

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Systemic lupus erythematosus (herein, lupus) is a complex, chronic autoimmune inflammatory disease with many clinical and immunologic manifestations. It occurs disproportionately among women and African Americans.12) The musculoskeletal system is affected severely in patients with lupus, causing arthralgia and arthritis in as many as 95% of patients.345)
Arthritic changes in patients with lupus are different from those in patients with inflammatory arthropathies. These arthritic changes may be related closely to vasculitic changes that also occur with lupus.67) In some series, 4%–30% of patients with lupus develop osteonecrosis, with the femoral head being the most common site of involvement.89) Lupus is often treated with glucocorticoids, which further increase the risk of osteonecrosis.101112)
Lupus treatment has improved, and life expectancy for some patients with lupus has improved;71314) however, the effects of lupus still cause major financial and societal burdens.15) Total joint arthroplasty is an excellent option for patients whose joints have been damaged by lupus-related arthritis. The numbers of total hip arthroplasties (THAs) and total knee arthroplasties (TKAs) being performed for patients with lupus are increasing.16) It is important to characterize the perioperative complications associated with lupus to optimize care and counsel patients about perioperative risks.
The aim of this study was to compare patients with and without lupus who underwent THA or TKA in terms of their characteristics and acute inpatient perioperative complications. We hypothesized that patients with lupus would have higher rates of major complications (including death) and minor complications compared with those of patients without lupus. We report on the risk of acute perioperative inpatient complications after THA or TKA in patients with lupus versus patients without lupus.
METHODS
We searched the National Inpatient Sample (NIS) database for patients who underwent primary THA or TKA from 2000 through 2009. The NIS database includes discharge information from a 20% stratified sample of U.S. hospitals and patient information for all payers. The sampling method reportedly captures 97% of U.S. hospital discharges.11) Discharge weights were used to scale the NIS data to represent the general US population. Our institutional review board deemed this study exempt from approval.
Inclusion and Exclusion Criteria
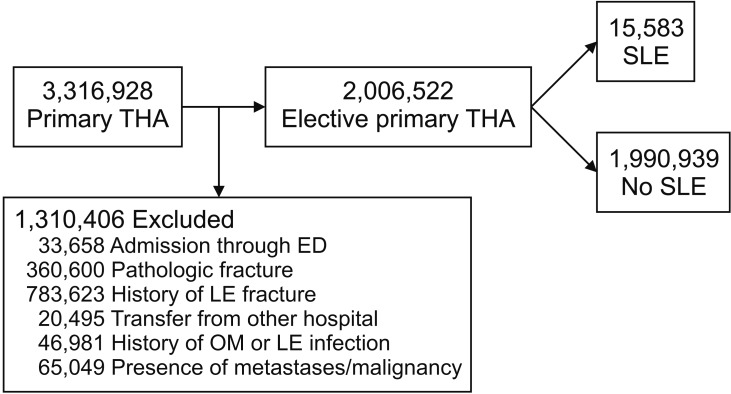
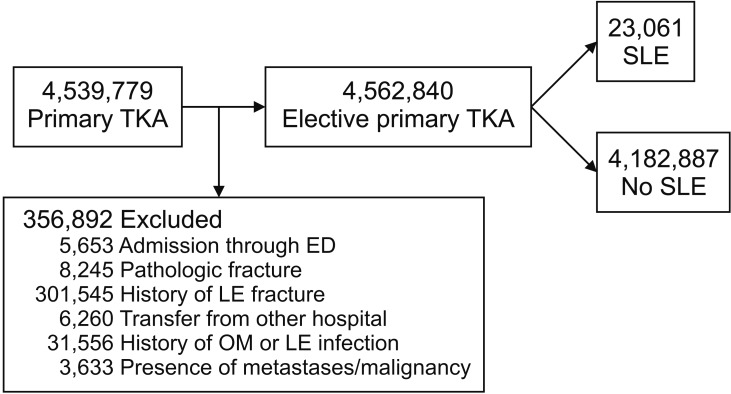
All patients with an International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)17) procedure code for primary THA (code 81.51 or 81.52) or primary TKA (code 81.54) were candidates for inclusion.13) To select for an elective primary arthroplasty population, we excluded patients who had a hip or lower extremity fracture; were admitted through the emergency department; were transferred from another hospital; or had acute or chronic osteomyelitis, malignancy, or history of pathologic fracture. Patients were assigned to one of two subgroups: those with lupus (ICD-9-CM code 710.0), or those without lupus.
Of the 3,316,928 patients who underwent THA, 1,310,406 were excluded (Fig. 1). The remaining 2,006,522 patients formed the THA study group. Of this group, 0.78% (n = 15,583) were diagnosed with lupus. Of the 4,562,840 patients who underwent TKA, 356,892 were excluded (Fig. 2). The remaining 4,205,948 patients formed the TKA study group. Of this group, 0.055% (n = 23,061) were diagnosed as having lupus.
Patient Characteristics and Complications
Using the National Inpatient Survey database, we collected data on patient age, sex, race, and comorbidities (Table 1). Race was categorized as black, white, other (Hispanic, Asian, or Native American), or missing. Comorbidities were classified according to the Elixhauser coding schematic described by Quan et al.18) Duration of hospitalization and total charges were evaluated as continuous variables. We searched the database for major complications (acute renal failure, death, myocardial infarction, pneumonia, pulmonary embolism, and stroke) and minor complications (deep vein thrombosis, hip dislocation, general complications, hematoma, seroma, and wound infection) by ICD-9-CM code. Complications in the National Inpatient Survey database are acute perioperative complications that occur during the same admission as the surgery.
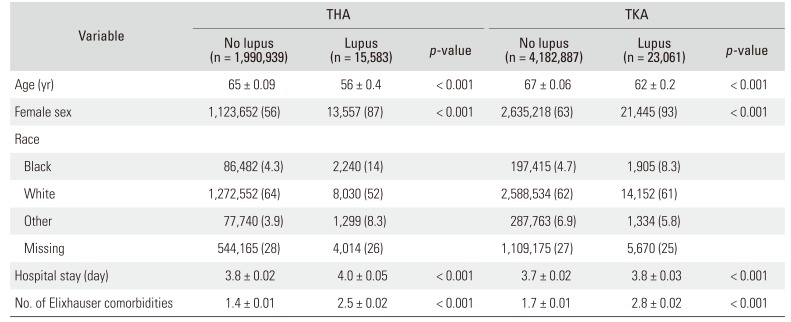
Table 1
Characteristics of Patients Who Underwent Elective Primary THA or TKA by Systemic Lupus Erythematosus Status, National Inpatient Sample, 2000–2009
![]()
Statistical Analysis
Descriptive statistics with standard errors for continuous variables were used for analyzing complications, patient characteristics, hospital charges, and duration of hospitalization. Student t-tests were used for continuous variables, and chi-square tests were used for categorical variables. Significance was set at p < 0.01. Univariate and multivariate logistic regression models were constructed to assess the association of lupus with major and minor perioperative complications. Associations between major Elixhauser comorbidities (i.e., cardiac arrhythmia, chronic pulmonary disease, congestive heart failure, liver disease, obesity, excess weight loss, and peripheral vascular disease) and death and complications in patients with or without lupus were assessed as multivariate odds ratios (ORs) with 95% confidence intervals (CIs). Statistical analysis was performed using Stata ver. 10 (StataCorp., College Station, TX, USA).
Go to : 
RESULTS
Total Hip Arthroplasty
Among patients who underwent elective primary THA, those with lupus were younger (mean age, 56 ± 0.4 vs. 65 ± 0.09 years; p < 0.001), were more likely to be women (87% vs. 56%, p < 0.001), had longer hospital stays (mean, 4.0 ± 0.02 vs. 3.8 ± 0.03 days; p < 0.001), and had more comorbidities (mean, 2.5 ± 0.02 vs. 1.4 ± 0.01; p < 0.001) than those without lupus (p < 0.001) (Table 1). Lupus was independently associated with major complications (OR, 1.4; 95% CI, 1.1 to 1.7) and minor complications (OR, 1.2; 95% CI, 1.0 to 1.5) (Table 2). Deep vein thrombosis, general complications, and pneumonia were associated with lupus on univariate analysis and independently on multivariate analysis (Table 2).
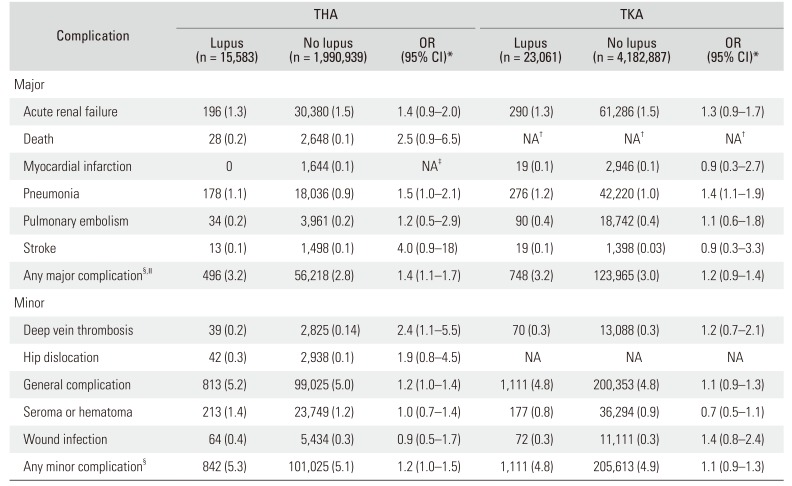
Table 2
In-Hospital Complications after Elective Primary THA or TKA by Systemic Lupus Erythematosus Status, National Inpatient Sample, 2000–2009
Values are presented as number (%).
THA: total hip arthroplasty, TKA: total knee arthroplasty, OR: odds ratio, CI: confidence interval, NA: not applicable.
*From multivariate analysis using patient age, sex, and number of Elixhauser comorbidities as covariates. †The National Inpatient Sample agreement prohibits reporting on variables with cell sizes ≤10. ‡Insufficient patient number to generate OR for THA group. §Patients with more than one complication are counted only once in the aggregate complication categories. ∥Includes death in pooled analysis for TKA group.
![]()
Total Knee Arthroplasty
Among patients who underwent elective primary TKA, those with lupus were younger (mean, 62 ± 0.2 vs. 67 ± 0.06 years), were more likely to be women (93% vs. 64%), had longer hospital stays (mean, 3.8 ± 0.03 vs. 3.7 ± 0.02 days), and had more comorbidities (mean, 2.8 ± 0.02 vs. 1.7 ± 0.01) than those without lupus (all p < 0.001) (Table 1). Lupus was not associated with increased odds of major complications (OR, 1.2; 95% CI, 0.9 to 1.4) or minor complications (OR, 1.1; 95% CI, 0.9 to 1.3) (Table 2). Patients with lupus were no more likely than those without lupus to have major or minor perioperative complications according to a pooled analysis (Table 2).
Go to :
DISCUSSION
Using 2000–2009 data from the NIS, we found associations between lupus and major and minor perioperative complications associated with elective primary THA, but not TKA. Patients with lupus who underwent THA or TKA were younger, were more likely to be women, had longer hospitalizations, and had more comorbidities than patients without lupus. As the life expectancy of patients with lupus continues to improve, their rates of osteonecrosis and joint replacement are likely to increase as well.121920)
Studies that have investigated the association between lupus and outcomes after THA have produced conflicting results, suggesting that lupus is and is not associated with negative outcomes. However, these studies were retrospective and used data from single centers or small patient cohorts.1621) The patient characteristics reported by Shah et al.21) and Roberts et al.16) have similarities to the current findings, including female predominance and more comorbidities in patients with lupus.
In the current study, no association was found between lupus and major or minor perioperative complications after elective primary TKA. Patients with lupus were younger than those without lupus in both the THA and TKA groups. However, the age difference between the TKA groups (with vs. without lupus) was not as great as that between the THA groups. In patients with lupus, the pathophysiology of knee arthritis may be slightly different from that of hip arthritis. There may be more osteonecrosis because lupus has a vasculitic component, and perfusion to the periarticular regions in the hip is more tenuous than that in the knee.67) The rate and nature of the development of severe hip pain necessitating THA may be an indirect way of identifying the severity of lupus.
Another possible explanation for differences in outcomes after THA versus TKA is the difference in blood loss typically experienced during these procedures. THA frequently involves more blood loss than TKA and is associated with a 2–3 times higher transfusion rate.2223) In this and other studies, patients with lupus who undergo arthroplasty have more comorbidities than those without lupus, and blood loss may predispose these patients to perioperative complications.1621)
The limitations of our study are related to the use of the NIS database, which records administrative data for the duration of the initial hospitalization only. Administrative databases have various levels of reliability depending on the comorbidity.24) Long-term outcomes after discharge, which are an important metric for arthroplasty, cannot be evaluated using the NIS. Another limitation is the completeness of the NIS data. The information coded in the NIS is reasonably accurate, with a specificity of more than 92%, but it may be incomplete.25) The NIS has the major advantage of being the largest administrative database available that includes all payers. For patient subsets, such as those with lupus, in which there are few cases at a single institution or even multiple institutions, the NIS database is an excellent tool for providing a large sample size to determine incidence of relatively rare outcomes, such as inpatient death.
Compared with those without lupus, patients with lupus are at substantially higher risk of acute perioperative inpatient complications after THA but not after TKA. Elective THA should be approached with caution after careful consideration of comorbidities and risk factors.
Go to :
 XML Download
XML Download