

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The 48/6 Model of Care is an integrated care initiative developed for hospitalized seniors in Canada that addresses 6 areas of functioning through patient screening and assessment.1 Screening and/or assessments (assessments are completed only where screening shows areas of concern) are then supported by the development of an individualized care plan to address key areas of health for the senior. Based on this process, healthcare teams can implement a personalized, documented care plan within 48 hours of the decision to admit. The six care areas are composed of common clinical issues related to older adults’ health. These are bowel and bladder management, cognitive functioning, functional mobility, medication management, nutrition and hydration, and pain management. The 48/6 Model of Care aims to prevent functional decline and in-hospital comorbidity in the senior population, which can help patients return home sooner at the level of independence that they had prior to admission through the screening of hidden problems for the six care areas within 48 hours of admission.
Mobility is a critical component of the assessment of function and disability in older adults because it is strongly related to the maintenance of autonomy and independence.23 Mobility is frequently assessed by performance based (e.g., gait speed, timed up and go test, or short physical performance battery [SPPB])45 or self-reported (e.g., ability to walk a quarter of a mile)6 measures. Although these measures are informative and valid, they may not capture the full scope of older adults' mobility in the community (e.g., how far they actually travels, need and availability of assistance).
The concept of life-space emerged as a complementary tool to the traditional measures of mobility to assess how much (how often and how far) a person actually moves around in their own environment using available resources.37 Measures of life-space reflect person's mobility by not only assessing their physical and geographical capacities, but also the need for type and degree of assistance to move around in their home and beyond.3 Available instruments for assessing life-space mobility include the Life-space diary,8 nursing home life-space diameter,9 Life Space Questionnaire,10 indoor life-space mobility at home,11 and Life-Space Assessment (LSA).3 Among these, the LSA is perhaps the most widely used valid and reliable tool for older adults, and has been translated into several languages.121314151617 Life-space mobility measured by LSA is correlated with physical performance assessed by SPPB, difficulty in activities of daily living, and self-reported health by 5-point Likert scale.7 Furthermore, declines in life-space mobility are associated with declines in quality of life (QOL) assessed by short version of the World Health Organization QOL scale.18 In that study, the decrease in QOL score was somewhat higher among those whose life-space mobility score declined > 10 points during a 2-year follow-up compared to those whose life-space remained stable or improved, even after adjustment for age, gender, number of chronic conditions, cognitive impairment, SPPB and education.
Previously, we introduced a modified version of the 48/6 Model of Care by adapting the Canadian care process.192021 The 48/6 Model of Care was primarily designed for use with hospitalized older adults, and its applicability in a community setting has not yet been reported. As with hospitalized older adults, the first step in applying the 48/6 Model of Care in a community setting would be screening for problems in the 6 care areas. We hypothesized that a screening tool based on the 48/6 Model of Care would be effective in screening for these problems in community-dwelling older adults as well as hospitalized older patients. Thus, the present study investigated the applicability of the 48/6 Model of Care, prevalence of dysfunction in 6 care areas, and its relationship with self-reported life-space mobility in community-dwelling older adults.
Go to : 
METHODS
Study design and participants
A cross-sectional community survey study was conducted between October and November 2016. Four hundred and forty-four adults were recruited. Three quarters (333) of the participants were recruited via street-intercept survey in Gwangjin-gu, Seoul, Korea, while one quarter was surveyed through a home visiting health care service for vulnerable populations, which was based from a public health center also in Gwangjin-gu, Seoul, Korea. The inclusion criteria were an age of 65 or older, had the ability to respond to the survey, and gave their written informed consent. The adults who could not complete the survey were excluded.
Study variables
Sociodemographic variables
Age, gender, education, family state, income, and comorbidities were assessed by self-report. The comorbidities included hypertension, diabetes, stroke, ischemic heart disease, cancer, chronic kidney disease, chronic lung disease, arthritis, and other.
Screening for six areas of the 48/6 Model of Care
The six care areas of the 48/6 Model of Care were cognitive function, functional mobility, pain management, nutrition and hydration, bowel and bladder management, and medication management. The screening questionnaire was originally developed to identify any dysfunction in 6 care areas among inpatient populations by the multidisciplinary focus group of geriatricians, neurologists, physiatrists, psychiatrists, and family physicians, geriatric nurses, and patients.1920 We used the same screening questionnaire for this study.
The screening questionnaire comprises 9 items for 6 care areas, because of the need for proper and specific screening. For example, cognitive function was divided into cognitive impairment and depression. The nutrition and hydration care areas asked about dysphagia and weight loss. Also, bowel and bladder symptoms were separately assessed. Unlike the questionnaire for the hospitalized older patients that was named as Geriatric Screening for Care 10,1920 it did not contain delirium questions.
The specific items were as follows:
• Cognitive impairment, “Have you felt a marked decrease in judgement or memory loss over the past year?”
• Depression, “Have you often felt sad or depressed in the last week?”
• Functional mobility, “Can you climb up stairs independently?”
• Pain, “Have you had pain more than one day in the last 2 weeks?”
• Dysphagia, “Have you had difficulty in swallowing liquids or foods in the last 2 weeks?”
• Weight loss, “Have you experienced unintentional weight loss in the last 6 months?”
• Urinary incontinence, “Have you experienced accidental leakage of urine in the last month?”
• Fecal incontinence, “Have you experienced accidental bowel leakage in the last month?”
• Polypharmacy, “Are you currently taking five or more medications?”
For each item, answering “yes” was considered to indicate a dysfunction, except for functional mobility, where an answer of “No” was defined as impaired mobility.
All participants were interviewed by the surveyor to complete the screening questionnaire. The time to complete the survey was about 15–20 minutes. Dysfunction in each item of the questionnaire and the total number of dysfunction were recorded for each participant.
Measurement of life-space mobility
Life-space mobility was assessed using the translated version of the LSA.22 Conceptually, life-space is a concentric pattern of zones radiating outwards from a person's usual abode.3 The LSA evaluates six levels of life-space, ranging from the person’s bedroom (Level 0) to places outside of the person's town (Level 5).7 The following questions were used to assess life-space mobility: “During the past 4 weeks, have you been to 1) other rooms of your home besides the room where you sleep; 2) an area outside your home such as a porch, deck, patio, the hallway of an apartment building, or garage; 3) places in your neighborhood, other than your own yard or apartment building; 4) places outside your neighborhood but within your town; and 5) places outside your town?’’ The frequency of movement and use of assistance were also assessed for each level (“How often have you been there?” and “Did you use aids or special equipment to get to there? Or did you need help from another person to get to there?” respectively).
A composite measure of life-space (LS-C) was calculated using the components of life-space level, frequency, and degree of independence. Specifically, this measure was calculated for each level by multiplying the life-space level (1–5) by the frequency (1, less than once a week; 2, 1–3 times a week; 3, 4–6 times a week; and 4, daily) and degree of independence (2, independent [i.e., no assistance from persons or equipment was necessary]; 1.5, equipment was used; and 1, personal assistance was necessary). The total score ranges from 0, which indicates that one is completely restricted to one’s bedroom, to 120, which indicates that one independently travels outside of town daily. Additionally, simple scores of life-space were assigned according to the highest level attained, without considering frequency of movement. Specifically, we assessed the maximal life-space (LS-M; range, 0–5), the highest life-space level attained regardless of whether equipment or help from a person was used; the independent life-space (LS-I; range, 0–5), the highest life-space level attained without help from a person and without using any equipment; and the restricted life-space (LS-ID), which was a dichotomous measure that classifies individuals as having a restricted (confined to one’s neighborhood) or an unrestricted independent life-space.7
Statistical analysis
Data were analyzed using SPSS Statistics 17.0 (SPSS Inc., Chicago, IL, USA). Demographic variables were analyzed via descriptive statistics. Linear-by-linear association test was conducted for comparison of prevalence of dysfunction identified in 48/6 screening questionnaire by age groups, and Kruskal-Wallis test for comparison of LSA scores by age groups. The relationships between the items corresponding to the six care areas of the 48/6 Model of Care and LSA scores were analyzed by Mann-Whitney U test. Correlations between the number of screened problems and LSA scores were examined using Spearman's correlation coefficients. Finally, a multiple regression analysis was conducted to examine the independence association between the specific item of 48/6 Model of care and LS-C. After confirming the significant association by univariate linear regression, the multivariate regression model was generated for all items of 48/6 Model of Care except impaired mobility due to collinearity between this item and life space variable. A normality test was preceded before stated statistical analyses for all data. The statistical significance level was set at P < 0.05.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Konkuk University Medical Center (approval No. KUH1170136). Written informed consent was obtained from all individual participants included in the study.
Go to :
RESULTS
Sociodemographic characteristics
Table 1 shows the sociodemographic characteristics of the enrolled older adults. The distribution of participants by age (in 5-year increments) was nearly even, and 58.6% were women. One-hundred and six participants (23.9%) were working. Almost half of participants were living with their spouse. Furthermore, the mean number of comorbidities was 1.8 ± 1.4.
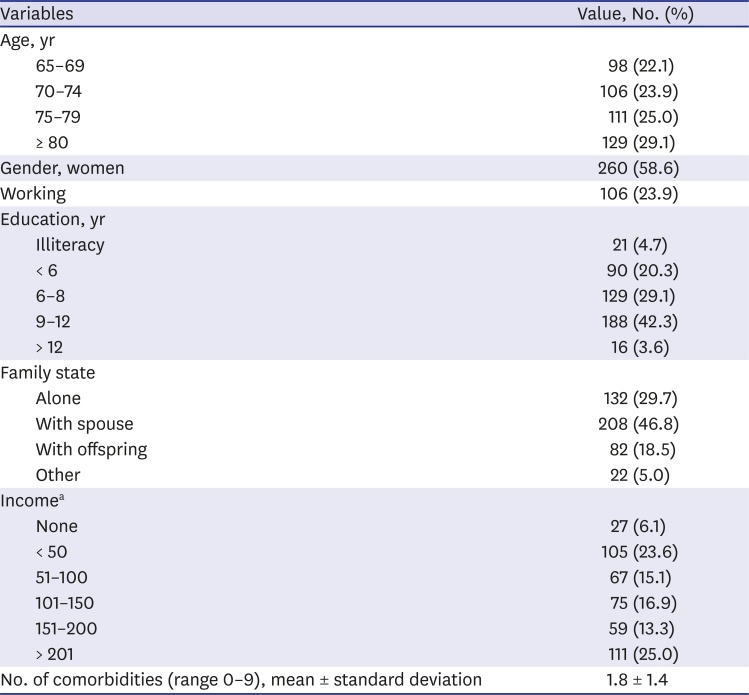
Table 1
Sociodemographic characteristics
![]()
Prevalence of dysfunction identified in screening questionnaire
The results of the screening for the 6 care areas of the 48/6 Model of Care are described in Table 2. The most prevalent dysfunction was pain (45.0%), followed by cognitive impairment (38.3%) and urinary incontinence (34.0%). The total number of dysfunction ranged from 0 to 9 with the mean value of 2.3 ± 2.1. Three hundred and twenty-six (73.4%) participants reported dysfunction in at least one item. Further, 264 (59.5%) reported dysfunction in ≥ 2 items and 178 (40.1%) in ≥ 3 items. Also, subgroup analysis revealed that most problems had increased with advanced age, and the prevalence of each dysfunction was significantly different between age groups except urinary/fecal incontinences.
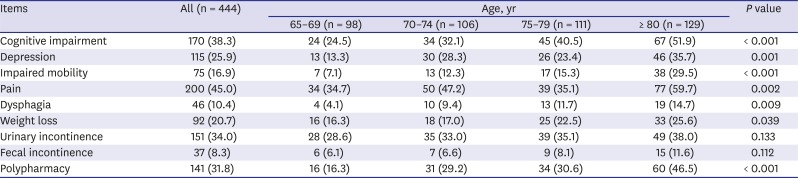
Table 2
Prevalence of dysfunction for 6 care areas
![]()
Life-space mobility
Table 3 shows the results of the LSA for all participants and subgroup analysis by age. The mean LS-C score was 58.3 ± 27.7, 4.7% were able to travel unlimitedly without personal or device assistance (LS-C score of 120), and 12.4% exhibited a restricted life-space (i.e., their independent life-space was confined to their neighborhood). Additionally, LS-C score, maximal life-space, and independent life-space were significantly restricted in order of age.
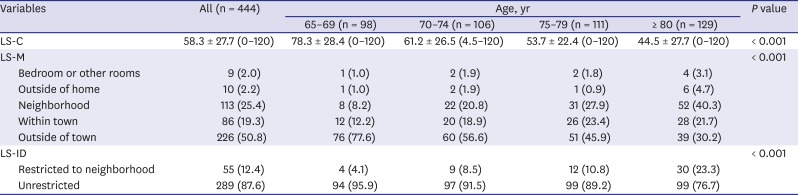
Table 3
LSA scores
Data are presented as mean ± standard deviation or number (%).
LSA = life-space assessment, LS-C = composite measure of life-space, LS-M = maximal life-space, LS-ID = restricted life-space.
![]()
Association between the 48/6 Model of Care results and life-space mobility
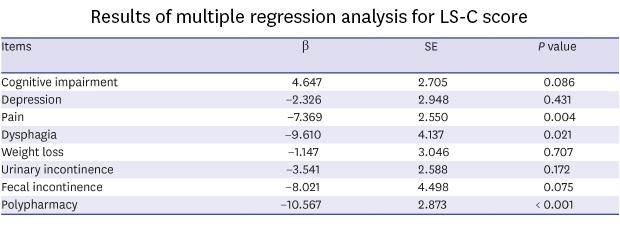
The LS-C score according to the presence of problems for each item of the 48/6 Model of Care is provided in Table 4. Notably, all items were significantly associated with LS-C score. Also, a greater number of total dysfunction was associated with significantly lower LS-C score (Spearman's rho, −0.468; P < 0.001). A multiple linear regression analysis was conducted to identify items associated with the LS-C score, including age as a covariate (Table 5). After controlling for age and other factors, polypharmacy (β = −10.567; standard error [SE], 2.873; P < 0.001), dysphagia (β = −9.610; SE, 4.137; P = 0.021), and pain (β = −7.369; SE, 2.550; P = 0.004) were still significantly associated with life-space mobility.
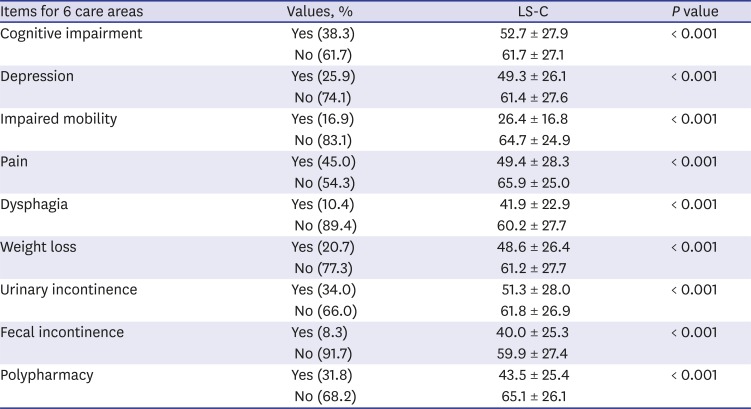
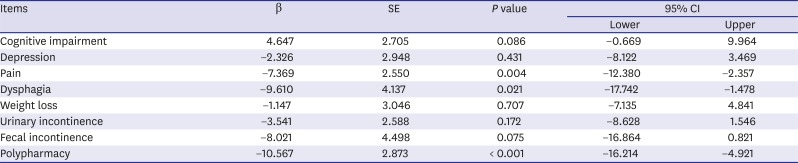
Table 4
LS-C score according to the presence of screened problem
![]()
Table 5
Results of multiple regression analysis for LS-C score
![]()
Go to :
DISCUSSION
As stated before, the 48/6 Model of Care was designed to improve the care quality of hospitalized seniors by addressing six areas of functioning: bowel and bladder management, cognitive functioning, functional mobility, medication management, nutrition and hydration, and pain management. It comprises screening and assessment, followed by devising an individualized care plan for the detected problems within 48 hours of admission. It is further supported by a discharge or transition plan to ensure that older adults can return to the community safely.1
In this study, we examined the prevalence of problems in these 6 care areas in community-dwelling older adults using the established questionnaire for hospitalized population, based on the idea that the model should be applied as part of the continuum of care from the hospital to community. Most participants (73.4%) included in this study had one or more problems among the 9 items corresponding to the 6 care areas. Furthermore, all 9 items showed a rather high prevalence, ranging from 8.3% to 45.0%, with pain, cognitive impairment, and urinary incontinence being most common problems. Expectably, most problems including urinary/fecal incontinences, although they did not have statistical significance, revealed increased prevalence in order of age.
Several geriatric health screening tools are currently used in both hospital and community settings. For instance, the Flemish version of the Triage Risk Screening Tool (fTRST) was developed to identify older emergency department patients who are at risk for emergency department revisits, hospitalization, or nursing home admission.23 The fTRST is 5-item screening tool that assesses cognitive impairment, caregiver, mobility, hospitalization, and polypharmacy. The total score can range from 0 to 6,24 and a cut-off score of 2 is known to indicate increased risk of subsequent emergency department use, hospitalization, and nursing home admission.23 The Vulnerable Elders Survey-13 (VES-13) was developed to identify community-dwelling older people at risk of death or functional decline.25 The VES-13 utilizes a 13-item function-based scoring system and asks for their age, physical status, functional capacity, and self-rated health.26 Scores range from 0 (lowest risk for functional decline) to 10 (highest risk).27 Patients who have scores of 3 or higher were identified as having a 4.2-fold greater risk of functional decline or death over a 2-year period compared with patients who had scores of < 3.25 However, some investigators have found that it is overvalued as a screening tool for vulnerability.28 Next, the G-8 is a geriatric screening tool used to identify older cancer patients who would benefit from comprehensive geriatric assessment (CGA).29 It contains 8 items, including seven items from the Mini Nutritional Assessment questionnaire and a question about age. The total score can range from 0 to 17, and is considered abnormal if the score is ≤ 14, which indicates a geriatric risk profile.24 The G-8 shows good screening properties for identifying older cancer patients who could benefit from CGA.29 It also has prognostic value for functional decline and overall survival.24 However, these geriatric screening tools are designed to identify populations that need further evaluation or to predict the functional outcomes using cut-off values. Although they include some of the 6 key care areas of the 48/6 Model of Care, most do not contain items for pain, bladder, and bowel management which has high implications in QOL of an individual.
On the other hand, the screening questionnaire used in this study includes multiple domains, and each item was selected with the consideration of developing a care plan after screening. The substantial prevalence of dysfunction in the 6 care areas observed in the present study means that further care plans after screening would be needed in community-dwelling older adults. In other words, if timely referral is made after screening with the 48/6 Model of Care at the community level, it might be helpful in preventing the functional decline.
Life-space mobility assessed by LSA was significantly restricted with advanced age. Also, life-space mobility was associated with problems in all 9 items of 6 care areas. Additionally, as the number of screened problems increased, the life-space showed a significant reduction. This is perhaps explained by the fact that cognitive function, pain, nutritional status, and incontinence all affect life-space as well as mobility. Furthermore, polypharmacy may reflect the presence of comorbidities that limit life-space. Notably, polypharmacy, dysphagia, and pain had particularly strong correlations with life-space mobility after controlling for age. Thus, it seems important to establish appropriate assessment and intervention plans that resolve these specific problems after screening with the 48/6 Model of Care, as it could help improve mobility in community-dwelling older people.
The present study has several limitations. First, participants included in this study are not representative of all community-dwelling older adults. Indeed, a relatively high proportion (one-fourth) of participants were utilizing a home visiting health care service for vulnerable populations. Therefore, the generalizability to healthier population may be limited. Second, the identified problems using this screening questionnaire should be verified with further assessments before arranging a care plan, as the questionnaire cannot be considered diagnostic.
We demonstrated that the screening of functional impairment using 48/6 Model of Care is feasible. Dysfunction in 6 areas of 48/6 Model of Care is highly prevalent among older individuals living in a community and it correlates with the extent of mobility of individuals in the community. This tool can be applied effectively to screen for the health status of community-dwelling older adults, and may be useful for estimating life-space mobility. Future studies that focus on assessments and care plans for identified dysfunction at the community level will be needed to further advance the implementation of this model in practice.
Go to :
 XML Download
XML Download