

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cardiovascular diseases are the most prevalent cause of mortality and morbidity in diabetic populations associated with chronic endothelial dysfunction [1] characterized by decreased bioavailability of nitric oxide (NO) due both to reduced endothelial nitric oxide synthase (e-NOS) activity and NO inactivation by reactive oxygen species (ROS) produced in excess under oxidative stress conditions associated with diabetes. Consequently, endothelial dysfunction together with obesity, hypertension and dyslipidemia represent major cardiovascular risk factors in diabetes [2].
Physical activity (PA) could be an important therapy in diabetes treatment being able to influence cardiovascular risk factors, improving endothelial functionality and lowering oxidative stress. In fact, it enhance NO production at the endothelial level by promoting blood-flow mediated shear stress [3]. Moreover, regular PA stimulates endogenous antioxidant defense systems improving the cellular redox status [4].
However it is difficult to engage patients in a radical lifestyle change involving a structured PA routine, especially in the case of sedentary subjects. Besides exercise sessions, the overall daily workload should be considered in relation to its influences in lowering cardiovascular risk factors in diabetic patients.
The present study was designed to evaluate the hematochemical, clinical, and biochemical effects of PA measured as recorded amount of activity rather than as scheduled and/or perceived amount of exercise in diabetics. microRNAs expression modulation in circulating angiogenic cells (CACs) was also evaluated as an innovative biomarker of vascular senescence in age-related diseases including diabetes.
METHODS
Participants and study design
This prospective observational study was conducted on nineteen naïve type 2 diabetes mellitus patients not doing any type of structured physical exercise activity (13 males and six females; aged 62±2 years; body mass index, 30±1 kg/m2; glycosylated hemoglobin [HbA1c], 7.6%±0.25%), recruited at the Diabetology Unit of the Italian National Research Center on Aging (INRCA) Hospital of Ancona, Italy. Inclusion criteria were age 50 to 70 and ability to perform at least 30 minutes walking without assistance. Exclusion criteria included physical inhabilities, neurodegenerative diseases and severe cardiovascular events.
The patients were instructed on the benefits of regular PA participating in a counseling activity based on the guidelines of the Italian Standard for Diabetes Mellitus care and American Diabetes Association recommendations and on the use of the portable gravitometer (MyWellness Key; Technogym, Cesena, Italy) used to record daily PA performed for 3 months. Clinical, hematochemical, and biochemical indexes were analyzed at the start and at the end of the study under fasting conditions.
The study was performed in accordance with the Helsinki Declaration of human studies and was approved by the Ethics Committee of INRCA (CER 2016-0614 IN). A written informed consent was obtained by all participants prior their inclusion in the study.
Evaluation of physical activity: MyWellness Key
PA was recorded through MyWellness Key [5], a wearable gravitometer that measures vertical acceleration determining the time and intensity [6]. MyWellness Key quantifies in real time during the day the volume of PA using MOVE units [7] an adimensional index similar to the metabolic equivalent of task for minute (MET-minutes) (2.5 MOVE=1 MET-minutes) [89].
A dose of 500 to 1,000 MET-minutes (equivalent to 1,250 to 2,500 MOVEs) per week, is considered a moderate PA sufficient to produce health benefits [10]. MOVEs can be used to identify different levels of daily PA, in particular: light exercise below 499 MOVEs, moderate exercise from 500 to 749 MOVEs, high intensity exercise from 750 to 999 MOVEs and very high intensity over 1,000 MOVEs [9].
Hematochemical evaluation
Lipid profile (triglycerides, high density lipoprotein cholesterol [HDL-C], low density lipoprotein cholesterol [LDL-C], and total cholesterol) and HbA1c were evaluated.
Clinical evaluation
The clinical parameters considered were systolic and diastolic blood pressure, body composition using dual-energy X-ray absorptiometry technique and endothelial function by using the endothelial-dependent vasodilation of finger arteries measured by peripheral arterial tonometry which permits to evaluate both reactive hyperemia index and augmentation index (AI) [11].
Biochemical evaluation
Paraoxonase-1 (PON-1) paraoxonase and arylesterase activities [12] and oxidized LDL levels by using enzyme-linked immunosorbent assay (ELISA) test (Oxidized LDL ELISA kit; Mercodia, Uppsala, Sweden) were evaluated in plasma. CACs isolation was performed from peripheral blood and microRNA-21, -126, -130a, and -146a were evaluated [13]. Expression levels are reported as relative expression according to the 2-ΔCt method and cell microRNA-39 was used as spike in.
Peripheral blood mononuclear cells were isolated to quantify DNA damage by using the alkaline version of the Comet Assay [14] and both intracellular ROS levels and mitochondrial membrane potential (MMP) flow-cytometrically (Guava InCyte software; Millipore, Burlington, MA, USA) [15] using 2-7-dichlorodihydro-fluorescein diacetate (DCFH-DA) [12] and 5′,6,6′-tetrachloro-1,1′,3,3′-tetraethylbenzimidazolylcarbocyanine iodide (JC-1) [14] fluorescence probes, respectively.
Statistical analysis
Average data were calculated for the three groups according to the amount of PA recorded and, for each one, data as mean±standard error of mean are reported. Significance of differences between before and after 3 months of trial and among groups were calculated using paired and unpaired Student's t-test. Pearson's correlation coefficient was used to evaluate the correlations with the daily exercise. P≤0.01 and P≤0.05 are considered statistically highly significant and significant.
RESULTS
Participants and physical activity
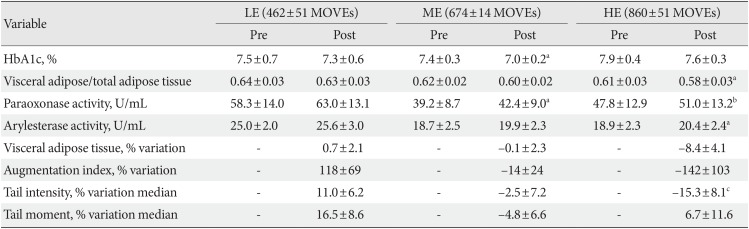
The patients were distributed according to the level of daily PA recorded by MyWellness Key and they were divided into three homogenous groups, according to MOVE [10]: high exercise (HE; 860±51 MOVEs), medium exercise (ME; 674±14 MOVEs) and low exercise (LE; 462±51 MOVEs) groups. No significant differences were observed at baseline among groups in relation to age distribution, anthropometric characteristics and values of HbA1c (data not shown).
Hematochemical analysis
Lipid profile remained unchanged following the trial independently of the amount of PA. On the contrary, all groups presented a reduction in the levels of HbA1c, although the variation was significant only in ME group (P=0.03) (Table 1).
Clinical analysis
Although no significant differences in terms of lean and total adipose tissues were observed (data not shown), in HE group visceral adipose tissue showed a decreasing trend (P=0.08) that resulted significant when normalized by total adipose tissue (P=0.03) (Table 1). Simultaneously, more active patients showed an improvement of endothelial functionality highlighted by a considerable decrease in the percent variation of AI compared to LE group close to significance (P=0.06). This data is also supported by a significant negative correlation between average daily MOVEs and AI % variation (R2=0.247, P=0.04). Finally, a slightly decrease of systolic blood pressure was observed in the HE (pre: 135±5 mm Hg; post: 127±5 mm Hg; P=0.08).
Biochemical analysis
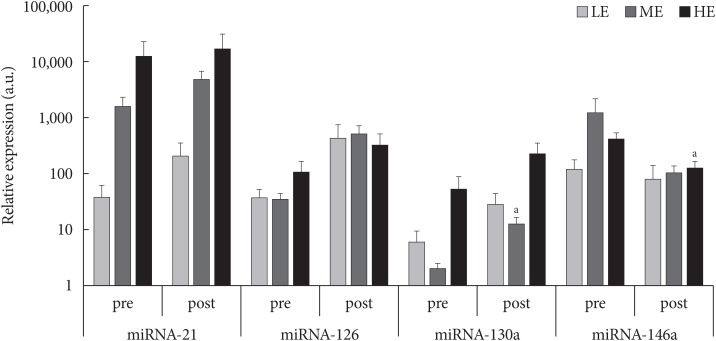
PON-1 paraoxonase and arylesterase enzymatic activities were significantly modulated by PA particularly in the more active patients, while in the ME group only paraoxonase activity was enhanced (Table 1). Flow-cytometric analyses highlighted no significant differences after 3-month of monitored intervention in terms of intracellular ROS production and MMP (data not shown). However, DNA damage, proportional to the comet tail intensity, differs significantly among the groups of less active and more active patients (P=0.03) (Table 1) and it was inversely correlated with the amount of PA (R2=0.379, P=0.01). Similarly, a slight negative correlation between average daily MOVEs and oxidized LDL/total LDL after 3 months of monitored activity was observed (R2=0.244, P=0.06). Finally, as shown in Fig. 1, among microRNA expression levels evaluated, microRNA-130a was up-regulated in ME group (P=0.05) whereas microRNA-146a was down-regulated in the HE one (P=0.05).
DISCUSSION
The present study evaluates the effects of PA recorded for 3 months in diabetics on hematochemical, clinical, and biochemical parameters. The inverse correlation between daily MOVEs and both oxidized LDL level and the extent of oxidative DNA damage, underline the important role of PA in counteracting oxidative stress in conditions of redox imbalance frequent in diabetes. These effects are likely due to a dose-dependent hormetic adaptive response.
An increase in PON-1 paraoxonase and arylesterase activities was observed in all experimental groups but a significant level was reached only in the most active patients showing an improvement in HDL-C with anti-atherogenic properties. This might have concurred to the observed dose-dependent decrease in plasma oxidized LDL level.
Notably, exercise dose significantly correlated with improvement in vascular stiffness expressed as AI and decrease in oxidative damage. Taken together, both correlations support the protective antioxidant role of exercise toward endothelium-derived NO. In fact, exercise-induced antioxidant defense likely protect NO limiting its oxidation by circulating ROS and therefore promoting its bioavailability [16].
PA in the most active group was also able to positively influence other cardiovascular risk factors such as visceral/total adipose tissue ratio, systolic blood pressure, although not significantly, and to down-regulate microRNA-146a, a marker of a senescence-associated pro-inflammatory status in vascular cells [17].
However, ME group benefited of PA both in terms of HbA1c decrease and microRNA-130a up-regulation, both considered relevant cardiovascular risk indexes [1819]. Finally, unaltered plasma lipid profile following PA is not surprising, taking into consideration both the normal baseline values of enrolled patients and the unclear role of training in this respect as showed by Kelley and Kelley [20].
In conclusion, the innovative aspect of the study is represented by the precise monitoring of all daily PA performed by patients, highlighting the inverse correlation between the amount of MOVEs and some cardiovascular risk factors associated with diabetes.
Moreover, the present study highlights the relevance of the novel methodological approaches proposed and identifies interesting new microRNA biomarkers that warrants future investigation on the role of PA in lowering cardiovascular risk in diabetic patients.
 XML Download
XML Download