

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Injury is a major cause of disability and death among children of all ages worldwide.12 In 2018, 24,097 incidents of child safety accidents were reported to the Consumer Injury Surveillance System (CISS) of the Korea Consumer Agency (KCA).3 A recent study using nationwide sampling data reported that the incidence of pediatric injury increased over the past 10 years despite a declining pediatric population in Korea. They also reported that the proportion of indoor playground-related injuries increased rapidly according to the increased number of indoor playgrounds. This increasing trend in pediatric injuries may be partially explained by the increasing availability of indoor playgrounds.4
A kids café is a type of indoor playground that has themed play facilities and food and beverage facilities. A kids café allows infants or children to safely have fun in various playrooms and allows their parents or guardians to read books, socialize with their friends, drink tea or comfortably take a rest.5 The number of kids cafés, which have been very popular in Korea for the past five or six years, has increased dramatically from 1,493 in 2015 to 2,626 as of the end of October 2018.6 As the number of kids cafés has increased, the number of children injured in kids cafés has also increased every year, raising concerns about children's safety. According to the KCA's report, 7,603 safety accident reports involving children under 14 years of age in the leisure, culture and play facilities were received in the CISS for the past five years (2014 to 2018). Among them, the most frequent site of accidents was the park, which accounted for 29.9% (1,234 cases), and the second most frequent site of accidents was kids cafés (26.2%; 1,082 cases).3 Kids café-related injuries in children increased approximately five fold in 2018 compared to 230 cases in 2015.7
Pediatric injury in kids cafés is increasing, and it is very important to collect objective data on them to assess the current situation and establish effective preventive measures based on these data. However, existing data collected in Korea have limitations with regard to identifying the clinical information, exact mechanism of injuries and environment associated with injuries in kids cafés. Therefore, in this study, we analyzed the characteristics of pediatric injuries in kids cafés and the risk factors for significant injuries that may require hospitalization or surgery based on information from the emergency medical centers visited by children who were injured to a certain degree in kids cafés.
METHODS
Study design and patients
This cross-sectional study was performed using data from the Emergency Department (ED)-based Injury In-depth Surveillance (EDIIS) registry in Korea. All patients under 18 years of age who were registered in the EDIIS database as having a pediatric injury from a kids café between January 2011 and December 2016 were included. Cases of pediatric injuries in a kids café were first identified by extracting the word “kids café”, words that are similar to “kids café” in Korean and the word “kids” from the variables containing free texts about the injury narratives and places, and one researcher then reviewed the injury narratives. After a review of the injury narratives, we excluded cases that were not related to kids cafés.
EDIIS registry
In 2006, the EDIIS was established by the Korea Centers for Disease Control and Prevention with five hospitals. It was developed to collect in-depth data on injury mechanisms and causes and to provide useful information for establishing strategies for injury prevention. The number of participating hospitals has increased to 20 since 2010, and now data on injured patients are being collected in 23 EDs in Korea. The EDIIS database has 246 variables, including patient demographics, injury-related data, prehospital data, clinical variables, diagnosis and medical treatment in the ED, ED disposition, and clinical outcomes after hospitalization.8
Variables and measurements
Information on the patient's age and sex, anatomical site of the injury, injury types, mechanism of injury, injury-inducing factors, ED disposition, number of days hospitalized and surgery was collected. The patients were divided into three age groups based on human development and growth according to the medical subject heading definition as follows: infant (0–1 years), preschool child (2–5 years), and child (6–12 years). The injured anatomical sites were categorized into head, face, oral cavity, neck, torso (including the thorax, abdomen, back, pelvis and genitals), upper extremity (including the shoulders, upper arms, elbows, forearms, wrists and hands), lower extremity (hips, thighs, knees, lower legs, ankles and feet), multiple (a combination of one or more of the above anatomical sites) and unspecified according to the International Classification of Disease 10th Revision (ICD-10) code and the review of the injury narratives. The injury types were divided into concussion, fracture, dislocation/subluxation, sprain/strain, laceration, superficial and unspecified according to the ICD-10 code. The mechanisms of injury were classified into slip, fall, collision with structures, contact with human, overuse and others. Injury-inducing factors were identified by reviewing the variables containing free texts about the injury narratives and inducing factors. Injury-inducing factors were divided into play equipment (trampoline, ride, slide, small toy including block, jungle gym, sand and seed, ball pool, zip-line, and rock climbing equipment), human, floor, furniture, wall and column, doors, stairs, and others/unspecified.
Main outcomes
The primary outcome of this study was risk factors for significant injuries in kids cafés. Significant injury was defined as injury requiring hospitalization or surgical treatment. The secondary outcome of this study was clinical characteristics of kids café-related injuries in Korea.
Statistical analysis
All statistical analyses were performed using STATA version 14.2 (StataCorp LP, College Station, TX, USA). Continuous variables were presented as medians with interquartile ranges (IQRs), and categorical variables were presented as the frequencies with the proportions. The odds ratio (OR) with 95% confidence interval (CI) was calculated using a multivariable logistic regression model to assess the relevant factors for significant kids café-related injury. The OR was adjusted for patient age, sex, anatomical site and mechanism of injury. The level of statistical significance was defined as a P value less than 0.05.
RESULTS
Demographics and clinical characteristics of kids café-related injuries in Korea
From 2011 to 2016, 1,537,617 injured patients were registered in the EDIIS registry. After a review of the injury narratives and places, 891 patients were included in the final analysis.
Table 1 shows the basic characteristics of kids café-related injuries by age group. The majority of pediatric injuries in kids cafés occurred in preschool children, and their median age was 3 years (IQR, 2–5). Males were predominant in all age groups. The most common anatomical site of the injury was the lower extremity (28.2%), followed by the upper extremity (24.7%), face (18.3%), head (10.8%), and oral cavity (10.0%), although face, oral cavity and head injuries were more common than upper extremity injuries in infants. The most common type of injury was superficial injury (27.2%), followed by fracture (23.3%) and laceration (22.0%); however, laceration was the most common type of injury in infants. The most common mechanism of injury was slip (27.1%), followed by fall (21.8%) and collision with structures (19.8%). Notably, however, fall was the most common mechanism of injury in children older than 6 years. After ED treatment, 46 patients (5.2%) were hospitalized, and 39 (4.4%) underwent surgery. Children older than 6 years were hospitalized more often, and preschool children had surgery more often than the other age groups. Among the hospitalized patients, the median hospital stay was two days (Table 1).
Table 1
Characteristics of kids café injuries by age group

Data are presented as median (interquartile range) or number (%).
aMultiple wound was defined as a combination of one or more of the anatomical sites.
![]()
There were 57 (6.4%) significant injuries that required admission or surgery. Table 2 shows the characteristics of significant kids café-related injuries compared to those of nonsignificant injuries. Upper extremity injury (73.3% vs. 21.3%; P < 0.001) and fracture (82.5% vs. 19.3%; P < 0.001) were more commonly significant injuries than nonsignificant injuries. Injury caused by slip (31.6% vs. 26.7%; P = 0.004) and fall (40.4% vs. 20.5%; P = 0.004) were significantly higher among significant injuries than among nonsignificant injuries (Table 2).
Table 2
Characteristics of kids café injury by severity
Data are presented as number (%).
aSignificant injury was defined as an injury requiring hospitalization or surgery; bMultiple wound was defined as a combination of one or more of the anatomic sites.
![]()
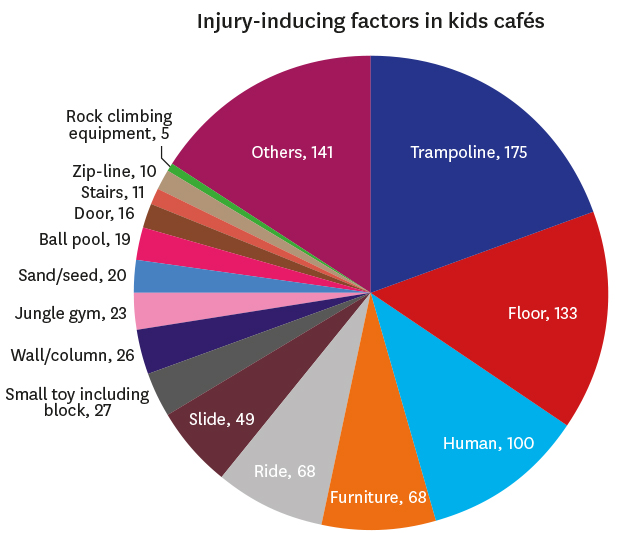
Among the injury-inducing factors, trampoline was the most common (19.6%). The results of the multivariable logistic regression analysis assessing significant injury-inducing risk factors are summarized in Table 3. When the OR was adjusted for patient age, sex, anatomical site and mechanism of injury, rock climbing equipment was the sole risk factor associated with significant kids café-related injuries (adjusted ORs, 14.94; 95% CI, 1.51–147.72) (Table 3).
Table 3
ORs for injury-inducing factors associated with significant injuries in kids cafés
OR = odds ratio, CI = confidence interval.
aSignificant injury was defined as injuries requiring hospitalization or surgery; bAdjusted for age, sex, injury mechanism and anatomical sites of injury.
![]()
DISCUSSION
A kids café is a specialized indoor playground that combines a playground for young children and a café for their caregivers and is especially popular in Korea.5 In recent years, child safety accidents have frequently occurred in kids cafés, becoming a social issue.3 This study is the first to report about kids café-related injuries. As the popularity of kids cafés rises in Korea, it is essential for healthcare providers and families with children to be aware of the risk factors for serious injuries in a kids café. In this study, we assessed the characteristics of kids café-related injuries in Korea and analyzed the risk factors associated with significant kids café-related injuries using a multicenter injury surveillance database. In this study, although most of the kids café-related injuries were minor, 5.2% of the children were hospitalized, and 4.4% had surgery. Upper extremity injuries, fractures, and the mechanisms of injuries (slip or fall) were associated with significant injury. Among the kids café facilities and equipment, significant injuries were most commonly caused by trampoline. Multivariable logistic regression analysis indicated that the rock climbing equipment was the only risk factor for significant kids café-related injuries. This result will be helpful in establishing preventive measures such as safety guidelines or educational programs for the safety of children in kids cafés.
Traditionally, the playground is the representative space where outside play activities occur during childhood. Over the past several years, indoor recreational facilities such as trampoline parks have increased in number and popularity in Western countries. Because of the increased number of indoor trampoline parks, they are increasing as a source of injuries among children.910 In Korea, large-sized indoor trampoline parks are not popular because of space limitations. Instead, another type of indoor playground called a “kids café” has emerged recently.11 Accordingly, the proportions of indoor playground- and trampoline-related injuries have recently increased rapidly in Korea.4
Kids café-related injuries are similar to playground-related injury, but there are also differences. Previous studies on playground-related injury in the US showed that playground-related injuries are common between the ages of five and eight years. The most common injury mechanism was fall, and the most common site was the upper extremity. Hospitalization occurred in 3%–9% of patients, the majority of whom had fractures.121314 A recent study about playground-related injuries in Korea showed that fall was the most common injury mechanism and that the head and neck were the most common injured anatomical location. Hospitalization occurred in approximately 8.25% of patients, most of whom had upper extremity injuries and fractures. Only 1.26% of patients received emergency operations. Compared with these studies on playground-related injury, our study showed that kids café-related injuries occurred in children younger than 5 years old. The ages of children visiting kids cafés ranges from infants to elementary school students. A kids café is an indoor playground where children of all ages usually play together; therefore, it is easy to injure young infants and toddlers who are not able to properly follow their bodies when they play with older children in a narrow place. In addition, the hospitalization rate was lower (5.2%), but the proportion of patients who underwent surgery (4.8%) was higher than that of playground-related injuries. In other words, minor injuries were more common, but serious injuries requiring surgery were also more common. Most kids cafés have a trampoline. Upper extremity, head and neck injuries often result from falls off a trampoline.15161718 Our study also showed that significant injuries requiring hospitalization or surgery were most commonly caused by trampoline. Therefore, the higher surgical rate is probably due to the kids café's trampoline. Regardless of age, the most common sites of injury were the lower extremities (28.2%) and upper extremities (24.7%), but the majority of injuries leading to hospitalization and surgery were upper extremities (73.7%) and fractures (82.5%). Most cases consisted of slip (27.1%), fall (21.8%), and collision (19.8%), which can cause high-energy traumatic events. A kids café is an indoor playground, which is smaller than an outdoor playground and is crowded with children of various ages. For this reason, small children are likely to bump into large children.
There are many kinds of rides and play equipment in kids cafés. In a kids café, children can be injured by a variety of materials, such as play equipment, the floor, other people, and furniture. Among them, rock climbing equipment in a kids café was a significant risk factor for serious injuries requiring hospitalization or surgery. The rock climbing equipment consists of walls with sharp-edged stones protruding from the surface of the wall. Children can climb a rock wall and fall down from a considerable height. In this study, both children (one 4-year-old and one 6-year-old) who were injured by the climbing equipment and admitted to the hospital were injured by a fall from a height. One had surgery, and the other was unknown. Otherwise, children may be injured by hitting the protruding rocks near the climbing walls. Young infants and toddlers who are not yet able to walk well alone and small children can be injured by slipping around the rock wall or by bumping into a larger child around the rock wall and then secondarily into the rock wall. For safe use of the rock climbing equipment in kids cafés, safety devices, protective gear and guardians who assist children while playing are very important. For play equipment that can cause high-energy trauma, such as rock climbing equipment, legal regulations may be needed from the early stage of installation in kids cafés to establish strict safety standards.
This study has several limitations. First, we identified kids café-related injuries by reviewing the variables containing free texts about the injury narratives and places. Therefore, if the registered data were insufficient or incorrect, this study is likely to have selection bias. Second, this study focused on patients who visited EDs in Korea and not all EDs in Korea were included in the EDIIS, although the EDIIS is a multicenter injury registry in Korea. Therefore, the study population in this study may not represent all cases of pediatric injuries in kids cafés. Third, we defined a significant injury as the need for surgery or hospitalization. In terms of the severity of injuries, hospitalization may be limited to representing severity because it can be affected by differences among hospitals. In hospitals that have room to spare, patients may be hospitalized for relatively minor injuries that require short-term follow-up or because the parents request hospitalization. Fourth, this study was based only on the preregistered items in the EDIIS registry because this study is a retrospective cross-sectional study. Therefore, other potentially important factors, such as the presence of caregivers or safety guards and fall height, were not available, and these factors might affect the outcomes as potential confounders. To overcome these limitations, further studies are required.
In conclusion, this study examined the clinical characteristics of kids café-related injuries in Korea and found that rock climbing equipment is especially risky for significant injuries in kids cafés. Our study suggests that further injury prevention strategies are warranted. Strict safety standards should be applied when installing play equipment that can cause high-energy damage, especially rock climbing equipment.
 XML Download
XML Download