

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cervical insufficiency may be present in approximately 0.5%–1% of obstetric populations and is an important cause of early spontaneous preterm delivery (SPTD) or second-trimester pregnancy loss.1234 The impact of this disease on adverse pregnancy and perinatal outcomes, even when treated with a cerclage, is closely related to the occurrence of subclinical intra-amniotic infection.5678 Therefore, considering a reported rate of up to 50% for intra-amniotic infection,9 a more precise prediction of the risk of intra-amniotic infection and SPTD, particularly by non-invasive tests, is clinically important for the counseling and clinical management of patients with cervical insufficiency.
Traditionally, several markers associated with pregnancy outcomes in cervical insufficiency have been identified through the analyses of amniotic fluid (AF).57101112 However, the assessment of these markers in the AF may be currently of limited clinical usefulness because obtaining AFs itself is invasive. In this context, a less invasive test based on analyzing these proteins in the mother's blood could provide a safe and attractive alternative to amniocentesis, considering that several reports have shown that intra-amniotic infection and SPTD are associated with simultaneous increases in the levels of several cytokines and chemokines in maternal blood and AF compartments in cases of preterm labor and preterm premature rupture of membranes.13141516 However, to our knowledge, the role of immune-related proteins in maternal blood samples in the prediction of intra-amniotic infection and SPTD in women with cervical insufficiency has not been reported to date.
Cervical insufficiency/sufficiency is generally recognized as a continuum on the basis of cervical length measurement using transvaginal sonography; in addition, a mid-trimester shortened cervix is correlated with an increased risk of cervical insufficiency and/or possible subsequent SPTD.1718 This study aimed to determine whether the tissue inhibitor of metalloproteinases (TIMP)-1, C3a, C5a, interleukin (IL)-6, and matrix metalloproteinase-9 (MMP-9) levels in the plasma, either alone or in combination with conventional clinical risk factors, can predict SPTD and intra-amniotic infection in women with premature cervical dilation (previously termed a cervical insufficiency) or a short cervix (≤ 25 mm). Additionally, we also compared the plasma levels of the aforementioned proteins in women with short cervix and with premature cervical dilation.
METHODS
Study population
A retrospective cohort study was conducted on consecutive singleton pregnant women presenting with premature cervical dilation or a short cervix (≤ 25 mm) at 17 to 29 weeks gestational age who were admitted at Seoul National University Bundang Hospital (Seongnam, Korea), a tertiary-care teaching hospital, from September 2004 to February 2015. Most patients enrolled in the current study were transferred from the local hospital (n = 64, 80%) where they were first presented to our tertiary care center for further management. The remaining patients received routine antenatal care at baseline at our institution and were thereafter diagnosed with premature cervical dilation or short cervix. Inclusion criteria included the following: 1) a live fetus; 2) intact amniotic membranes; 3) trans-abdominal amniocentesis performed for evaluation of microbiologic and inflammatory status of the amniotic cavity based on the reports showing that the prevalence of intra-amniotic infection and intra-amniotic inflammation is 50% and 40%, respectively, in women with cervical insufficiency and 10% and 22% in women with a short cervix, respectively591920; 4) maternal plasma (1 aliquot) available for analysis; 5) absence of premature contractions, preterm labor or clinical signs of chorioamnionitis at the time of diagnosis; 6) no history of prior cervical cerclage; and 7) absence of major fetal congenital anomalies. Several clinical data (but not the laboratory data measured in the plasma samples) contained in this manuscript have been published in PLoS One (n = 31), Arch Gynecol Obstet (n = 56), and J Korean Med Sci (n = 65).82122 For determining gestational age, we used both the last menstrual period and an ultrasound scan performed in the first or second trimester. The main outcome measures were SPTD at < 32 weeks and intra-amniotic infection (defined as the presence of a positive AF culture for microorganisms).
AF, sample collection and preparation
Upon admission, transabdominal amniocentesis was performed under sonographic guidance with the use of antiseptic skin preparation. AF samples were immediately transported to the microbiological laboratory to culture aerobic and anaerobic bacteria, Ureaplasma urealyticum, and Mycoplasma hominis, following previously described methods.23 Maternal blood samples were usually obtained within 2–3 hours of amniocentesis and collected into ethylenediaminetetraacetic acid tube. Serum C-reactive protein (CRP) level was also measured in the maternal blood samples. The samples were centrifuged at 1,500 g at 4°C for 10 minutes, and the supernatant was aliquoted for storage at—70°C until assay. Managing physicians had access to results of the AF culture and CRP level.
Inflammatory and immune mediator assays in plasma
The following immune-related proteins levels were determined in the stored plasma samples using ELISA kits: MMP-9, TIMP-1 (DuoSet ELISA from R&D System, Minneapolis, MN, USA), complement C3a and C5a (BD Biosciences, San Diego, CA, USA), and IL-6 levels (R&D System). The ELISA assays were carried out by strictly following the manufacturer's instructions provided. The ranges of the MMP-9, TIMP-1, C3a, C5a, and IL-6 standard curves were 31.2–2,000 pg/mL, 31.2–2,000 pg/mL, 0.078–2.5 ng/mL, 0.08–2.5 ng/mL, and 0.2–10 pg/mL, respectively. Prior to measurement of these proteins, the plasma samples were diluted at 1:5 for high sensitivity IL-6, 1:10 for C5a, 1:500 for MMP-9 and TIMP-1, and 1:5,000 for C3a. The intra- and inter-assay coefficients of variability (CVs) were < 10% for the analyzed proteins, except for C5a; the intra- and inter-assay CVs were 14.7% and 15.7%, respectively.
Definition, diagnosis, and management of premature cervical dilation or a short cervix
Premature cervical dilation was defined as a painless dilation of the cervix (≥ 1 cm) with exposed amniotic membranes, as assessed during sterile speculum examination, without evidence of uterine contractions. A short cervix was defined as a cervical length of ≤ 25 mm measured by transvaginal ultrasound. The methods of sonographic cervical length measurement were previously described in detail elsewhere.24 Our protocol for management of women with premature cervical dilation or a short cervix was published previously.78 The decisions regarding the placement of a cervical cerclage, progesterone supplementation, amniocentesis, antibiotic treatment, and tocolytic administration at the time of cerclage placement depended on the discretion of the attending obstetrician. Medications (i.e., tocolytics, antibiotics, and corticosteroids) were administered after amniocentesis. Acute histologic chorioamnionitis was diagnosed in accordance with previously proposed criteria.25 Clinical chorioamnionitis was diagnosed based on the criteria proposed by Gibbs et al.26
Statistical methods
Continuous variables were compared using Mann-Whitney U test or Student's t-test, as appropriate. Categorical variables were compared using χ2-test or Fisher's exact test. The normality of the data was tested using Shapiro-Wilk test. A multivariate logistic regression analysis using the forward stepwise technique was performed to determine the best combination model for SPTD prediction. Continuous variables were examined, using a link test, for linearity in the logit.27 The significant univariate variables (P < 0.05) were entered into the logistic regression model, and the same P value was required for the final inclusion in the model as a threshold of significance. The Hosmer-Lemeshow test was used for assessing the goodness of fit of the models. Receiver-operating characteristic (ROC) curve analyses were performed with each protein in the plasma and predicted probabilities (C statistic) for the prediction of SPTD derived from the regression model and were used to select optimal cutoff values for each variable. The area under the curves (AUCs) were compared for each protein in the plasma and best combination model using DeLong et al.'s28 method. A Spearman's rank correlation test was used for analysis of correlation among the continuous variables. All reported P values were two-sided, with a significance level of 0.05. All analyses were computed using the SPSS for Windows version 21.0 (IBM SPSS Inc., Chicago, IL, USA).
Ethics statement
The Institutional Review Board of Seoul National University Bundang Hospital approved this study (project No. B-1311/228-010). The patients provided written informed consent for the amniocentesis procedure and collection and use, for research purposes, of maternal blood samples and clinical information.
RESULTS
During the study period, a total of 80 women with a diagnosis of premature cervical dilation (n = 50) and a short cervix (n = 30), who met met the inclusion/selection criteria, were included in the final analysis. The mean gestational age at the time of sampling was 22.2 ± 2.6 weeks (range, 17.3–29.1 weeks). SPTD at < 32 weeks of gestation occurred in 48.8% (39/80) of patients. The overall rate of positive AF cultures was 15.0% (12/80). Among these 12 women with positive AF cultures, U. urealyticum was isolated from the amniotic cavity in 11 women, M. hominis in seven, and Streptococcus viridans in one. Polymicrobial invasion was present in seven of the 12 patients (58.3%).
The levels of plasma IL-6, MMP-9, and TIMP-1 were significantly correlated with each other (all variables, r = 0.286–0.321, P < 0.05), but correlated with neither the level of plasma C3a nor the level of C5a (all r = −0.100 to 0.206, P > 0.05). The C3a and C5a levels in the plasma were significantly correlated (r = 0.536, P < 0.001). The serum CRP level was significantly correlated with the plasma IL-6 level (r = 0.487, P < 0.001), C3a level (r = 0.290, P = 0.01), and C5a level (r = 0.241, P = 0.03), but not with the level of MMP-9 (r = 0.193, P = 0.091) or TIMP-1 (r = 0.085, P = 0.459). Cervical dilatation was significantly correlated with the plasma C3a level only (r = 0.302, P = 0.006), while the levels of the other immune-related proteins measured in the plasma (including the CRP level) were not correlated with cervical dilatation (all variables, r = 0.076–0.189, P > 0.1).
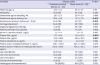
The demographic, clinical, and laboratory characteristics of the study population stratified according to SPTD < 32 weeks of gestation are shown in Table 1. The women who delivered at < 32 weeks of gestation had a significantly higher proportion of cervical insufficiency, more advanced cervical dilatation, and higher rates of antibiotic and tocolytic administration and were less likely to be given vaginal progesterone than those who delivered at ≥ 32 weeks of gestation. The median plasma levels of C3a, C5a, and IL-6, but not of TIMP-1 and MMP-9, were significantly higher in the women with SPTD at < 32 weeks than in those who delivered at ≥ 32 weeks. However, no significant associations were observed between SPTD at < 32 weeks and maternal age, parity, CRP level, positive AF cultures, cerclage placement, and use of corticosteroids.
Table 1
Demographic, clinical, and laboratory characteristics of the study population stratified according to the spontaneous preterm delivery at < 32 weeks
Values are given as the means ± standard deviations or number (%).
Significant findings (P < 0.05) are presented in bold letters.
aData for the histologic evaluation of the placenta were only available in 51 of the 80 women because in 10 cases, delivery took place at another institution and in 19 cases, histologic evaluation of the placenta was not performed because of our institutional policy that only the placentas in cases of preterm delivery are to be sent for histopathologic examination.
![]()
To develop a combined prediction model for SPTD at < 32 weeks, various immune-related proteins in the plasma along with clinical risk factors were included in the multivariate analysis. The variables entered into the multivariate analysis were selected on the basis of a P value of < 0.05 in the univariate analyses, and the continuous factors were included as continuous variables in the model because the linearity assumption was satisfied for these factors. The following factors were entered into the forward selection logistic regression model as predictors related to SPTD at < 32 weeks: cervical dilatation, levels of C3a, C5a, and IL-6 in the plasma, and disease entity. The final variables retained in the prediction model included the plasma IL-6 and C3a levels, and cervical dilatation (Table 2).
Table 2
Regression coefficients, ORs, and 95% CIs of the final non-invasive predictive modela for predicting SPTD at < 32 weeks of gestation

The formula generated to predict SPTD at < 32 weeks was as follows: Y = loge (Z) = −3.826 + 0.312 × (plasma IL-6 [in pg/mL]) + 1.023 × (cervical dilatation [in cm]) + 0.072 × (plasma C3a [in ng/mL]). Z = eY and risk (%) = (Z/[1+Z]) × 100.
OR = odds ratio, CI = confidence interval, SPTD = spontaneous preterm delivery, SE = standard error, IL-6 = interleukin-6.
aFinal model resulting from a forward regression analysis including the following predictive parameters: cervical dilatation, C3a, C5a, and IL-6 in the plasma, and disease entity.
![]()
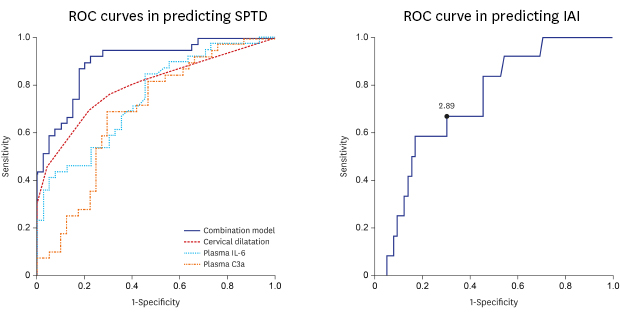
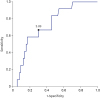
The AUC of this prediction model was 0.901 (95% confidence interval [CI], 0.834–0.968), and the Hosmer-Lemeshow test for this model showed a P value of 0.276, indicating an adequate model fit. The use of the cutoff ≥ 0.38 predicted SPTD at < 32 weeks with a sensitivity of 89.7% (95% CI, 75.8%–97.1%) and a specificity of 80.0% (95% CI, 64.4%–91.0%). The positive and negative likelihood ratios were 4.5 (95% CI, 2.4–8.4) and 0.1 (95% CI, 0.1–0.3), respectively. The AUC for the combined prediction model was significantly greater than that for any single variable included in the predictive model (P < 0.01 for each) (Fig. 1).
 | Fig. 1Receiver-operating characteristic curves in predicting spontaneous preterm delivery at less than 32 weeks by plasma IL-6 and C3a, cervical dilatation, and combined prediction model (including plasma IL-6 and C3a, and cervical dilatation). The area under the curve for plasma IL-6 and C3a, cervical dilatation, and combined prediction model was 0.750, 0.688, 0.793, and 0.901, respectively (P = 0.005 between plasma IL-6 and the combined prediction model, P < 0.001 between plasma C3a and the combined prediction model, P = 0.006 between cervical dilatation and the combined prediction model).IL-6 = interleukin-6.
|
Table 3 displays the demographic, clinical, and laboratory characteristics of the study population according to the presence or absence of intra-amniotic infection. The women with intra-amniotic infection had a significantly higher median plasma IL-6 level and a lower mean gestational age at delivery than those without intra-amniotic infection. However, the median levels of plasma C3a, C5a, MMP-9, TIMP-1, and serum CRP were not significantly different between the two groups. The ROC curve analysis showed that the AUC was 0.734 (95% CI, 0.598–0.870, P = 0.01) and that the best cutoff value for the plasma IL-6 level was 2.89 pg/mL, with a sensitivity of 66.7% and a specificity of 70.1% for predicting the presence of intra-amniotic infection (Fig. 2).
Table 3
Demographic, clinical, and laboratory characteristics of the study population according to the presence or absence of intra-amniotic infection
Values are given as the means ± standard deviations, the median (range), or number (%).
Significant findings (P < 0.05) are presented in bold letters.
aData for the histologic evaluation of the placenta were only available in 51 of the 80 women because in 10 cases, delivery took place at another institution and in 19 cases, histologic evaluation of the placenta was not performed because of our institutional policy that only the placentas in cases of preterm delivery are to be sent for histopathologic examination.
![]()
 | Fig. 2Receiver operating characteristic curve for plasma IL-6 in predicting intra-amniotic infection. Numbers next to solid dots represent plasma IL-6 levels (pg/mL; area under the curve, 0.734; standard error, 0.069; P = 0.010).IL-6 = interleukin-6.
|
Table 4 shows the clinical and laboratory characteristics according to disease entity. The women with premature cervical dilation had significantly higher median plasma C3a and C5a levels, delivered significantly earlier, and had higher risks of SPTD at < 32 weeks of gestation than those with a short cervix. However, the median levels of plasma IL-6, MMP-9, TIMP-1, and serum CRP were not significantly different between the two groups.
Table 4
Demographic, clinical, and laboratory characteristics of the study population according to disease entity
Values are given as the means ± standard deviations or number (%).
Significant findings (P < 0.05) are presented in bold letters.
aData for the histologic evaluation of the placenta were only available in 51 of the 80 women because in 10 cases, delivery took place at another institution and in 19 cases, histologic evaluation of the placenta was not performed because of our institutional policy that only the placentas in cases of preterm delivery are to be sent for histopathologic examination.
![]()
Of the 80 women investigated, 64 (80%) were transferred from a local hospital and the remaining 16 women (20%) were not. There were no differences between the transferred and non-transferred patients in terms of parity; gestational age at sampling and delivery; disease entity; cerclage placement; vaginal progesterone therapy; cervical length on ultrasound; cervical dilatation; prevalence of clinical and histologic chorioamnionitis; and use of antenatal steroid, tocolytic, and antibiotic treatments (data not shown). However, the transferred patients were significantly younger (P = 0.013).
Subgroup analysis was further conducted on the basis of the disease entity to examine the association between the 5 biomarkers, SPTD, and intra-amniotic infection. In the subgroup of patients with premature cervical dilation, the median plasma levels of C3a and IL-6, but not of C5a, MMP-9, and TIMP-1, were significantly higher in the women with SPTD at < 32 weeks than in those who delivered at ≥ 32 weeks. However, none of the proteins whose levels were measured in plasma were associated with the incidence of intra-amniotic infection in the subgroup of patients with premature cervical dilation (Supplementary Tables 1 and 2). Similarly, in the subgroup of women with a short cervix, univariate analyses revealed that only elevated IL-6 plasma level was associated with SPTD at < 32 weeks and that none of the proteins whose levels were measured in plasma were associated with the incidence of intra-amniotic infection (Supplementary Tables 3 and 4).
DISCUSSION
The main findings of this study include: 1) the plasma IL-6, C3a, and C5a levels could be useful non-invasive predictors for SPTD at < 32 weeks in women with premature cervical dilation or a short cervix; 2) using a combination of these biomarkers and conventional clinical factors is more accurate in predicting SPTD than using the markers alone; 3) of the measured plasma proteins, an elevated plasma level of IL-6 only predicted intra-amniotic infection; and 4) the women with premature cervical dilation had significantly higher median plasma levels of C3a and C5a, but not of IL-6, MMP-9, and TIMP-1, as compared to women with a short cervix. To our knowledge, this study was the first to examine the associations of changes in various proteins present in the plasma compartment with intra-amniotic infection in women with premature cervical dilation/short cervix. Similar results regarding the relationship between SPTD, intra-amniotic infection, and plasma pro-inflammatory cytokine levels were also documented for women with preterm labor and intact membranes by our and other groups.13162930
A model based on the plasma IL-6 and C3a levels, and cervical dilatation, as non-invasive parameters, yielded an AUC of 0.901 in predicting SPTD, which indicates a good discriminatory ability. In fact, these factors have been consistently reported to be associated with SPTD in the setting of cervical insufficiency/short cervix 73132 and preterm labor.30 In addition, using this combined model was significantly more accurate in predicting SPTD than using each of these factors alone. These findings are in line with the results of our previous studies on various proteins in the cervicovaginal fluid and AF compartments in women with premature cervical dilation/short cervix2133 and support the notion of multifactorial etiologies for SPTD occurring in premature cervical dilation/short cervix.
Of note, we found that elevated plasma levels of C3a and C5a were associated with an increased chance of SPTD at < 32 weeks. These findings are in agreement with the results of previous studies by Lynch et al.3132 who found a significant relationship between elevated plasma levels of complement activation fragments C3a and Bb in early pregnancy (< 20 weeks) with SPTD. Given the strong connection between the complement system, inflammation, and first-line defense against invading bacteria,34 the findings of our group and Lynch et al.3132 suggest that complement activation in the plasma may have been implicated in the pathophysiology of inflammation-associated preterm birth in which the underlying process was chronic.35 Similarly, in the AF compartment in women with premature cervical dilation/short cervix, we have also demonstrated significant increases in AF C3a and C5a in the occurrence of SPTD.22 In contrast to the results obtained for SPTD, our study demonstrates that the plasma levels of neither C3a nor C5a were associated with intra-amniotic infection, suggesting that it is particularly difficult for the maternal immune system in the plasma to respond to microbes in the amniotic cavity. Many authors have used modeling to identify proteins associated with intra-amniotic infection and SPTD, and generated ROC curves. These curves always appear significant because the data used to generate the ROC curve is derived from the study population based on which it was created. To determine if proteins, which are evaluated with ROC curves, are really predictive of intra-amniotic infection or SPTD, it needs to be tested prospectively in a second population. Therefore, the findings with respect to the relationship of plasma C3a and C5a with the risk of intra-amniotic infection and SPTD should be prospectively validated in a different study population.
In line with previously published in studies on women with preterm,1316 the present study shows that an elevated level of IL-6 in plasma moderately predicted intra-amniotic infection in women with premature cervical dilation/short cervix. IL-6 is a pro-inflammatory mediator that is produced in the choriodecidua compartment in response to microorganisms, which may play a primary role during an ascending intrauterine infection.36 Moreover, the maternal circulation in the choriodecidua space is well established in the 20th week37; thus, IL-6 produced during localized decidual infection gains access to the maternal circulation to induce systemic inflammation. Alternatively, increased IL-6 plasma level in cases of intra-amniotic infection is likely to be due to the possibility that microorganisms directly traverse intact membranes (especially in patients with premature cervical dilation) and induce the production of cytokines (e.g., IL-6) within the amniotic cavity; in turn, these cytokines are released into the circulation. Thus, our finding is natural and supports the hypothesis that a systemic maternal inflammatory response may lead to preterm parturition in women with premature cervical dilation/a short cervix. From a clinical perspective, this observation may be important, as the measurement of the IL-6 level in the plasma may provide information to identify noninvasively the patients who would benefit from antibiotics and cerclage placements. On the other hand, we found that positive AF cultures were not associated with SPTD at < 32 weeks. This finding can be explained by the fact that the conventional culture-based method in the amniotic cavity is substantially less sensitive, considering a report that cultivation techniques for genital mycoplasmas missed 91% of cases with microbial invasion of the amniotic cavity with ureaplasmas demonstrated by molecular microbiology techniques.38 Finally, our findings that the prevalence of intra-amniotic infection in women with premature cervical dilation (16%) or a short cervix (13.3%) was similar to the results of previous studies (for premature cervical dilation, 22% [7/31] vs. 16% [8/50], P = 0.559; for short cervix, 9% [5/57] vs. 13.3% [4/30], P = 0.488).3940
The results of the current study, which were analyzed according to the status of the cervix, have shown that the plasma levels of C3a and C5a were significantly higher in the women with premature cervical dilation than in those with a short cervix. Additionally, we also found that the plasma C3a level was positively correlated with cervical dilatation. Similarly, in the context of animal models of infection-induced preterm labor, previous studies by Gonzalez et al.4142 have reported that complement activation in the serum plays a causative role in cervical remodeling, which results in dilation and effacement of the cervix, leading to preterm delivery in mice. When taken together, these observations suggest that the complement system in the maternal blood may be involved in the mechanism of cervical insufficiency occupying the extreme of a continuum of competence. Future studies are needed to determine whether the complement activation fragments in the plasma can be useful biomarkers for the early diagnosis of premature cervical dilation.
Our study has several limitations. First, the main limitation of the present study is that the cohort was a heterogeneous group with different disease entities (in order to increase the sample size), despite that a short cervix and premature cervical dilation are not the same disease entity. However, it is unlikely that this has altered the main findings, as we adjusted for these confounding variables in the multivariate analysis. Second, the study was of a retrospective nature and was conducted at a single center, thereby limiting the sample size. Third, our prediction models were not validated with test samples, which may limit the generalizability of the study findings. Therefore, our results need further validations from larger prospective studies in other populations. Fourth, not every woman with premature cervical dilation/short cervix who was admitted to our institution was enrolled in the current study because some women did not agree to have amniocentesis, and the decision for completing an amniocentesis was at the discretion of the attending physician. This may cause a concern for a potential selection bias. Fifth, study participants were recruited over a 11-year period to collect a larger number of cases despite improved treatment guidelines for premature cervical dilation/a short cervix in asymptomatic women during this period, which may in turn affect the outcome of interest. Sixth, we did not have information about vaginal culture tests because they were not covered by medical insurance in Korea. Given the report that showed that vaginal Ureaplasma parvum colonization in the first trimester increases the risk for SPTD,43 combination with vaginal culture results might improve the discriminating power for our predictive model. Seventh, we did not have information about prior medications such as progesterone, antibiotic, or tocolytic therapy before the admission of transferred patients, which might have affected the analysis results. The major strength of the present study is that it is, to our knowledge, the first study to examine the associations of changes in various proteins present in the plasma compartment with intra-amniotic infection in women with premature cervical dilation/short cervix.
In conclusion, in women with premature cervical dilation or a short cervix, plasma IL-6, C3a, and C5a levels could be useful non-invasive predictors of SPTD at < 32 weeks; a combination of these biomarkers and conventional clinical factors may clearly improve predictability of SPTD, as compared to the markers alone. Of the measured plasma proteins, an elevated plasma level of IL-6 only predicted intra-amniotic infection. Further large-scale prospective studies are required to determine whether our prediction model or plasma IL-6 will gain an important role in patient selection for a cervical cerclage placement.
 XML Download
XML Download