unstable patients should be determined by assessing the patient's degree of instability and the distance to the MDCT scanner.59 FAST is sensitive and specific in the determination of both traumatic pericardial effusion and intraperitoneal fluid that is indicative of injury, and thus, it effectively guides emergent surgical decision-making.60 However, limited sensitivity precludes the use of POCUS as a definitive test to rule out intraabdominal injury.61 Each FAST examination reflects the clinical situation at a single moment. The overall sensitivity of FAST for abdominal injury can be improved using serial ultrasound examinations. A second ultrasound examination improves sensitivity, negative predictive value, and accuracy for intra-abdominal injury.62 The pelvic region is the most dependent space in the supine patient, and therefore, it is an important site to look for free fluid. A determination of pneumothorax focuses on visualization of pleural sliding without relying on detecting free fluids.
Ultrasound in pediatrics
Pediatric patients are vulnerable to ionizing radiation, and therefore, ultrasound is the main diagnostic modality rather than computed tomography or radiography.6364 Ultrasonographic findings of viral pneumonia or bronchiolitis are B-line and/or subpleural consolidation, and those of bacterial pneumonia include B-lines and/or lung consolidation and sonographic air bronchogram.6566 In the emergency department, POCUS is used on pediatric patients with traumatic symptoms such as fractures, foreign bodies, or hip pain. The cause of hip effusion varies, but transient synovitis and septic arthritis are common in pediatric patients in the emergency department. Although ultrasound is not a confirmative diagnostic tool, it is important to confirm the presence of hip effusion with ultrasound. POCUS is also useful and valuable diagnostic imaging tool in children with nonspecific manifestations of intussusception.67
Ultrasound in the emergency department
Ultrasound in the emergency department has been used as an integral part of critical care and resuscitation in recent years, and the range of ultrasound use in the emergency department has greatly expanded. Emergency medicine (EM) physicians can use POCUS for critical care in the emergency department as follows: differentiating shock states; finding causes of respiratory failure; guiding fluid resuscitation; and accessing neurologic dysfunction.68 There are a variety of shock protocols using ultrasound but the use of the Rush protocol69 or the echo-guided life support protocol70 may be more efficient in our emergency department because it is feasible to evaluate the heart, the lung, and vessels in the abdomen together as a multi-directional assessment.6970
However, in addition to using ultrasound for critical care, ultrasound has a high use rate for diagnosis and procedures in various situations in which emergency department patients find themselves. EM physicians can use an extensive POCUS to examine abdominal, obstetric, testicular, musculoskeletal, and ocular lesions and to allow procedural guidance.
EM physicians should perform an exact evaluation using ultrasound, which can be used to make a definitive decision on the final disposition or discharge with a diagnosis that is determined by ultrasound. Therefore, assistance and advice should be sought from more experienced specialists if there are uncertain findings.3
Ultrasound in ICU
Ultrasound in the ICU is performed in an extensive field of diagnosis and management of critically ill patients who have a variety of disease features. As an extension of ultrasound in the emergency department, ultrasound in the ICU should focus on being comprehensive and complete rather than being rapid and essential.71 Comprehensive ultrasound studies to assess the full functional and structural status often revise the treatment strategy, and help to understand the disease status, and guide treatment. For example, routine comprehensive echocardiography in the general ICU revealed a clinically significant cardiac problem in one-third of patients with severe and critical cardiac disease that was previously unknown in 7.5% of patients.72 Because it is impossible for ICU physicians to perform comprehensive and professional ultrasound in diverse fields such as abdomen, thorax, and heart, ultrasound in the ICU has to be multidisciplinary and cooperative between clinical departments. ICU intensivists play a role in communication between the departments.
However, patients in the ICU are at high risk to experience disease exacerbation and develop complications. Therefore, clinicians in the ICU should be ready to perform POCUS to identify shock and assess fluid responsiveness.73 Additionally, procedures performed in the ICU such as insertion of an intravascular catheter, chest tube, effusion drainage from the thorax or abdomen, and tracheostomy can be performed under ultrasound guidance. Ultrasound guided procedures should always be considered first where available. ICU patients often experience clinical deterioration repeatedly from diverse causes, which requires comparison between current and previous ultrasound findings.
INSURANCE ISSUE
In Korea, the insurance coverage for ultrasound examination is gradually expanding in accordance with measures to enhance the national health insurance coverage, which began in 2017 and will continue until 2021, because the importance of ultrasound for on-site diagnosis has been emphasized. Full coverage of the insurance for POCUS in the emergency and critical care areas was implemented in July 2019.1 The National Health Insurance Act of Korea defined POCUS as a basic sonography tool that is required for differential diagnosis and treatment decisions in the emergency and critical care units. It is classified as STU (one or two scanning sites) and MTU (Table 1). The cost of POCUS can be covered by health insurance based on the conditions described below. First, it should be performed in the emergency department or ICU at the hospital. However, if the examination is performed in an emergency situation, the place where the examination can be conducted is not limited. Second, the physician should perform the ultrasound directly and record the findings (Table 2) in the patient's medical record (Tables 3 and 4). MTU examinations can be covered by insurance if the purpose (indication), personnel, and range of examination (Table 1) are all met. If these conditions are not met, it is regarded as a STU examination. The cost for payment of an ultrasound examination is different based on the Korean Triage and Acuity Scale in the emergency department. If the Korean Triage and Acuity Scale of the patients ranges from 1 to 3, 20% of the total cost will be charged to the patient. Additionally, 30% to 60% of the total cost will be charged to the patient depending on the types of medical institution (e.g., tertiary hospital, general hospital, or primary clinic).
Table 1
Classification of basic ultrasound examination: single targeted versus multiple targeted

Table 2
Essential component for medical records in single and multiple targeted ultrasound examination according to the scanning area

Table 3
Examples of medical records for the single targeted ultrasound examination (point-of-care echocardiography)

Table 4
Examples of medical records for the multiple targeted ultrasound examination (differential diagnosis for shock)

There are several points to be noted regarding the type of medical institution. First, the insurance code system for diagnostic, guided, and special ultrasound examination has not been changed. Second, basic ultrasound examination classified as a STU or MTU examination can be performed whether or not the ultrasound is for diagnostic purpose based on the physician's decision. However, the Health Insurance Review and Assessment Service plans to monitor the prescription status on whether a basic or a diagnostic ultrasound examination is prescribed simultaneously and if it is repeated too many times. Third, the MTU examination is allowed only in cases of trauma, cardiac arrest, shock, chest pain, and dyspnea. In other cases, a STU examination over two or more sites should be prescribed, even though multiple sites will be scanned. Fourth, physicians should scan all parts of the chest, heart, abdomen, and pelvis when they prescribe an MTU examination. However, there are no obligations for recording all findings in the medical record. Recording one or more findings on each organ will be enough. Fifth, the cost of MTU can be covered on national health insurance when performed only by an authorized physician, such as: resident physician or specialist in EM, specialist in critical care medicine, or specialist in trauma surgery.
CONCLUSION
POCUS has become an important modality in the emergency and critical care setting. It will become an essential diagnostic component to treat patients appropriately and promptly or to make a differential diagnosis. More studies are needed to support various indications and critical situations in other fields.
 XML Download
XML Download