

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The genes of human cytomegalovirus (CMV) chronically exists in the host myeloid lineage including CD34+ hematopoietic progenitor cells as extrachromosomal plasmid after asymptomatic or self-limited primary lytic infection that occurs during childhood and adolescence [123]. Unlike other viruses of Herpesviridae family, latently established CMV can express a handful of transcripts such as latency-associated unidentified nuclear antigen (LUNA), UL81-82 antisense transcript, and latency-associated homolog of interleukin-10 (LAcmvIL-10) together with periodic active replication events during the life-long [24567]. The outstanding feature of sleepless latency leads to the extraordinary expansion of CMV-specific resting effector memory CD8+ T-cell subpopulation and then chronic inflammatory condition as well as dysregulation of host immune mechanisms [789101112]. This long-term pathophysiologic mechanisms of CMV acquisition may be the direct cause of chronic inflammatory cardiovascular diseases (CVDs) or autoimmune diseases including systemic lupus erythematosus and systemic sclerosis [1314].
Although the pathogenesis of type 2 diabetes mellitus (T2DM, non-insulin-dependent diabetes mellitus [DM]) is quite complex and involves various cross-linked molecules including adipocytokines, receptors, and genetic pathways as well as immune system, T2DM seemed to be a fundamentally chronic low-grade inflammatory metabolic disease with clinical detrimental effects through various micro- and macrovascular complications [15161718192021]. Lohr and Oldstone [22] detected the CMV immediate-early and late gene products using reverse transcription polymerase chain reaction (PCR) and in situ hybridization in pancreatic tissues of T2DM patients. Recent studies suggested that viperin (endoplasmic reticulum-associated, interferon-inducible virus inhibitory protein), which is directly induced by CMV, may play a role in lipid and glucose metabolism through interaction with the CMV mitochondrial inhibitor of apoptosis (vMIA) protein [2324].
Considering these molecular biological experiments, we hypothesized that CMV diseases may contribute to the development of T2DM. Although only a few clinical studies evaluating the association between CMV and T2DM were performed nearly 2 decades ago, these studies evaluated CMV seroepidemiology measured by anti-CMV immunoglobulin G (IgG) antibody test or titer, to determine previous CMV exposure and latent status by humoral immunity, with age being a variable influence [2526272829]. The anti-CMV IgG is not useful for evaluating CMV-specific cell-mediated immunity (CMV-CMI), which plays a major role in immunosenescence and immune exhaustion caused by CMV [30]. The active replication of whole CMV genes can be delicately categorized into CMV infection and diseases, defined as detection of DNA (DNAemia) or competitive virions (viremia) in the peripheral blood and cytopathic inflammatory end-organ tissue-invasive disease, respectively [30]. The CMV infection or diseases, in relation to more powerful immune boosting of CMV-CMI than anti-CMV IgG serostatus, will better reflect the chronic inflammatory dysregulation phenomenon by CMV-related indirect effect [30].
The impact of CMV infection or diseases on new-onset T2DM had been primarily evaluated as posttransplant DM in adult solid organ transplant recipients [3132]. However, little is known about the causal connection of CMV diseases to T2DM development in the entire population including both transplant and non-transplant patients. Therefore, we performed the general population-based matched case-control cohort study in both immunocompetent and immunocompromised patients to explore whether the CMV diseases contributes to the development of T2DM.
METHODS
Data resource and management process
Our study used the database warehouse of the Korean Health Insurance Review and Assessment Service claims, including the detailed information about all kinds of healthcare utilization in the entire Korean population [33]. A total of 1,188 unduplicated patients with CMV diseases between 2010 and 2014 were extracted using a unique code (V104) for the relief reduction of patients with rare intractable diseases, operated by the South Korean National Health Insurance Service (NHIS) [33]. The healthcare providers should submit the specific document to the NHIS to register this particular payment relief. The V104 code corresponds to B25 (cytomegalovirus disease), B25.0 (cytomegaloviral pneumonitis), B25.1 (cytomegaloviral hepatitis), B25.2 (cytomegaloviral pancreatitis), B25.8 (other cytomegaloviral diseases), and B25.9 (cytomegaloviral disease, unspecified) according to the World Health Organization's 2016 International Statistical Classification of Diseases and Related-Health Problems 10th Revision (ICD-10). To apply the V104 code, the clinicians should confirm the CMV diseases through histopathological exam, culture, shell viral assay, and pp65 antigen test. The presumptive or suspected diagnosis with imaging studies or clinical decision is not permissible. The V104 code does not include congenital CMV infection (ICD-10 code: P35.1) and cytomegaloviral mononucleosis (ICD-10 code: B27.1). The study was approved with waiver of informed consent by the Institutional Review Board of Gangnam Severance Hospital (IRB no. 3-2017-0341) and the NHIS. This study was performed according to the Declaration of Helsinki, the ethical principles for medical research involving human subjects.
Study design and patient selection
We performed the whole population-based matched case-control cohort study. The patients with V104 code of CMV diseases comprised the case group and those without this code comprised the control group. Five hundred and seventy-six case patients of the 1,188 with CMV diseases were finally selected between 2010 and 2014 after excluding 285 patients with previous T2DM before first CMV diagnosis date back to 2006 and another 327 who were aged <20 years. The 2,880 control patients without T2DM between 2006 and cohort entry point were randomly stratified matched by age and sex with the case patients in the same cohort entry year, with a 5:1 ratio. This cohort start and end date were January 1, 2011 and December 31, 2015. The event in the cohort was the development of new-onset T2DM in both case and control group. If subject had the event, their follow-up were ceased. All subject without event were followed until December 31, 2015. If patients were died before event occurrence, they were censored (Fig. 1).
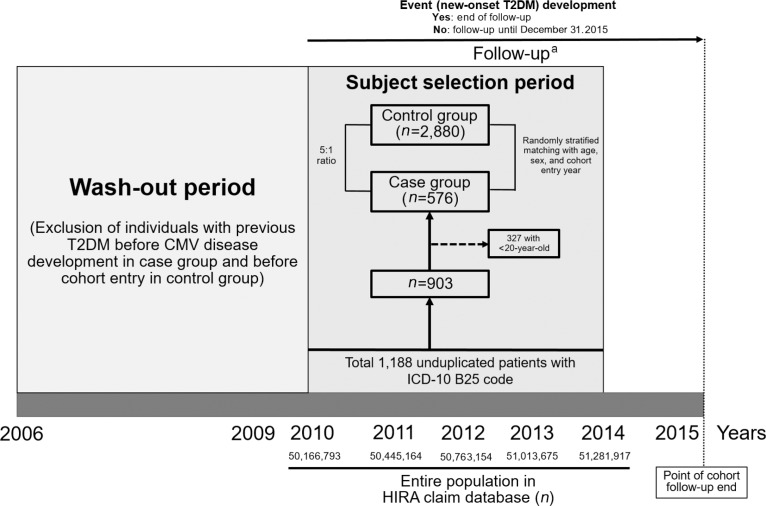
Fig. 1
The process of subject selection by case and control group. T2DM, type 2 diabetes mellitus; CMV, cytomegalovirus; ICD-10, International Statistical Classification of Diseases and Related-Health Problems 10th Revision; HIRA, the Korean Health Insurance Review and Assessment Service. aIf patients were died before event occurrence, they were censored.
![]()
Definition
Lower income status was defined as an annual household income of lower than 25% based on the results of the 2010 South Korea Population and Housing Census. Recurred or refractory CMV diseases cases were defined as patients who received repeat treatments of ganciclovir and/or valganciclovir between 30 days and 1 year after the first CMV diagnosis [34]. We simply expressed the refractory or recurred disease as refractory CMV diseases. Chronic medical diseases were matched with the ICD-10 code of T2DM (E11–E14), hypertension (I10–I13 and I15), dyslipidemia (E78 including E78.0–E78.9), chronic obstructive pulmonary disease (COPD) (J44 including J44.0, J44.1, J44.8, and J44.9), ischemic heart diseases (IHDs) (I20–I25), cerebral infarction (I63, I64), heart failure (HF) (I50), and end-stage renal disease (ESRD) (N18.5). For T2DM diagnosis, we additionally used the anti-diabetic drug description with codes of insulins, sulfonylureas, metformin, meglitinides, thiazolidinediones, dipeptidyl peptidase-4 inhibitors, and α-glucosidase inhibitors along with above ICD-10 codes [35].
Statistical analysis
We used the McNemer test and paired t-test to compare the nominal and continuous variables between the two groups, respectively. We performed the multivariate logistic regression analyses with model 1 (M1, not adjusted), model 2 (M2, adjusted by age and sex), and model 3 (M3, adjusted by age, sex, lower income status, hypertension, and dyslipidemia) to evaluate the impact of adult CMV diseases on new-onset T2DM. The incidence probability of T2DM was analyzed using Kaplan-Meier curves and log-rank test. The two-tailed P values of ≤0.05 were considered significant. Statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
Frequencies of chronic diseases between case and control group
The overall follow-up duration of all participants was about 3 years. There was no significant difference in the proportion of patients aged ≥60 years and with lower income status between case and control group. The case group had significantly higher frequency of new-onset T2DM compared to the control group (5.6% vs. 2.2%, P<0.001) (Table 1). When we divided the total patients (n=3,456) into group with (n=95) new-onset T2DM and group without T2DM (n=3,361), the frequency of CMV diseases was found to be higher in the group with T2DM (33.7% vs. 16.2%, P<0.001) (Supplementary Table 1). The percentages of patients with hypertension, dyslipidemia, COPD, IHD, cerebral infarction, HF, and ESRD were common in the case group (all of P<0.001) (Table 1).
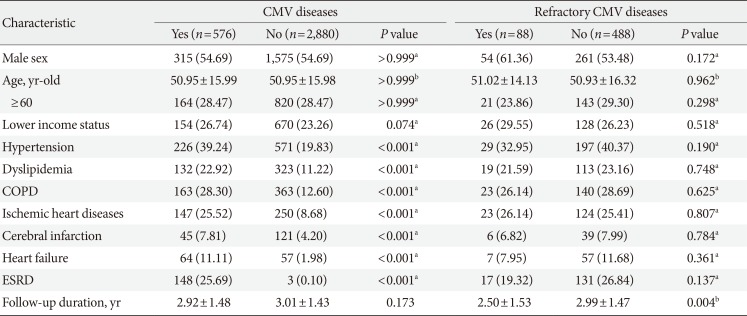
Table 1
Comparison of baseline characteristics between adult individuals with and without cytomegalovirus disease in the matched cohort
![]()
Impact of CMV diseases on the development of new-onset T2DM: subgroup analyses
The incidence rate (IR) per 1,000 T2DM patients in the case group was nearly two-fold higher than that in the control group at M1 (odds ratio [OR], 2.61; 95% confidence interval [CI], 1.69 to 3.96), M2 (OR, 2.60; 95% CI, 1.68 to 3.95), and M3 (OR, 2.06; 95% CI, 1.31 to 3.17) (Table 2). Kaplan-Meier curve showed that the incidence probability of T2DM in the case group was significantly higher than that in the control (P<0.001) (Fig. 2A). In the case group, the subgroup aged ≥60 years had a significantly lower risk of developing T2DM than those aged <60 years (M3 [OR, 1.11; 95% CI, 0.50 to 2.20] vs. [OR, 3.63; 95% CI, 1.97 to 6.65]; P=0.032, respectively). However, there was no significant difference in the OR of sex, lower income status, hypertension, dyslipidemia, COPD, IHD, cerebral infarction, HF, and ESRD (Table 2).
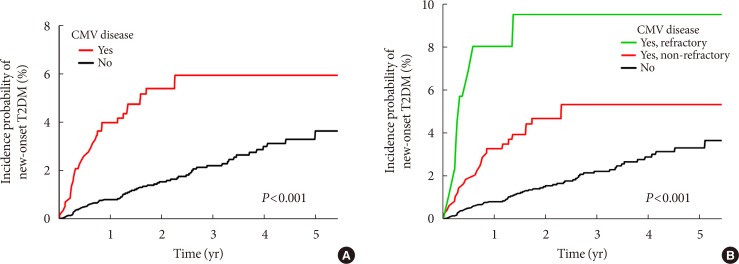
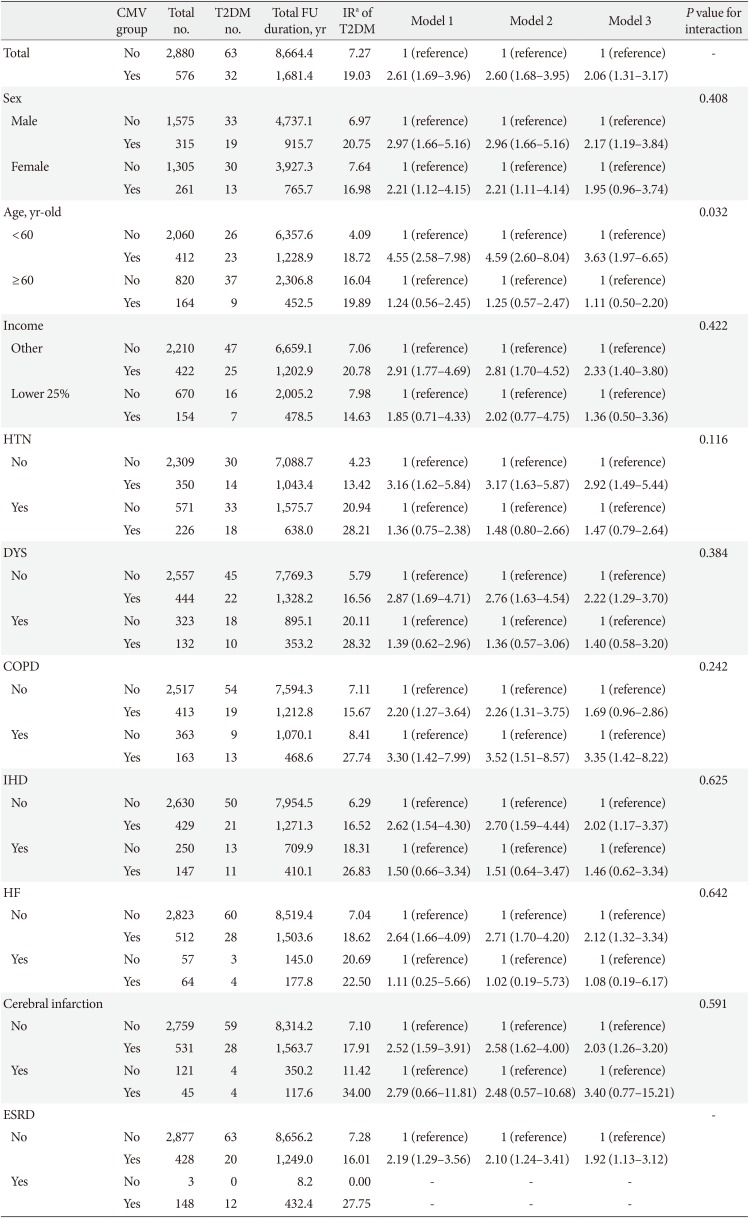
Fig. 2
Kaplan-Meier curve for new-onset type 2 diabetes mellitus (T2DM) incidence according to cytomegalovirus (CMV) disease. (A) Comparison of patients with and without CMV diseases. (B) Comparison of three groups including refractory and non-refractory CMV diseases (P value of log-lank test).
![]()
Table 2
Multivariate logistic regression models to examine the effect of adult cytomegalovirus disease on new-onset of type 2 diabetes mellitus in various subgroups
Values are presented as number or odds ratio (95% confidence interval). Model 1, non-adjusted; Model 2, age- and sex-adjusted; Model 3, age-, sex-, lower income-, hypertension-, and dyslipidemia-adjusted.
CMV, cytomegalovirus; T2DM, type 2 diabetes mellitus; FU, follow-up; IR, incidence rate; HTN, hypertension; DYS, dyslipidemia; COPD, chronic obstructive pulmonary disease; IHD, ischemic heart disease; HF, heart failure; ESRD, end-stage renal disease.
aPer 1,000.
![]()
Difference between refractory and non-refractory CMV diseases in T2DM
In a further analysis conducted in three groups with refractory CMV diseases, the patients with refractory CMV diseases (M3: OR, 4.01; 95% CI, 1.76 to 7.69) had a significantly higher IR of T2DM than those without CMV diseases (reference) or with non-refractory CMV diseases (M3: OR, 1.77; 95% CI, 1.07 to 2.82). There was no significant difference in the ORs between the three groups according to sex and age (P=0.256 and P=0.114, respectively) (Supplementary Table 2). In the Kaplan-Meier curve of the three groups, patients with refractory CMV diseases had the highest IR of T2DM (P<0.001) (Fig. 2B).
DISCUSSION
This study showed that the occurrence of CMV diseases increases the incidence of new-onset T2DM, with a relative risk of ≥200%, which was higher than the CMV-attributable risk of CVD evaluated by meta-analyses (22% and 67%) [1436]. This result was identical with additional analysis from the matched cohort of 3:1 ratio (1,488 of control group and 496 of case group) with age, sex, cohort entry year, lower income status, hypertension, and dyslipidemia as 2.01 of OR (Supplementary Table 3). Interestingly, patients aged <60 years had a higher risk of T2DM after CMV diseases. However, the existence of chronic inflammatory diseases such as hypertension, dyslipidemia, COPD, IHD, cerebral infarction, HF, and ESRD did not influence the incidence of post-CMV T2DM. These findings were consistently derived from different regression models adjusted by clinical factors of usual risks for T2DM [37] and confounding variables showing higher frequencies in patients with CMV diseases (Table 1). The Kaplan-Meier curve indicated that most post-CMV T2DM cases developed shortly after CMV diseases, in particular, within 1 year.
Majority of epidemiological studies evaluating the causal relationship between CMV and metabolic diseases have focused on CVD, especially coronary heart disease (CHD), type I DM, and autoimmune diabetes [13143638]. The meta-analysis conducted by Ji et al. [14] revealed that CMV infection was associated with high risk of CHD. However, only seven (12.7%) among the total 55 studies including the meta-analysis reported the detection of CMV DNAemia by PCR [14]. Interestingly, the OR reported in seven studies was higher than that in studies using CMV seroprevalence (8.12 vs. 1.56, respectively) [14]. A few studies measuring anti-CMV IgG showed that T2DM patients had higher frequency of CMV seropositivity and titer (OR, 2 to 12) than healthy subjects [2627]. In addition, CMV seropositive status was associated with higher glucose levels [26]. However, these studies may have considerable limitations and are underpowered due to the small sample size and rare CMV events and because the specific subjects do not reflect the universal population.
The pathophysiological mechanisms of post-CMV T2DM remain uncertain. Although Lohr and Oldstone [22] revealed that CMV genes existed in the pancreatic islets of Langerhans cells without cytopathic inflammation and Numazaki et al. [39] investigated that CMV was found to replicate in in vitro human fetal pancreatic islet cells in the early 1990s, further studies had not been reported. Yoneda et al. [38] recently reported that the immunologic indirect effect of CMV infection was associated with direct pancreatic β-cell injury, showing T lymphocyte infiltration. The reliability of the experiments conducted in human samples was confirmed although the absence of CMV in normal controls [22,38]. The discrete impact of CMV infection on the failure of islet allografts to support the active CMV replication may be an attributing factor to the development of T2DM through direct and/or indirect pancreatic damages from CMV [40]. On the contrary, we may presume that the substances used in the envelop composition such as viperin, which is essential to extracellular budding and shedding of complete CMV virion, might alter the lipid and glucose metabolism pathways [24].
Our new findings of post-CMV T2DM discrepancy by age group and early development after CMV diseases could provide novel insights for the causative effects of CMV replication in chronic inflammatory diseases including T2DM. Another unique analysis for the refractory nature of CMV diseases, which may suggest prolonged active CMV replication, had earlier development of and more strong relationship with T2DM. The complete lytic reactivation of CMV resulting in end-organ cytopathic disease or DNAemia, especially in the younger population who have more prominent immunologic response than the elderly with profound immunosenescence or subjects who have uncontrolled CMV replication, could lead to deeper deterioration of immune homeostasis. The comprehensive measurement of CMV-specific immunologic profiles using mass cytometry (cytometry by time of flight [CyTOF]) and genetic evaluation for alteration of glucose metabolism by CMV are warranted. If information regarding causative mechanisms in CMV replication and T2DM would be accumulated along with further epidemiologic studies in various ethnic populations, the development of CMV vaccine could be targeted to prevent several chronic inflammatory diseases including T2DM in this era of aging population.
This study has some limitations, same as those of large-scale studies using coding data processing. Therefore, the data collection method could cause the selected disease to be underestimated. However, our analyses can overcome this drawback through a matched case-control design. In addition, the frequencies of CMV diseases incidence according to ICD-10 code showed that our database from the entire population had the majority of B25.8 and B25.9 code (1,025 of 1,188, 86.3%), which may indicate the confirmatory CMV diagnosis driven by pathology in gastrointestinal tract such as esophagus, stomach, duodenum, and colon. The absence of rare cytomegaloviral pancreatitis as well as the minority of cytomegaloviral pneumonitis (75 of 1,188, 6.3%), which could be presumptive or over-diagnosed with chest computed tomography scan or quantitative nucleic acid amplification test in bronchoalveolar lavage without standardization and universal cut-off level for proper diagnosis, will guarantee the validity of our database for the confirmatory CMV tissue-invasive end-organ disease (Supplementary Table 4) [30]. Secondly, our subjects were restricted by South Korean nationality. A previous study showed that the effect of CMV infection on CHD might be different among ethnic groups, with increased risk among Asian populations [14]. In addition, the refractory CMV diseases were identified simply by repeated administration of anti-CMV drugs. The huge database could not allow a more precise definition of clinical information-based refractory cases in each CMV patient. Finally, our cohort includes some proportion of solid organ transplantation recipients of about 20% among total individuals with CMV diseases (Supplementary Table 5). However, the patients with new-onset T2DM had higher frequencies of several chronic inflammatory diseases, including hypertension, dyslipidemia, IHD, cerebral infarction, and ESRD, in the well-known relation to T2DM (Supplementary Table 1) [37]. These basic characteristics will ensure the good quality in this cohort. In addition, the low IR of CMV end-organ disease in general population may make our population-based study worthy to evaluate the relationship of CMV and T2DM.
In spite of these limitations, our study has several strengths and outstanding features: (1) first assessment of the T2DM incidence after CMV diseases including tissue-invasive end-organ damage, but not the CMV serostatus in T2DM patients, (2) long wash-out period for ≥4 years that can discriminate the casual relationship between CMV diseases and T2DM as well as can analyze the post-CMV T2DM, and (3) largest sample size among studies reporting about the relation between T2DM and CMV
In conclusion, our data indicate that CMV diseases increase the development of T2DM. These results suggest that active CMV replication may play an important role in T2DM pathogenesis.
 XML Download
XML Download