

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Obesity is a leading health problem in modern society, and its economic burden is continuously increasing [12]. The prevalence of obesity has doubled since 1980 in more than 70 countries worldwide, including Korea [1]. The risk of diverse chronic diseases, including cardiovascular disease, diabetes mellitus, some types of cancer, and musculoskeletal diseases is increased by obesity [3456]. Although obesity is caused by a complex interplay of genetic and environmental factors, over-nutrition is pivotal among the factors that contribute to obesity [7]. Thus, in addition to pharmacologic agents, various meal plans and food supplements have been proposed in an attempt to address the obesity problem.
Diets with a relatively high protein content (i.e., 20% to 30% of total daily intake) are effective in weight control [8]. High protein diets increase satiety, which reduces total energy intake and energy expenditure, both of which contribute to weight loss [8]. Moreover, a premeal supplementation of protein can also induce weight loss and have beneficial effects on cardiometabolic risk factors [910]. An acute premeal load of whey protein increased satiety and delayed gastric emptying, which led to reduced food intake [1112]. Whey protein contains an abundant source of amino acids and bioactive peptides and affects the secretion of gut hormones. It has been shown to increase the secretion of anorexic hormones including glucagon-like peptide-1 (GLP-1), peptide YY (PYY), and cholecystokinin and to decrease the secretion of the orexigenic hormone ghrelin [13]. The intake of soy protein, another source of protein, was also shown to increase PYY and decrease ghrelin [14].
Dietary fiber also has metabolic benefits and can be a suitable companion to protein supplementation in a nutrition therapy for metabolic diseases. Dietary fiber is a complex carbohydrate that resists digestion and absorption in the small intestine [15]. Its physicochemical property can increase satiety by increasing chewing time and the luminal viscosity of the intestine [16]. In addition, the fermentation of dietary fiber by gut bacteria produces short chain fatty acids (SCFAs), which were shown to increase the secretion of GLP-1 and PYY in rodent models [17]. Thus, dietary fiber and protein may have additive effects on gut hormone secretion, satiety, and food intake.
We made a bar-type premeal supplement that contained 9.3 g of whey protein, 1.4 g of soy protein, and 12.7 g of dietary fiber. Previously, we showed its effect on reducing postprandial glucose excursion after a mixed meal load in individuals with type 2 diabetes mellitus or normal glucose tolerance, which was associated with increased insulin and GLP-1 secretion [18]. In the current study, we investigated the effect of the premeal bar on food intake and gut hormone secretion in healthy individuals.
METHODS
Study protocol
We recruited healthy individuals in this study. Inclusion criteria were age between 19 and 80 years, body mass index (BMI) of 18.5 to 35 kg/m2, no prior diagnosis of diabetes mellitus, fasting plasma glucose <100 mg/dL and glycosylated hemoglobin (HbA1c) <6.0% [19]. Individuals with allergies to flours, nuts, legumes, and milk; previous history of abdominal surgery; and any chronic illness requiring continuous medications were excluded. We compared the effects of premeal consumption of water only (as a control), a usual bar (UB) or a protein-enriched, dietary fiber-fortified bar (PFB) on total energy intake. The subjects visited the Clinical Trial Center of the Seoul National University Hospital on 3 separate days at 8:30 AM after 12 hours of overnight fasting at least 1 week apart. An intravenous catheter was placed on their non-dominant arm for blood sampling. The baseline blood sample was obtained and appetite and fullness were measured by visual analog scale (VAS). Water (180 mL of still water) only, the UB and water, or the PFB and water were provided to the subjects (at −15 minutes) at each visit in a randomized order. After 15 minutes, they ate an ad libitum test meal. Venous blood was sampled, and appetite and fullness were measured before (at 0 minutes) and every 30 minutes until 120 minutes after the start of the test meal. Serum and plasma were separated immediately by centrifugation and stored at −70℃ for further analyses.
The study protocol was approved by the Institutional Review Board of the Seoul National University Hospital (IRB No. 1705-091-855) and registered at ClinicalTrial.gov (NCT 03431233). The study was conducted in accordance with the Declaration of Helsinki [20]. All participants provided written informed consent.
Test meal and premeal bar
We provided gimbab as a test meal. Gimbab is a Korean dish made from cooked rice and other ingredients, including vegetables and meats that are wrapped with gim (also known as nori), a dried sheets of laver seaweed. The gimbab was sliced and served in bite-sized portions. Each slice contained very similar proportions of nutrients. We measured the total amount of the intake in grams. In terms of calories, the test meal had 161.1 kcal per 100 g and was composed of protein (10.6%/total dry weight), fat (8.1%/total dry weight), and carbohydrate (81.3%/total dry weight). All test meals were prepared with a standardized recipe.
The PFB and UB were made by Ssial Food Inc. (Jecheon, Korea). One serving of PFB (30 g) had 73 kcal and contained 0.4 g of carbohydrate, 9.3 g of whey protein, 1.4 g of soy protein, 0.3 g of fat, and 12.7 g of dietary fiber. The ingredients of the PFB were whey protein (36.7%), soy protein nuggets (5.4%), acacia gum (24.6%), glycerin fatty acid esters (0.4%), stevia (0.6%), indigestible maltodextrin (25.8%), D-sorbitol (6.4%), citric acid (0.1%), and vanilla extract (0.1%). The UB had same calories as the PFB (73 kcal) and contained 13.9 g of carbohydrate, 0.9 g of soy protein, and 1.8 g of fat. The UB was not fortified with protein or dietary fiber.
Measurements
Appetite and fullness were measured by VAS, with a 1 to 10 score. The plasma glucose level was measured by the glucose oxidase method (YSI 2300 STAT Plus analyzer; YSI Inc., Yellow Springs, OH, USA). Plasma insulin, GLP-1, PYY and active ghrelin were measured by a magnetic bead panel multiplex assay (HMHEMAG-34K-04; Merck Millipore, Darmstadt, Germany). All assays were performed according to the manufacturer's instructions.
Study endpoints
The primary endpoint of the study was the total energy intake, including the calories of the premeal supplements. The secondary endpoints were the amount of total calorie intake at 30 minutes (from −15 to 30 minutes), amount of test meal intake (from 0 to 30 minutes or from 30 to 120 minutes), changes of appetite, fullness, plasma glucose, insulin, GLP-1, PYY, and active ghrelin levels.
Statistical analysis
The baseline characteristics were presented as the mean±standard deviation (SD) for continuous variables or number (%) for categorical variables. The results were presented as the mean±SD in tables and the mean±standard error of the mean in graphs, unless otherwise indicated. The food intake was analyzed by repeated-measures analysis of variance (ANOVA) with Tukey's post hoc test. The plasma glucose, insulin, GLP-1, PYY, and active ghrelin were analyzed by two-way ANOVA as for time and premeal supplement matched by repeated measures with Tukey's post hoc test. The Pearson correlation coefficient was calculated for the correlation between two continuous variables. The incremental area under the curve (iAUC) was calculated using the trapezoidal rule. Net area under the curve (AUC), which is a net of iAUC and decremental AUC, was calculated for plasma ghrelin levels. A P<0.05 was considered statistically significant. All data were analyzed by GraphPad Prism 7 (GraphPad Software, La Jolla, CA, USA).
RESULTS
Food intake, appetite, and fullness
A total 20 healthy subjects were enrolled and completed the study. The baseline characteristics of the subjects are summarized in Table 1. The subjects had a mean age of 31.4±8.6 years and a BMI of 23.6±3.9 kg/m2. The range of HbA1c was 4.6% to 5.6%. Energy intake was considered in two ways: total energy intake (including the calories of the PFB or UB) and test meal energy intake (excluding the calories of the PFB or UB). The primary endpoint, the total energy intake, was significantly lower after the PFB preload than after the water preload (904.4±534.9 kcal vs. 1,075.0±508.0 kcal, P=0.016) (Table 2, Fig. 1A). Compared to the UB preload, the PFB preload reduced the total energy intake by only marginal statistical significance (P=0.078). The test meal energy intake was significantly reduced by the UB and PFB preloads compared with the water preload, with a tendency toward a greater reduction by the PFB than the UB preload (Table 2). For the first 30 minutes, the test meal intake was significantly lower after the PFB preload than after the water or UB preloads (Table 2, Fig. 1B). The test meal intake from 30 to 120 minutes was significantly lower after the PFB preload than after the water preload, but it was not different between the UB and PFB preloads.
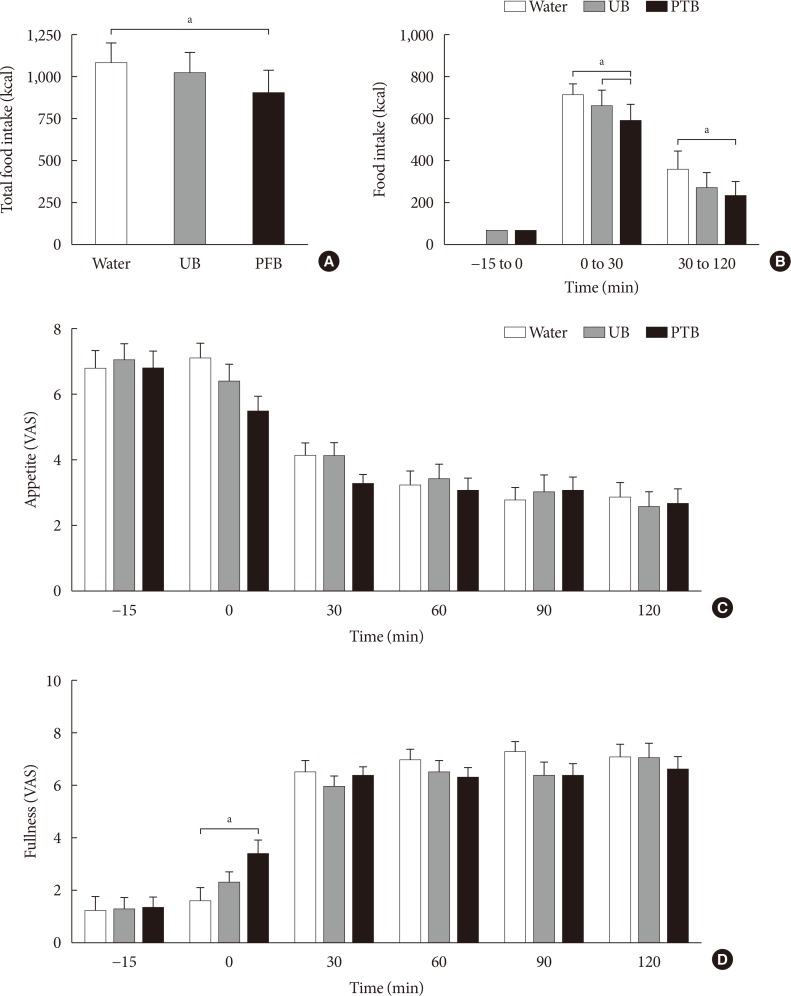

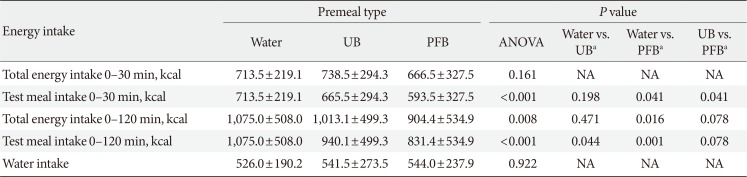
Fig. 1
The total energy intake for 120 minutes (A) and energy intake of each time interval during the study (B), changes of appetite (C), and changes of fullness (D) after each premeal supplementation. Data are mean±standard error of the mean. (A) P for analysis of variance (ANOVA) was 0.008, (B) P for ANOVA for 0 to 30 minutes and for 30 to 120 minutes were <0.001 and 0.032, respectively. (C) For appetite, P for time was <0.001, P for preload was 0.560, and P for time-by-preload interaction was 0.469. (D) For fullness, P for time was <0.001, P for preload was 0.880, and P for time-by-preload interaction was 0.011. UB, usual bar; PFB, protein-enriched dietary fiber-fortified bar; VAS, visual analog scale. aP<0.05 by post hoc analysis.
![]()
Table 1
Baseline characteristics of the subjects
Values are presented as mean±standard deviation or number (%).
BMI, body mass index; BP, blood pressure; HbA1c, glycosylated hemoglobin; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; AST, aspartate transaminase; ALT, alanine transaminase; GFR, glomerular filtration rate.
![]()
Table 2
Comparison of energy intake
![]()
Subjective appetite and fullness after the three preloads are depicted in Fig. 1C and D. Baseline appetite and fullness were not different between the three different preloads. Immediately after intake of the UB and PFB (at 0 minutes), appetite tended to decrease and fullness tended to increase. There was a significant time-by-preload interaction for fullness (P=0.011), but not for appetite (P=0.469). In a post hoc analysis of each time point, at 0 minutes when subjects started eating the test meal, the PFB preload significantly increased fullness compared with the water preload (P=0.006).
Plasma glucose, insulin, and gut hormone secretion
There was a significant time-by-preload interaction for plasma glucose levels (P<0.001) (Fig. 2A and B). The postprandial glucose levels at 30 and 60 minutes after the start of the test meal were significantly lower for the PFB preload than for both the UB and water preloads. However, there was no significant difference in plasma insulin levels between the three types of preloads, although the PFB preload showed a trend of a higher early postprandial insulin level at 30 minutes and a lower insulin level at 120 minutes (Fig. 2C and D). The insulinogenic index of 30 minutes, which is (insulin 30 min–insulin 0 min)/(glucose 30 min–glucose 0 min), was significantly increased after PFB preload compared to water or UB preloads (Supplementary Fig. 1). There was significant time-by-preload interaction for plasma GLP-1 levels (P<0.001) (Fig. 2E). The plasma GLP-1 levels at 30 minutes after the start of the test meal were significantly higher with the PFB preload than with both the UB and water preloads. Likewise, the iAUC of GLP-1 was significantly higher for the PFB than for both the UB and water (6,173.6±3,834.2 pg/mL/min for PFB vs. 2,731.6±2,620.1 pg/mL/min for UB or 3,086.0±2,433.0 pg/mL/min for water, P<0.001 for ANOVA and post hoc comparisons) (Fig. 2F). Plasma PYY levels started to increase after the intake of the PFB and UB preloads, which were further augmented after the test meal intake; however, there was no significant difference among the three types of preloads (Fig. 2G). The iAUC of PYY showed only a tendency to be higher with the PFB or UB preload than with the water preload (Fig. 2H). Plasma active ghrelin levels were decreased after the start of the test meal, but there was no significant difference among the three groups (Fig. 2I). The iAUC of active ghrelin showed only a tendency to be lower after the PFB preload than after the UB or water preload (Fig. 2J).
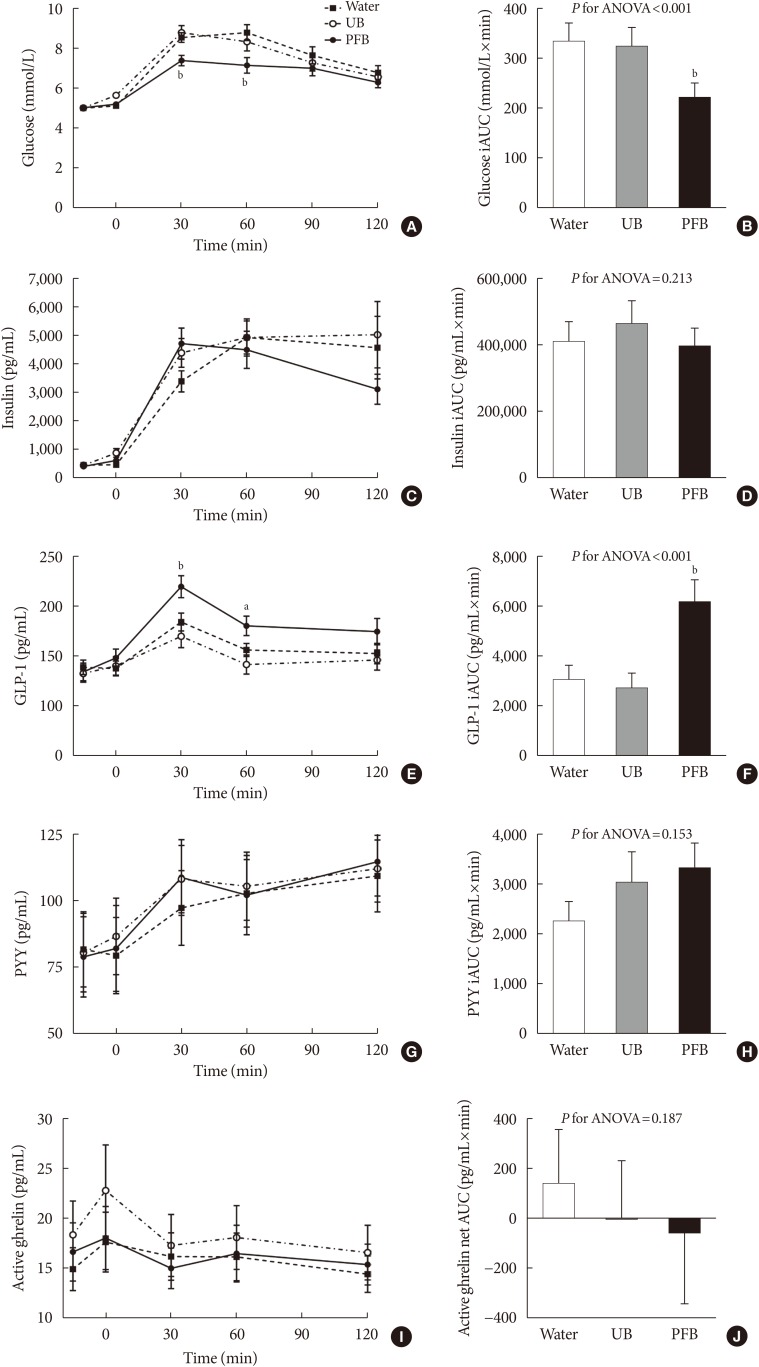
Fig. 2
The changes of (A) plasma glucose, (C) insulin, (E) glucagon-like peptide-1 (GLP-1), (G) peptide YY (PYY), (I) active ghrelin levels, and (B, D, F, H, J) their incremental area under the curves (iAUCs), respectively, after each premeal supplementation. Data are mean±standard error of the mean. (A) For glucose, P for time was <0.001, P for preload was 0.102, and P for time-by-preload interaction was <0.001. (C) For insulin, P for time was <0.001, P for preload was 0.649, and P for time-by-preload interaction was <0.183. (E) For GLP-1, P for time was <0.001, P for preload was 0.096, and P for time-by-preload interaction was <0.001. (G) For PYY, P for time was <0.001, P for preload was 0.972, and P for time-by-preload interaction was <0.638. (I) For active ghrelin, P for time was 0.017, P for preload was 0.710, and P for time-by-preload interaction was 0.912. UB, usual bar; PFB, protein-enriched dietary fiber-fortified bar; AUC, area under the curve. aP<0.05 by post hoc analysis between PFB and water control, bP<0.05 by post hoc analysis both for PFB vs. UB and PFB vs. water control.
![]()
Correlation analysis between food intake and plasma insulin or gut hormone levels
We investigated which hormonal factors were responsible for the decrease of energy intake after the PFB preload compared to the water preload. Interestingly, the difference in plasma PYY levels at −15, 0, and 30 minutes and the AUC of PYY between the PFB and water preloads showed a significant negative correlation with the difference in the energy intake between the two groups for the first 30 minutes (all P<0.05) (Supplementary Table 1). The difference in the plasma PYY level at 30 minutes numerically showed the highest negative correlation with the difference in the energy intake for 30 minutes (r=−0.541, P=0.014) (Fig. 3).
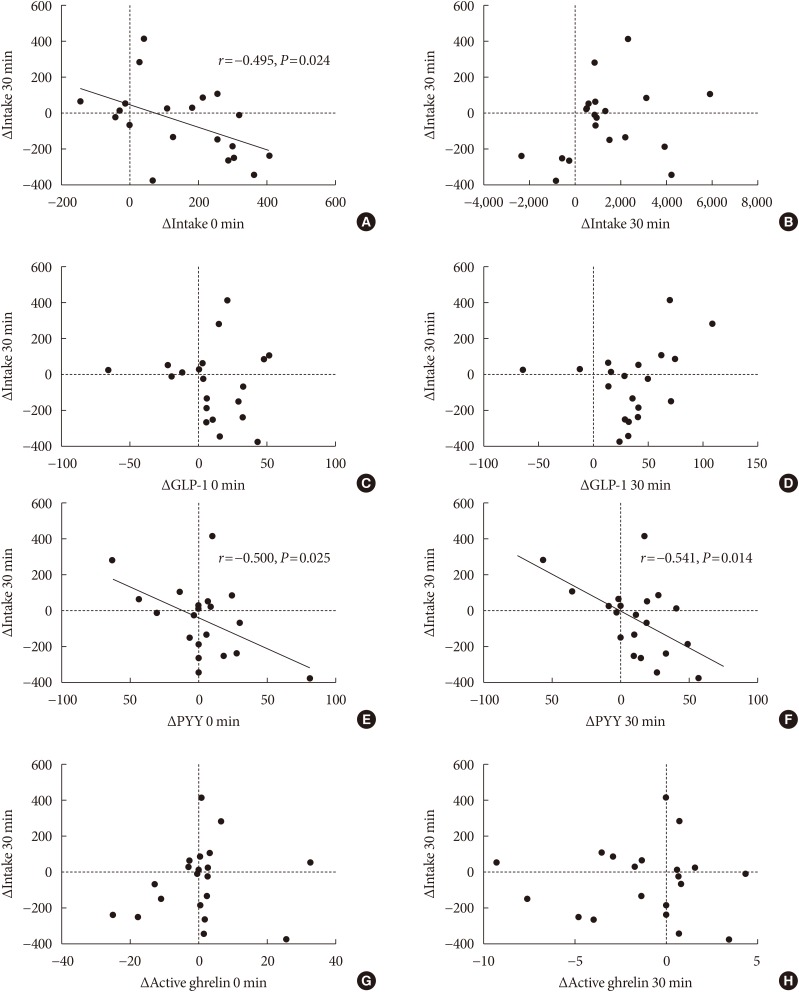
Fig. 3
Correlation analyses of the difference in energy intake for the first 30 minutes and the difference in the (A) insulin at 0 minute, (B) insulin at 30 minutes, (C) glucagon-like peptide-1 (GLP-1) at 0 minute, (D) GLP-1 at 30 minutes. (E) peptide YY (PYY) at 0 minute, (F) PYY at 30 minutes, (G) active ghrelin at 0 minute, and (H) active ghrelin at 30 minutes between the protein-enriched dietary fiber-fortified bar (PFB) and water preloads. Linear regression analysis was done for each parameter. The difference in insulin at 0 minutes, PYY at 0 minutes, and PYY at 30 minutes were only significantly correlated with the difference in energy intake for the first 30 minutes between the PFB and water preloads.
![]()
DISCUSSION
In this study, we investigated the effect of a premeal supplement fortified with a modest amount of protein and dietary fiber on food intake and gut hormone secretion. Not only the energy intake of the subsequent test meal but also the total energy intake including the calories of the premeal supplement itself was significantly lower after the PFB preload than after the water preload. The UB, which had same of calories as the PFB but was composed of mainly carbohydrates, did not reduce the total energy intake. Along with the lower energy intake, the PFB preload decreased the postprandial glucose levels and increased GLP-1 secretion.
A premeal load of protein has been shown to reduce subsequent food intake [9]. An acute load of protein delays gastric emptying and increases satiety, which were associated with protein's effect on gut hormone secretion, including an increase of GLP-1, PYY, and CCK and a decrease of ghrelin [89]. In a previous study, either a whey or soy protein preload (45 to 50 g) increased satiety and reduced subsequent pizza intake compared to egg albumin [21], which indicated that different sources of protein may act differently on satiety and food intake. In another study, whey protein (50 g) reduced energy intake at a subsequent buffet meal compared to a glucose preload [22]. In line with these acute preload studies, long-term premeal supplementation with whey protein (56 g/day) showed a modest reduction of body weight (−1.8 kg) for 23 weeks compared with maltodextrin supplementation [23]. In combination with a low calorie diet (1,400 kcal/day), a whey protein premeal supplementation (50 g) reduced body weight (−8.0%) compared to maltodextrin (−4.1%) for 6 months [24]. However, these studies used fairly large amounts of protein. The protein supplement itself provides a significant amount of calories, which might limit its weight loss effect. In a previous study, different doses of whey protein (10 to 40 g) reduced the energy intake of a subsequent test meal in a dose-dependent manner, where the reduced test meal intake was observed with 20 g or more of whey protein [11]. However, the total energy intake, including whey protein, was not changed, even with the highest dose of whey protein [11]. Thus, we thought that it might be a good strategy for weight loss to combine another premeal supplement which has additive effects to the protein supplement.
In this regard, adding dietary fiber might make a good combination for the protein supplement because it provides low amount of calories and has beneficial biologic effects that are additive to the protein supplement in increasing satiety and, thereby, reducing energy intake [15]. The physicochemical property of dietary fiber can directly contribute to the increased satiety by bulk formation and high viscosity, which may result in decreased gastric emptying [25]. In addition, fermentation of dietary fiber by gut bacteria produces SCFAs, which may exert various biologic effects through the activation of cognate receptors, G-protein coupled receptor 41 (GPR41)/free fatty acid 3 (FFA3) and GPR43/FFA2 [26]. GPR43 is present in enteroendocrine L-cells, which secrete GLP-1 and PYY, and SCFA stimulates the secretion of these gut hormones from L-cells through GPR43 in vitro [17]. Colonic infusion of propionate, an SCFA, stimulated the secretion of GLP-1 and PYY, which was attenuated by GPR43 knockout in mice [17]. SCFA was also reported to suppress fat accumulation in the adipose tissue through the action of GPR43 [27]. In a study involving 2,909 healthy subjects from a multicenter population-based cohort, dietary fiber consumption was associated with body weight, waist-to-hip ratio, fasting insulin and other cardiovascular risk factors [28]. In addition, a systematic review and meta-analysis revealed that the supplementation of soluble dietary fiber for 2 to 17 weeks significantly reduced body weight compared to placebo [29]. In a study with young healthy adults, having evening meal of boiled barley kernel (12.2 g of dietary fiber), compared to white wheat bread (3.0 g of dietary fiber), reduced hunger and food intake on the following day [30]. We previously reported that dietary fiber-enriched cereal reduced postprandial glucose excursion compared to conventional cereal in patients with type 2 diabetes mellitus [31], which also suggests possible benefit of dietary fiber supplementation on glucose metabolism.
We used a modest dose of protein, 10.7 g (9.3 g of whey protein and 1.4 g of soy protein). To see acute effects, most previous studies used protein in a dosage that ranged from 25 to 60 g; there are only a few studies that used smaller doses of protein. In a study with 16 healthy young males, 10 g of whey protein did not reduce the subsequent food (in this case, ad libitum pizza) intake, while higher doses (>20 g) of whey protein did reduce the subsequent food intake [11]. In another study with 11 male patients with type 2 diabetes mellitus, 15 g of whey protein preload decreased postprandial glucose excursion and increased satiety, while the gut hormone responses, including GLP-1, were not significantly changed [32]. In contrast, in the current study, a modest dose of whey protein when combined with dietary fiber significantly reduced energy intake of a subsequent test meal by 23% and total energy intake by 16%, which was accompanied by a significant augmentation of the GLP-1 response. Our results suggest that a premeal supplementation of protein and dietary fiber may have an additive or synergistic effect on satiety, food intake and GLP-1 secretion.
In our study, the PFB affected the secretion of gut hormones after the test meal intake. Thus, we examined which gut hormones contributed to the difference in energy intake between the PFB and water preloads. GLP-1 was prominently increased after the PFB preload compared to both the UB and water control. However, the difference in GLP-1 did not correlate with the difference in energy intake between the PFB and water preloads. In contrast, the difference in plasma PYY levels between the PFB and water preloads showed a negative correlation with the difference in food intake, which indicates that increased PYY secretion may contribute to the reduced test meal intake. Furthermore, there was a tendency toward more PYY secretion with the PFB preload than with the water preload. It is well known that PYY, which is secreted by the eneteroendocrine L-cell, acts directly on the NPY neuron in the arcuate nucleus and exerts an anorectic effect [33]. Similarly, in one study, where the subjects had a premeal supplement of whey protein and after 3 hours had an ad libitum buffet meal, the energy intake also showed a significant negative correlation with PYY levels but not with the GLP-1 levels [12]. These results suggest that PYY might have a role as a regulator for energy intake after whey protein consumption.
The insulinogenic index of 30 minutes was higher after PFB preload than water or UB preloads. This suggests that the relative insulin secretion considering the glucose increment was higher after PFB preload. First of all, the higher postprandial GLP-1 secretion could contribute to the increased insulin secretion, which was possibly induced by the protein component of PFB. The protein component in ingested food can directly stimulate intestinal L-cell to secrete GLP-1. In previous studies, protein hydrolysates stimulated GLP-1 secretion in a perfused rat ileum and in immortalized human L-cells [3435]. Dietary fiber also can contribute to the increased GLP-1 secretion. As formerly mentioned, the SCFA which can be produced from the fermentation of dietary fiber in the intestine can stimulate L-cells to secrete GLP-1 [17]. These studies suggest that the protein and fiber contents of PFB could contribute to the enhanced postprandial insulin secretion.
Our study has several limitations. First, the premeal supplement had multiple ingredients besides protein and dietary fiber. These ingredients could have their own effects on satiety and gut hormone secretion. Second, we used gimbab as the test meal. Although gimbab is a very popular food for Koreans, other meals with different nutrient compositions might show different results. Third, we did not measure the gastric emptying time, which can be affected by whey protein and dietary fiber.
In conclusion, acute premeal supplementation of a modest amount of protein and dietary fiber decreased caloric intake and postprandial glucose, which was associated with marked GLP-1 secretion. The long-term effects of the PFB on obesity and metabolic disorders should be explored.
 XML Download
XML Download