

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Aplastic anemia (AA) is a disease characterized by an overall decrease in blood counts in peripheral blood (PB) due to insufficient hematopoiesis in the bone marrow (BM).1 The pathogenesis of AA was found to be quantitative reduction of early immature hematopoietic stem cells (HSCs). The immunologic mechanism of this process was suggested by the restoration of hematopoiesis with immunosuppressive therapy (IST) including antithymocyte globulin (ATG) and cyclosporine A (CsA) in two thirds of the cases,12 and also evidenced by the suppression of the hematopoiesis with cytokines including interferon-γ and tumor necrosis factor-α. These cytokines act on the Fas/Fas ligand and produce NO to induce apoptosis.3 Clonal expansion of cytotoxic T cells with reverse correlation with the disease activity was observed in some cases.4
Allogeneic hematopoietic stem cell transplantation (HSCT) or IST have been used as specific treatment for severe aplastic anemia (SAA) to restore hematopoiesis for the last 40 years. The choice between these two modalities was guided by the age of the patient and the availability of the human leukocyte antigen (HLA)-matched related or unrelated donor (UD).5 For pediatric patients with SAA, matched related transplantation should be pursed preferentially, as recent studies result in long-term survival in more than 90% of cases. For children lacking a matched related donor (MRD), IST has been offered to result in a comparable survival, but a significant proportion of patients remains transfusion-dependent or develops a relapse after response to IST.6 Traditionally, unrelated or alternative donor transplantation has been reserved for patients who are refractory or have relapsed after IST. However, recent improvement in survival following unrelated or alternative donor transplantation which is almost equivalent to that of MRD suggest the feasibility of upfront unrelated stem cell transplantation (SCT).67
A gradual improvement in the outcome of HSCTs in pediatric AA over the past 30 years has been attributed by the refinement of conditioning regimen, improvement of supportive care, and DNA typing of histocompatibility antigens, and so on.8 Recently, studies on graft-versus-host disease (GvHD)-free/failure-free survival (GFFS) which reflects better quality of life than overall survival (OS) and failure-free survival (FFS), have been conducted in allogeneic SCT on patients with childhood hematologic malignancy.9 Although the outcomes of pediatric HSCT in Korean AA have been reported in several studies,1011 the trend of HSCT strategies leading to improved outcome and the survival outcomes including GFFS have not been investigated in Korea. Thus, this retrospective study was aimed to show the outcome of HSCTs in pediatric AA and to investigate prognostic factors for survival from a single institution over the last 25 years.
METHODS
Patients
From May 1, 1991 to December 31, 2018, 43 patients underwent allogeneic HSCTs at the Departments of Pediatrics, Chonnam National University Hospital (CNUH) and Chonnam National University Hwasun Hospital (CNUHH). And their medical records were reviewed retrospectively. Baseline clinicopathologic data from patients, such as age, sex, initial blood counts, cellularity of BM, and etiology were recorded. Characteristics regarding to transplantation, such as, donor type, stem cell source, the degree of HLA matching, interval from diagnosis to transplantation, number of transfusions before transplantation, the presence of preceding IST, conditioning regimen, GvHD prophylaxis, engraftment, chimerism status, the presence of major viral infections, the presence of acute and chronic GvHD, transfusion-dependency, the need for second transplantation, and survival were analyzed.
Diagnostic criteria
All HSCTs were performed in patients with SAA or very severe aplastic anemia (VSAA). The diagnosis of SAA required at least two of the following criteria: an absolute neutrophil count (ANC) of less than 0.5 × 109/L, a platelet count (PLT) of less than 20 × 109/L, or a corrected reticulocyte count of less than 1% in the presence of hypocellular BM.12 VSAA was reserved to patients when the neutrophil count was below 0.2 × 109/L.1 Chromosome breakage test was performed to exclude congenital/inherited AA. Patients with clonal cytogenetic anomalies were excluded in the study population.
Conditioning regimen and GvHD prophylaxis
The conditioning regimen has been modified over time based on the donor type and the degree of HLA match. Initially, patients were conditioned with intravenous cyclophosphamide 50 mg/kg/d given for 4 consecutive days with horse ATG (Atgam; Pfizer, New York, NY, USA) 30 mg/kg/day for 3 days.13 Additional procarbazine (12.5 mg/kg/day) was used in very early phase of the study. Since 2005, fludarabine (Flu)-based preparative regimen was used in most cases. The most prevalent preparative regimens in this study consisted of Flu 25 or 40 mg/m2 and cyclophosphamide (Cy) 750 mg/m2 for 4 days plus thoracoabdominal irradiation (TAI) 3 Gy the day before transplantation in matched related transplantation, and rabbit ATG (1.25 mg/kg/day for 4 days) was added in unrelated transplantation.
GvHD prophylaxis was continuous intravenous infusion of CsA (5 mg/kg/day) for matched related transplantation, or tacrolimus (0.03 mg/kg/day) plus short course of methotrexate (MTX) 15 mg/m2 at D+1, 10 mg/m2 at D+3, D+6, and D+11 for unrelated transplantation.
Supportive care
The patients were managed in a protective isolation room until the recovery of neutrophils. Immunoglobulin was administered every 3 weeks until 100 days after transplantation. Antifungals and pentamidine nebulizer were used to prevent infections. Donor chimerism was monitored at 1, 3, 6, 9, and 12 months after transplantation. Other routine measures of supportive care have been modified over the years. HLAs were initially serologically typed for Class I, but all HLA-A, -B, -C and -DRB1 were DNA typed since 2002.
Subgroup analyses
For patients with SAA or VSAA frontline HSCT was offered if there were MRDs. Salvage unrelated HSCTs were offered to the refractory/relapsed cases without MRDs after IST, while MRD transplants were performed in small number of cases of IST failure who initially presented with moderate diseases.
The patients were subdivided into subgroups by transplant strategies, mainly by conditioning regimens. The survival was evaluated as of December 31, 2018. Patients were censored at the time of the events or at time of last follow-up.
Outcome analyses
Complete response (CR) after IST or transplantation was defined as simultaneous fulfillment of the following: hemoglobin > 10 g/dL, ANC > 1.5 × 109/L and PLT > 100 × 109/L with evidence of normal hematopoiesis. Partial response (PR) was defined when the blood counts no longer met the diagnostic criteria of SAA, but still did not meet the criteria for CR. Patients who did not achieve CR or PR, or were transfusion-dependent at 3 months after transplantation were defined as non-responders.13
OS was defined as the time between transplantation and death from any cause or time of last contact. FFS was calculated from the date of transplantation to last follow-up or first event (death due to any causes, lack of response, relapse, clinical paroxysmal nocturnal hemoglobinuria, secondary malignancy, HSCT after IST whichever occurred first).7 GFFS was defined as the absence of grade 3–4 acute GvHD or chronic GvHD with systemic treatment in addition to the status of FFS.9
Engraftment failure was defined by failure to achieve neutrophil engraftment, as evidenced by ANC < 0.5 × 109/L on D+28 post-transplant.14 Graft failure after initial recovery of hematopoiesis was considered to be secondary graft failure. Donor-type aplasia was considered when patients had hypocellular BM with persistent cytopenia (hemoglobin < 8 g/L, neutrophils < 1.0 × 109/L, or platelets < 50 × 109/L) in full donor chimerism for > 6 months after achieving engraftment.15
Major acute complications including acute GvHD, cytomegalovirus (CMV) reactivation and disease, Epstein-Barr virus (EBV)-lymphoproliferative disease, hepatic veno-occlusive disease (VOD), and hemorrhagic cystitis after transplantation were documented and their incidences were compared among subgroups.
Statistical analysis
Continuous variables were compared using the Student's t-test and categorical variables were compared using the χ2 test of Fisher's exact test. Probabilities of survival were estimated using the Kaplan-Meier (K-M) method and were compared using the log-rank test. Prognostic variables were evaluated by multivariable analyses using a Cox regression proportional hazard model. P value < 0.05 was considered statistically significant. The software package SPSS version 21.0 (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses.
RESULTS
Patient characteristics
A total of 43 acquired AA patients underwent allogeneic transplantations and were enrolled in this study. The characteristics of the patients involved in this study are shown in Table 1. Of these, 24 (55.8%) were females with male/female ratio of 1:1.26. Median age at diagnosis was 8.2 years, median age at transplantation was 11.3 years, and the median time from diagnosis to transplantation was 1.3 years (0.1–19.6 years). The average length of follow-up was 7.1 years. The etiology was idiopathic in all but 1 case of EBV infection. Paroxysmal nocturnal hemoglobinuria (PNH) clones (> 1%) at the time of diagnosis were seen in only one case, but the patient did not have clinical symptoms. At the time of transplantation, all patients were either SAA (n = 30, 69.8%) or VSAA (n = 13, 30.2%).
Table 1
Patient characteristics at the time of transplantation
The details of transplantation characteristics, such as, type of donor, source of stem cells, median dose of harvested CD 34+ cells, conditioning regimen, GvHD prophylaxis and ABO incompatibility were described in Table 2. In related transplantations, all the donors were siblings. BM was the main source of donor cells throughout the study. There were two main backbones of conditioning regimens: Cy-based regimen followed by Flu-based one.
Table 2
Comparison of allogeneic transplantation characteristics by conditioning regimen
Data are presented as number (%) or median (range)
Cy = cyclophosphamide, Flu = fludarabine, RD = related donor transplantation, UD = unrelated donor transplantation, IST = immunosuppressive therapy, ATG = antithymocyte globulin, GvHD = graft-versus-host disease, CsA = cyclosporine, Tac = tacrolimus.
OS, FFS and GFFS according to different transplantation methods
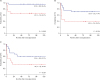
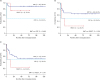
The 10-year K-M estimated OS, FFS, and GFFS for 43 allogeneic transplants were 86.0%, 60.5%, and 51.2%, respectively (Fig. 1). The OS, FFS and GFFS were compared between matched related and UDs (Fig. 2). MRD showed significantly better OS (96.4% vs. 66.7%; P = 0.006), FFS (71.4% vs. 40.0%; P = 0.014), and GFFS (60.7% vs. 33.3%; P = 0.031) than UD, respectively.
Fig. 1
The 10-year Kaplan-Meier survival rates for aplastic anemia patients who received allogeneic stem cell transplantation (n = 43). (A) OS, (B) FFS and (C) GFFS.
OS = overall survival, FFS = failure-free survival, GFFS = GvHD-free/failure-free survival.

Fig. 2
The 10-year Kaplan-Meier survival rates for aplastic anemia patients who received allogeneic stem cell transplantation by donor type. (A) OS, (B) FFS and (C) GFFS.
OS = overall survival, SD = sibling donor, UD = unrelated donor, FFS = failure-free survival, GFFS = GvHD-free/failure-free survival.
For stem cell source, BM was used in most cases (n = 37), while PB stem cells were used in 4 (all in unrelated settings), and umbilical cord in 2. The OS, FFS and GFFS of BM group were superior to those of PB, but not reaching the significant level, probably because of small numbers of PB group (OS, 89.2% vs. 75.0%, P = 0.468; FFS, 64.9% vs. 25.0%, P = 0.111; GFFS 54.1% vs. 25.0%, P = 0.171) in this study (Fig. 3).
Fig. 3
The 10-year Kaplan-Meier survival rates for aplastic anemia patients who received allogeneic stem cell transplantations by stem cell source. (A) OS, (B) FFS and (C) GFFS.
OS = overall survival, BMT = bone marrow transplantation, PBSCT = peripheral blood stem cell transplantation, CBT = cord blood transplantation, FFS = failure-free survival, GFFS = GvHD-free/failure-free survival.
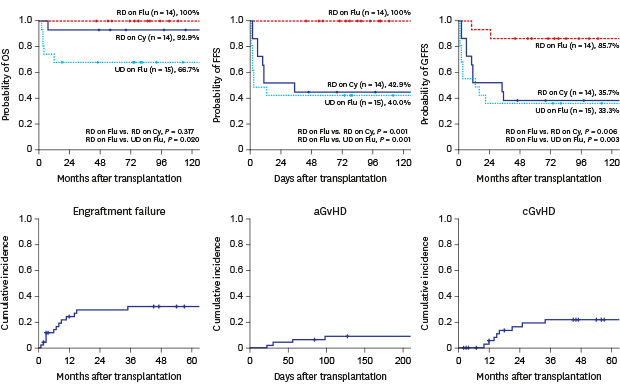
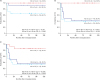
With regards to conditioning regimen, the K-M 10-year OS for 14 patients who received Cy-based conditioning was 92.9%, while that of 29 patients with Flu-based conditioning was 82.1% (P = 0.367) (Fig. 4A). But Flu-based conditioning tended to have better FFS and GFFS than those with Cy-based conditioning (Fig. 4B and C). Table 2 also compared characteristics of transplants by conditioning regimens. In Cy-group, all the cases (n = 14) were MRDs, while only 41.4% (12/29) of cases were MRDs in Flu-group (P = 0.019). As a frontline treatment, transplantation was performed in 22 patients (51.2%) for whom all had MRDs, and there was no up-front transplantation using UD. The remaining 21 patients received IST using ATG and CsA as a frontline treatment, which included SAA cases without MRDs (n = 8) and non-severe AA cases evolving to SAA later (n = 13). More patients received previous IST in Flu-group than in Cy-group (62.0% vs. 21.4%; P = 0.012). Ten patients (23.3%) received more than 40 transfusions before transplantation without any significant difference between the two groups. Irradiation was incorporated in the conditioning more commonly in Flu-group (26/29, 89.7%) than in CY-group (3/14, 21.47%; P < 0.001), but there were no considerable differences in FFS (66.5% vs. 50.0%, P = 0.324) and GFFS (55.2% vs. 42.9%, P = 0.433) between irradiation (n = 29) and non-irradiation group (n = 14), respectively. ATG was frequently used in the conditioning regimen in both groups (P = 0.198). The use of ATG in the conditioning regimens had a tendency of lower survival rates in OS (82.1% vs. 93.3%, P = 0.320), FFS (53.6% vs. 73.3%, P = 0.194), and GFFS (50.0% vs. 53.3%, P = 0.726), but they were not statistically significant. Also, the use of ATG was not associated with survival within Cy-based and Flu-based conditioning subgroups (data not shown).
Fig. 4
The 10-year Kaplan-Meier survival rates for aplastic anemia patients who received allogeneic stem cell transplantations by conditioning regimen. (A) OS, (B) FFS and (C) GFFS.
OS = overall survival, Cy = cyclophosphamide, Flu = fludarabine, FFS = failure-free survival, GFFS = GvHD-free/failure-free survival.
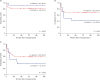
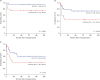
Fig. 5 illustrates the survival according to the donor type and the conditioning regimen. In related donor transplantation, OS was similar between Flu-group (92.9%, n = 14) and Cy-group (100.0%, n = 14), while FFS (100.0% vs. 42.9%; P = 0.001) (Fig. 5B) and GFFS (85.7% vs. 35.7%; P = 0.006) (Fig. 5C) were significantly better in Flu-group than in Cy-group. In UD transplantation (n = 15) including 2 cord blood transplants, all of whom received Flu-conditioning had OS of 66.7%, which was significantly lower than related donors with Flu-conditioning. However, the FFS and GFFS were quite similar between related donors with Cy-conditioning and UDs with Flu-conditioning.
Fig. 5
The 10-year Kaplan-Meier survival rates for aplastic anemia patients who received allogeneic stem cell transplantations by donor type and conditioning regimen. (A) OS, (B) FFS and (C) GFFS.
OS = overall survival, RD = related donor, Flu = fludarabine, Cy = cyclophosphamide, UD = unrelated donor, FFS = failure-free survival, GFFS = GvHD-free/failure-free survival.
The frontline transplantation group was superior to the frontline IST followed by transplantation group in OS, FFS, and GFFS (Fig. 6). Among them, FFS was statistically different (P = 0.041). Additionally, other factors such as the incorporation of irradiation in the conditioning, and method of GvHD prophylaxis (CsA- vs. tacrolimus-based) were compared for survival analyses, but they were not different.
Fig. 6
The 10-year Kaplan-Meier survival rates for aplastic anemia patients who received allogeneic stem cell transplantations by the use of previous frontline IST. (A) OS, (B) FFS and (C) GFFS.
OS = overall survival, IST = immunosuppressive therapy, FFS = failure-free survival, GFFS = GvHD-free/failure-free survival.
Engraftment failure and donor-type aplasia
Engraftment failure was seen in 13 patients with 30.2% of cumulative incidence: 8 after matched related transplant (8/28, 28.6%), and 5 after unrelated transplant (5/15, 33.3%; P = 0.746) (Fig. 7A). The median CD34+ cell doses of patients with stable engraftment and those with graft failure were not different (4.32 × 106/kg vs. 3.99 × 106/kg; P = 0.947). Primary graft failure was seen in only one patient, who was transplanted with 2 allele-mismatched BM of 2.3 × 106/kg of CD34+ cell dose. Secondary graft failure after achieving initial engraftment was seen in 12. Among the secondary graft failure, 10 patients showed evidence of donor-type aplasia, which was seen in 13.8% (4/29) after Flu-based conditioning, and in 42.6% (6/14) after Cy-based (P = 0.035). As a rescue, a 2nd transplantation was performed in 8 cases, resulting in survival in all 8. However, a 3rd transplantation was needed in 2, resulting in complete response and transfusion dependence in each. Among 13 patients with engraftment failure, 2 patients died: one with primary graft failure died of CMV disease, and the other with secondary graft failure after mismatched transplant refused further treatment. For 10 patients with donor-type aplasia, 7 were salvaged by 2nd transplant, 1 responded to IST, 1 on thrombopoietin receptor agonist, and the last is still dependent on transfusions.

Transplantation-related complications
Major complications were documented in Table 3 and their cumulative incidences were shown in Fig. 7. The cumulative incidences of acute GvHD (≥ Grade II) was 9.3% (Fig. 7B), whereas chronic GvHD requiring systemic treatment was 18.6% (2 in Cy-group and 6 in Flu-group (14.3% vs. 20.7%; P = 0.613) (Fig. 7C). The use of ATG was not associated with the incidence of acute GvHD (P = 0.388) and chronic GvHD (P = 0.401) (data not shown). The cumulative incidence of CMV reactivation was 20.9% (9/43), but CMV diseases including pneumonia and encephalitis were seen in 3 (7.0%), which were associated with fatalities. They were all after UD transplants, and ATG was used in conditioning in 2 cases. EBV lymphoproliferative disease was observed in one patient with MUD BM transplantation, but was successfully treated with rituximab. The cumulative incidence of hepatic VOD was 14.0% (6/43; 3/14 in Cy-group versus 3/29 in Flu-group; P = 0.326). The median onset of hepatic VOD was 9 days after transplantation. In one case, hepatic VOD developed 25 days after the second PBSCT after graft failure, which was 150 days after the first BMT. Severe hemorrhagic cystitis was seen in one case each from two conditioning regimens.
Table 3
Complications following allogenic stem cell transplantation by study period

Cause of deaths and prognostic factors
The characteristics of deaths after transplantation were described in Table 4. Six patients died (1 in Cy-group and 5 in Flu-group; P = 0.371). Except for one case (Pt. #1) who died of late graft failure following matched related transplant, the remaining 5 cases were transplanted from donors other than related donors and were pre-treated with IST. Four deaths were attributed to pneumonia in which two of them were due to CMV pneumonia. CMV encephalitis with intracranial bleeding was documented in a case.
Table 4
Characteristics and causes of deaths in transplanted aplastic anemia patients

IST = immunosuppressive therapy, OS = overall-survival, FFS = failure-free survival, Cy = cyclophosphamide, M = male, Flu = fludarabine, F = female, MRBMT = matched related bone marrow transplantation, mmUCT = mismatched umbilical cord blood transplantation, CMV = cytomegalovirus, mmUBMT = mismatched unrelated bone marrow transplantation, MUBMT = matched unrelated bone marrow plantation, ICH = intracranial hemorrhage, mmUPBST = mismatched peripheral blood stem cell transplantation, AKI = acute kidney injury, CKD = chronic kidney disease.
Prognostic factors were evaluated for OS, FFS, and GFFS by univariable and multivariable analyses (Table 5). Type of donor (odds ratio [OR], 10.975; 95% confidence interval [CI], 10.647–11.303; P = 0.029) and viral reactivation (OR, 10.266; 95% CI, 10.006-10.526; P = 0.008) after transplantation were found to be the independent factors in OS. For FFS and GFFS, number of prior transfusions and donor type were significant prognostic factors. The source of stem cells and the period of transplant before and after 2005 were not associated with OS, FFS, and GFFS (data not shown). Second transplantation was more commonly needed in patients conditioned with Cy (OR, 6.500; 95% CI, 6.256–6.744; P = 0.022). Likewise, donor-type aplasia was more frequently encountered in patients conditioned with Cy (OR, 4.687; 95% CI, 4.459–4.915; P = 0.043). Multivariable analyses showed that donor type was the prognostic factor in FFS, and GFFS. Viral reactivation in OS and the number of transfusions in FFS and GFFS were additional prognostic factors, respectively.
Table 5
Univariable and multivariable analysis of prognostic factors in allogeneic stem cell transplantation

DISCUSSION
Over the past 4 decades, bone marrow transplantation (BMT) from a MRD has been the treatment of choice for children with acquired SAA. The treatment algorithm was based on the age, severity of AA, and the availability of MRD.516 Recent studies in children have shown the OS rates exceeding 90% with BMT from MRD. IST using ATG and CsA has been considered as the first-line therapy for patients who lack a MRD, but those studies of IST also have shown comparable OS almost approaching 90%. However, FFS or event-free survival (EFS) after IST excluding deaths, lack of response, relapse, development of PNH, or secondary malignancy or HSCT showed only 3-year EFS of 33%, or 10-year FFS of 56%, respectively, which were significantly inferior to those after BMT from MRD.7 In the retrospective, multicenter study of Korean Society of Pediatric Hematology-Oncology (KSPHO) from 1991 to 2005, the 10-year OS after BMT for MRD was 92.2%, which was comparable to other studies, but OS after alternative donor transplants, mostly after failed IST showed 47.1%,11 which was less favorable than more recent studies, such as 78% OS after failed IST.17
Second-line treatment is considered when the AA patient is refractory to frontline IST or is showing evidence of relapse after initial response. The relapse has been reported in up to 30% of responders to IST. As a second-line treatment, 2nd course of IST or matched unrelated donor (MUD) HSCT is considered depending on the availability of donor and age of the patient. Re-treatment with rabbit ATG and CsA showed reasonable response rate of 65% in relapsed cases but only 30% in refractory cases to initial horse ATG treatment.18 Direct comparison of 2 second-line treatments, prospectively conducted by Japanese Society showed comparable 5-year OS (95.2% vs. 93.5%), but remarkable difference in FFS (9.4% vs. 83.9%; P = 0.001) after 2nd IST (n = 21) or HSCT from alternative donor (n = 31), respectively.19
The outcome of MUD transplantation has improved dramatically over the past two decades with better donor selection by DNA typing, better supportive care and experiences, showing comparable results with those of BMT from a MRD.1920 Excellent survival of 95% at 5 years was reported after MUD HSCT post IST using FCC conditioning regimen (Flu, Cy [120–200 mg/kg], and alemtuzumab). The lower rate of acute and chronic GvHD in the study was partially related to a superior depletion of alloreactive donor T-cells with alemtuzumab as compared with ATG.20 In a recent multicenter Korean study of MUD transplants a reduced-toxicity conditioning regimen (Flu, 200 mg/m2; Cy, 120 mg/kg; and ATG, 7.5 mg/kg) showed excellent OS (96.7% vs. 67.9%; P = 0.004) and EFS (93.3% vs. 64.3%; P = 0.008, respectively) as compared to the previous conditioning regimen (Flu, 120 mg/m2; Cy, 200 mg/kg; and ATG, 7.5 mg/kg).21
Encouraged by those excellent MUD transplants comparable to MRD transplants, researchers employed upfront UD transplants in SAA children without prior IST. UK study showed excellent 2-year OS (96%) and 2-year EFS (92%) in upfront UD transplants (n = 29) after FCC conditioning, similar to 91% and 87%, respectively, after MRD transplants (n = 87). The OS and EFS after MUD HSCT post IST failure were inferior (74% each). The median interval from the diagnosis to HSCT was only 0.37 (0.15–1.3) years.6 Another study from Korea showed excellent OS and EFS (91.3% each) after frontline alternative donor HSCT (n = 23), better than frontline IST group (n = 19) and salvage HSCT group (n = 11).10 Thus, upfront MUD transplants should be pursued if suitable MUD, preferably 10/10 match, is available especially in the case of unavailability of horse ATG.622
The development of acute and chronic GvHD has substantial effect on the quality of life of transplanted patients. Thus, GFFS, representing more ideal recovery after HSCT without ongoing morbidity, was recently introduced and evaluated in patients with hematologic malignancies and AA.923 In a Swedish retrospective study of 68 adult AA patients the 5-year OS was 86.8%, but GFFS was 69.1%. Patients aged ≥ 40 years had a higher transplant-related mortality, and lower 5-year OS (70.6% vs. 92.2%; P = 0.022), and a trend of lower GFFS (52.9% vs 74.5%; P = 0.069).24 A novel multicenter Chinese study of AA adults and children comparing upfront transplants showed excellent 1-year GFFS of 80.8% after haploidentical transplants, which was comparable to 88.4% after MRD transplants. Those results need to be reproduced in prospective studies to avoid selection bias.25 Thus, the current study is unique, real-world data evaluating GFFS in children with AA. GFFS was 51.2% in HSCT for 43 childhood AA patients, although OS was 86.0%. The best result of GFFS was seen in MSD transplantation with Flu-based conditioning (85.7%).
The standard conditioning regimen for MRD transplantation has been Cy (200 mg/kg) and ATG, showing excellent engraftment (95%) and long-term outcome (90% at 2 years) with reduced risk of GvHD.26 However, due to high dose Cy-related toxicity, such as, cardiotoxicity, infertility, and hemorrhagic cystitis, transition of conditioning regimen from Cy/ATG to Flu, Cy plus ATG or alemtuzumab has been observed. The OS and FFS were above 90% in children after reduced intensity FCC conditioning.20 Likewise, EBMT and British Society also recommend Flu-based conditioning regimen in adult cases.1227 The addition of low dose total body irradiation (TBI) or TAI to the standard conditioning seems controversial, as that may have a role in preventing graft failure, but may increase transplant-related morbidity and mortality.28
For the conditioning regimen in UD HSCT, the combination of Flu, Cy and ATG similar to those with MRD has been recommended from EBMT studies.29 The dose of Cy was originally set at 300 mg/m2 × 4, but the dose of Cy was increased to 120 mg/kg because of the significant risk of rejection. Low dose TBI, 2 Gy or 3 Gy has been added to reduce rejection following the American and Japanese studies.3031 Furthermore, the addition of low dose TBI was regarded as one of the factors attributable to excellent OS after MUD HSCT, which was not statistically inferior to that of MRD transplants.13 However, the beneficial effect should be weighed against the increased risk of second malignancies, infertility, growth failure and endocrine dysfunction. And another encouraging conditioning regimen is Flu (100–180 mg/m2), melphalan (70–180 mg/m2) and ATG by a Japanese Group. The OS and EFS were comparable to Flu/Cy-based conditioning.32
In this study, there were considerable changes in transplantation techniques which included donor/recipient HLA matching, conditioning regimen, infection prophylaxis, and supportive care. Among them, various conditioning regimens have been used over time. However, Cy-based conditioning was substituted by Flu plus Cy in most cases since 2005. There was a discrepancy in survival rates. The higher OS of Cy-group was because all of them were MRD transplants (Fig. 2A). But, Flu-based conditioning tended to have better FFS and GFFS than those with Cy-based conditioning, which might reflect better quality of life despite less favorable characteristics of Flu-group, such as less proportion (41.4%, 12/29; P = 0.019) of MRDs and higher proportion of previous IST (62%, 18/29; P = 0.012). These findings were in line with previous study showing less rejection with improved survival.
Graft failure has been a significant obstacle to a successful transplantation for SAA. The etiology is complex and very frequently multifactorial. Non-malignant diseases, such as AA seem to have higher incidence, but other factors including HLA mismatches, previous transfusion history, low CD34+ cell count, reduced intensity conditioning, graft source, viral infections, GvHD, drug toxicity, and others may be implicated. The cumulative incidence of graft failure was 15%–17% after MUD HSCT.293031 The EBMT study reported the incidence of 17% after Flu, Cy and ATG with or without low dose TBI conditioning for alternative donor transplants after IST failure 29. Graft rejection was found in 10% after MSD and 8% after UD HSCT for AA patients.33
The high incidence of graft failure (13/43; 30.2%), mostly with secondary graft failure (n = 12) in our study needs to be improved. The transition from Cy-based conditioning to Flu-based conditioning resulted in the incidence of secondary graft failure from 42.6% after Cy-based conditioning to 13.8% after Flu-based conditioning (P = 0.035). Other measures including better HLA typing by DNA methods, better supportive care against viral infection and GvHD, shorter interval from diagnosis to HSCT with less transfusions, and incorporation of TBI in conditioning in most cases may have contributed to reduced incidence of graft failure in recent years. However, the presence of donor-specific anti-HLA antibodies (DSA) was not evaluated routinely in this study. Found in 10%–40% of cases, those antibodies are known to be associated with higher risk of graft rejection, especially in CB transplant and URD transplant settings.34
Donor-type aplasia with poor graft function was seen in 23.3% (10/43) in our study. The incidence was decreased from 42.6% (6/14) after Cy-based conditioning to 13.8% (4/29) after Flu-based conditioning (P = 0.035). On the other hand, a Japanese pediatric study (n = 660) showed the cumulative incidence of donor-type aplasia in 5.7% of AA cases with the predominance in Flu-based conditioning than in non-Flu group (11.6% vs. 2.7%; P < 0.001).35 Another Japanese study including AA patients (n = 26), and refractory cytopenia of childhood (RCC) patients (n = 24) showed the cumulative incidence of donor-type aplasia in 16% (8/50). It was found in 40% (6/15) after Flu/Cy conditioning regimen with low dose TBI, but in 6.5% (2/31) after Cy conditioning regimen with or without TBI (P = 0.003). And it was more frequently seen in RCC patients (32%), which was found to be a significant risk factor (hazard ratio, 7.7; P = 0.013) by multivariable analysis.15 The high percentage of donor-type aplasia may need retrospective morphologic review to exclude the inclusion of RCC cases in this study.
The preferred stem cell source for all patients with AA including URD HSCT should be unmanipulated BM, as the use of PB stem cells is associated with an increased risk of chronic GvHD, and inferior outcome despite the earlier engraftment. Other factors found to positively affect OS after MUD HSCT were age ≤ 30 years, transplant within the first year after diagnosis, and CMV status.13
As the presence of significant GvHD may jeopardize the quality of life, trials to decrease the incidence of GvHD have been attempted. ATG has been suggested to reduce high grade acute or chronic GvHD. In a recent meta-analysis, grade III/IV acute GvHD (risk ratio [RR] 0.52; 95% CI, 0.34–0.81; P = 0.004), and chronic GvHD (RR, 0.52; 95% CI, 0.40–0.69; P < 0.001) were decreased with the use of ATG.36 However, the use of ATG was not significantly associated with reduced incidence of acute GvHD (P = 0.388) and chronic GvHD (P = 0.401), or improved survival including GFFS (P = 0.726) in this study, probably because of small number and heterogeneity of our study. A retrospective study in the UK comparing ATG and alemtuzumab conditioning showed similar results but lower chronic GvHD in the alemtuzumab group (11% vs. 26%; P = 0.031).33 In the setting of MSD BMT, the use of rabbit ATG (8 mg/kg) in the conditioning showed protective effects against Grade II–IV acute GvHD, and moderate and severe chronic GvHD as compared with the use of horse ATG (90 mg/kg).37
This study reviewed the outcomes of transplantation for pediatric AA along with changes of transplant strategies over last 25 years. The predominance of MRD transplants with Cy-based conditioning has evolved to increasing number of URD transplants, Flu-based conditioning, incorporation of irradiation, tacrolimus-based GvHD prophylaxis, and better supportive care. The FFS and GFFS tend to be higher in Flu-based conditioning group than in Cy-based group, especially in related transplantation, which may reflect better quality of life, although unfavorable factors were more frequent in the Flu-based group. Also, OS was quite comparable between 2 groups. However, systemic evaluation of quality of life by performance scales was not available in this retrospective study.
Graft failure including donor-type aplasia remains troublesome throughout this study. Change to Flu-based conditioning, incorporation of irradiation, the use of PB stem cells in some MUD transplants, all resulted in some reduction of graft failure, but the incidence is still high. Routine analysis of donor-specific anti-HLA antibodies, morphologic exclusion of RCC, better control of concomitant infections, and more effective GvHD control might be attempted to ensure stable, solid engraftment in patients with AA. Most importantly, either increase of Cy dose to 200 mg/kg, or change of conditioning regimen to Flu, Mel, ATG +/– irradiation should be considered to further decrease graft failure in our institution. These changes might be translated into improved FFS, and GFFS after transplant. Further efforts to minimize long-term complications, including radiation-related consequences should be pursued in the future.
 XML Download
XML Download