

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Congenital clubfoot, or congenital talipes equinovarus (CTEV), is one of the most common congenital deformities.1) It most likely represents congenital dysplasia of all musculoskeletal tissues (musculotendinous, ligamentous, osteoarticular, and neurovascular structures) distal to the knee. This conclusion is based on multiple investigators' observations of a myriad of different abnormal anatomic findings and on the functional outcome of patients who were believed to have received optimal non-operative or operative treatment but nevertheless subsequently always had some degree of impairment.2) Congenital clubfoot is a complex three-dimensional deformity consisting of four components: cavus, adductus, varus, and equinus.
The incidence of congenital clubfoot is approximately 1.2 per 1,000 live births.3) If a clubfoot is allowed to remain deformed, many other late adaptive changes occur in the bones. These changes depend on the severity of soft-tissue contractures and the effects of walking. In untreated adults, some joints may spontaneously fuse or degenerative changes secondary to the contractures may develop.
On the basis of a proper understanding of the pathoanatomy from stillborn fetuses with clubfeet and of functional anatomy from radiography of normal feet and of clubfeet, Ignacio Ponseti developed and refined a uniform treatment for clubfeet in the late 1940s.4) Although Ponseti's clubfoot treatment has been around for many years, it is only in the recent past that his method has been given due consideration with a review of the long-term results of patients treated by him.5) The standard regimen of the Ponseti casting technique involves weekly change of cast after an initial period of manipulation. However, more recently, this arbitrary interval between two consecutive casts has been called into question. Studies have shown that the accelerated Ponseti protocol has as similar safety and efficacy as the standard protocol. In the accelerated Ponseti technique, casting is done after five days, twice weekly or thrice weekly.6)
An earlier study by Elgohary and Abulsaad7) showed that the accelerated Ponseti technique significantly reduces the correction time without affecting the final results while being as safe and effective as the traditional Ponseti, but they had excluded patients with a pretreatment Pirani score of less than 4. A decrease in the overall duration of treatment could offer multiple potential benefits leading to better compliance. The aim of our study was to compare the results of the standard Ponseti regimen to those of the accelerated Ponseti regimen in our population cohort.
METHODS
This study is a prospective, single-blind, randomized controlled study conducted in our hospital between May 2015 and December 2016. A minimum 1-year follow-up was completed by December 2017. After obtaining permission from the college ethical committee, we enrolled a total of 100 patients for the study and followed up for a minimum of 1 year. Written informed consent was obtained from the parents or guardians of the children. Randomization was done at the patient level with both feet being treated by using the same method in bilateral cases and an opaque sealed envelope method was used. Exclusion criteria were as follows: age more than 6 months, neurogenic or syndromic CTEV, and previously operated or relapsed CTEV.
All patients were treated in our clubfoot clinic and a detailed history was sought from attendants, with particular reference to the age, sex, exposure of the mother to radiation or drugs during pregnancy, type of delivery, place of delivery, birth order, birth asphyxia, family history, other deformities or diseases, and any previous intervention. Initial Pirani8) and Dimeglio9) scoring was done. Radiographs of the foot were taken (anteroposterior view and lateral view in stress dorsiflexion) to calculate the talocalcaneal angle, talus-first metatarsal angle, and tibiocalcaneal angle.10)
Steps were the same in both the standard and accelerated Ponseti techniques111213) except for the duration of cast immobilization. The cast was changed twice weekly in the accelerated group and once weekly in the standard group. The two phases in the management were as follows: (1) treatment phase: consisted of weekly gentle manipulation and casting in the standard group and twice weekly in the accelerated group. Manipulation was done for 1 minute in each group. (2) Maintenance phase: consisted of bracing with a foot abduction orthosis after removal of the final cast.
All the deformities of clubfoot were corrected simultaneously except the equinus deformity, which was corrected in the final cast. The final cast was applied for three weeks with the foot in more than 15° of dorsiflexion and 70° of abduction, if tendoachilles tenotomy had been performed, or for 2 weeks otherwise. The radiographs of the foot were taken to calculate talocalcaneal angle, talus-first metatarsal angle, and tibiocalcaneal angle after the final cast was removed.
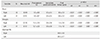
The foot abduction brace was used thereafter for 23 hours a day for 3 months and then during night time and nap time. The first follow-up was at 1 week to check for compliance of bracing, then monthly till 3 months and then every 3 months till final assessment at 1 year. At the end of 12-month follow-up, the Pirani and Dimeglio scores were checked along with the modified functional rating system (FRS) score (Table 1).1415) Results were labeled as excellent, good, fair, and poor on the basis of the modified FRS score.
Statistical Methods
Data analysis was performed by using IBM SPSS ver. 25.0 (IBM Corp., Armonk, NY, USA). Metric data are described as mean and median; nonmetric or categorical data are described as frequency and frequency percentage. Intergroup comparison of metric variables was done by the Student t-test and that of nonmetric variables was done by chi-square test. Furthermore, the intragroup variance was measured by paired t-test and repeated measures analysis of variance was done by F-test. All the inferences were drawn at 0.05 level of significance.
RESULTS
A total of 100 patients were included in the study (158 feet). Of those, 58 patients had bilateral involvement, 23 had right-side involvement and 19 had left-side involvement. In the standard group, 31 (62%) had bilateral involvement, nine (18%) had right-side involvement, and 10 (20%) had left-side involvement; in the accelerated group, 27 (54%) had bilateral involvement, 14 (28%) had right-side involvement, and nine (18%) had left-side involvement. The mean age in the standard group was 29.2 days (range, 2 to 165 days) and that in the accelerated group was 18.2 days (range, 1 to 175 days). Most of our patients were male: 36 in the standard group and 34 in the accelerated group. Family history of CTEV was present in 9% of total cases.
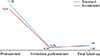
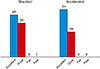
The average pretreatment, immediate posttreatment, and final follow-up Pirani and Dimeglio scores are given in Figs. 1 and 2. There was no statistically significant difference in the number of casts needed for full correction between the standard group (6.3 ± 1.2) and the accelerated group (6.1 ± 1.4; p = 0.45). The average duration of casting needed for correction was 58.2 ± 8.3 days (range, 42 to 77 days) in the standard group and 39.5 ± 5.2 days (range, 32 to 56 days) in the accelerated group (p < 0.001). In the standard group, 70 of 81 clubfeet (86.42%) needed a percutaneous tendoachilles tenotomy while in the accelerated group, 65 of 77 clubfeet (84.41%) needed one. The mean age at tenotomy was 41.02 days in the standard group and 18.18 days in the accelerated group.
The anteroposterior talocalcaneal angle increased from 17.22° ± 6.3° pretreatment to 33.93° ± 8.9° immediate posttreatment (p < 0.05) in the standard group and from 17.4° ± 6.5° to 36.54° ± 8.6° (p < 0.05) in the accelerated group. The mean lateral talocalcaneal angle increased from 18.18° ± 5.7° to 31.01° ± 8.7° (p < 0.05) in the standard group and from 18.66° ±6.8° to 34.35° ± 9.8° (p < 0.05) in the accelerated group. The mean talus-first metatarsal angle changed from 60.33° ± 20.5° to −23.37° ± 9.2° (p < 0.05) in the standard group and from 56.79 ± 19.10 to −23.97 ± 10.90 (p < 0.05) in the accelerated group. The mean tibiocalcaneal angle decreased from 108.95 ± 20.30 to 79.74 ± 10.20 (p < 0.05) in the standard group and from 102 ± 15.50 to 80.4 ± 12.60 (p < 0.05) in the accelerated group. There was no statistically significant difference between the two groups in immediate posttreatment anteroposterior talocalcaneal angle (p = 0.07), lateral talocalcaneal angle (p = 0.06), talus-first metatarsal angle (p = 0.97), and tibiocalcaneal angle (p = 0.95).
Final outcome was assessed by using the modified FRS and categorized into excellent, good, fair, and poor. The mean FRS was 83.81 ± 6.8 in the standard group and 85 ± 6.3 in the accelerated group (p = 0.24). In the standard group, excellent and good results were obtained in 55.55% and 44.45% (45 and 36 out of 71) feet, respectively; and in the accelerated group in 66.23% and 33.77% (51 and 26 out of 77) feet, respectively. There were no patients with fair or poor results (Fig. 3).
Table 2 lists the complications that we encountered during the treatment of clubfeet and the management of these complications. Only equinus deformity recurred among our patients. In the standard group, it recurred in two patients (three feet); in the accelerated group, in one patient (two feet). All of these patients were managed by percutaneous heel cord tenotomy and casting. All of these patients had not had an initial tendoachilles tenotomy done. We also did an intragroup comparison (post-hoc analysis) of treatment scores over the study period in each group, the results of which are presented in Tables 3 and 4: there were statistically significant differences in Pirani and Dimeglio scores between pretreatment, immediate posttreatment, and final follow-up. Table 5 summarizes the results of this study.
DISCUSSION
At present, the Ponseti method is the most commonly used modality for management of CTEV.16) The traditional Ponseti technique of weekly manipulation and casting is inexpensive, has a relatively short learning curve, and has yielded excellent results in both in short- and long-term studies.17) Although Giesberts et al.18) have published a review article showing that accelerated protocols have a similar efficacy and safety profile as the traditional protocols, no ideal casting interval has been suggested. Our aim was to establish the effectiveness of a twice-weekly accelerated protocol vis-à-vis the standard protocol in our population cohort.
The overall male to female ratio in our study was 2.3 (2.57 in the standard group and 2.12 in the accelerated group). Although many studies have demonstrated this sexual dimorphism, the exact cause is still not known. A polygenic threshold model with Carter effect has been proposed as the likely mechanism.15) While in our study 9% of the patients had a positive family history, this is much less than 22% and 25% reported by Terrazas-Lafargue and Morcuende19) and Dobbs and Gurnett,20) respectively. Bilateral involvement (58%) was more common in our study than that in the study by Elshenawy et al.21) The initial Pirani score was 4.67 in the standard group and 4.35 in the accelerated group, lower than that in studies by Elgohary and Abulsaad7) and Harnett et al,22) reflecting a less severe initial deformity. The immediate posttreatment score was 0.34 in the standard group and 0.35 in the accelerated group; Elgohary and Abulsaad7) reported immediate posttreatment scores of 0.49 and 0.52. The average decrease in the Pirani score in our study was 4.32 in the standard group and 4 in the accelerated group, whereas it was 4 and 4.5, respectively, in the study by Harnett et al.22) The Pirani score at final follow-up was 0.56 in the standard group and 0.50 in the accelerated group, whereas Elgohary and Abulsaad7) reported a score of 0.49 and 0.52 in respective group. The initial Dimeglio score was 11.75 in the standard group and 10.51 in the accelerated group, the mean immediate posttreatment score was 0.79 in both groups, and at final follow-up, it was 1.25 and 1.36, respectively.
The mean number of casts required was 6.32 in the standard group and 6.14 in the accelerated group. In the study by Elgohary and Abulsaad,7) the number was 4.88 and 5.16, respectively, and in the study by Harnett et al,22) 4 and 4, respectively. In our study, percutaneous heel cord tenotomy was done in 86.42% in the standard group and in 84.41% in the accelerated group. The rates of tendoachilles tenotomy have been variably reported as <50% to 100% in various studies.2324) In our study, the average time spent in cast was 58.52 days in the standard group and 39.38 days in the accelerated group. However, when we excluded the last cast, which was of variable duration depending on whether a tenotomy had been done or not, the average time spent in cast (before correction of equinus) was 41.02 days in the standard group and 18.18 days in the accelerated group (p < 0.001). Elgohary and Abulsaad7) reported the average time spent in cast before correction of equinus was 33.36 days in the standard group and 18.13 days in the accelerated group, while Xu25) reported 35.35 days and 20.61 days, respectively.
In our study, five of the total 158 feet had a recurrence: three feet (3.7%, two patients) in the standard group and two feet (2.6%, one patient) in the accelerated group. While Harnett et al.22) reported no recurrences at about 6 months' follow-up, Elgohary and Abulsaad7) reported a recurrence of 14.7% and 15.6 % in the two groups at a minimum 1-year follow-up (range, 12 to 48 months). The recurrence was in the form of equinus deformity in these patients and all of them did not have an initial heel cord tenotomy. The cause of recurrence in our study may be attributed to not performing an initial tenotomy. We encountered one tibial fracture in the first patient in the accelerated group at the time of brace application. Although the cause of this fracture was unidentified, the fracture healed after two more weeks of cast immobilization. Gerlach et al.26) in a 2009 study, reported two iatrogenic fractures of tibia in patients with clubfoot managed with the Ponseti technique. In one case, the distal tibial fracture was incidentally seen after clubfoot correction; in the other case, the tibial fracture was seen 24 hours after the brace application.
The Ponseti method continues to be the best approach for correction of typical congenital clubfeet. But, changing casts twice weekly greatly reduces the time patients spend in cast immobilization. In addition, in developing countries where time to clinics necessitates time away from home, work, and family, the adoption of accelerated technique can reduce costs for families and help to improve patient compliance. However, the final outcome did not show any significant difference between the two methods. The only problem we could find with the accelerated Ponseti method was that we had to dedicate two days to clubfoot clinic rather than a single day. The limitation of the study was the relatively short follow-up; a longer follow-up may reveal other significant differences between the two methods.





 XML Download
XML Download