

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Endothelial dysfunction is considered as an early marker for atherosclerosis and an early step in atherosclerotic plaque formation, as the endothelium plays a major role in regulating vascular homeostasis via vasodilation, smooth muscle cell function, thrombogenesis, and fibrinolysis [123]. However, there is limited data regarding whether sodium-glucose cotransporter-2 (SGLT2) inhibitors improve endothelial function [456].
Several clinical trials have revealed that empagliflozin and canagliflozin were associated with slower progression of kidney disease and lower rates of clinically relevant renal events [7]. The suggested mechanisms involve reduced glomerular hyperfiltration by modifying tubuloglomerular feedback [8], which could theoretically activate the renin-angiotensin-aldosterone system (RAS) [9]. However, there remains controversy regarding the clinical implications of those findings.
The present study investigated the effects of dapagliflozin and metformin on endothelial function and renal injury markers among drug-naïve patients with type 2 diabetes mellitus (T2DM). The drugs' effects were also evaluated based on glycemic control, insulin resistance, ketogenesis, hemodynamic factors (including blood pressure), RAS, and renal injury markers (urine microalbumin, β2-microglobulin, and N-acetyl-beta-D-glucosaminidase [NAG]).
METHODS
Study design
This prospective, randomized, open-label, 8-week crossover study evaluated drug-naïve patients with T2DM. The study's protocol was approved by the Institutional Review Board of the Seoul National University Boramae Medical Center (26-2014-148), and informed consent was obtained from all participants and/or their legal guardians. The enrollment, randomization, data collection, and data management processes were implemented by third-party entities. The study was registered at ClinicalTrials.gov (NCT0250161).
Participants and treatments
The inclusion criteria were: (1) no treatment for T2DM during the 12 weeks before enrollment; (2) age of 20 to 80 years; and (3) glycosylated hemoglobin (HbA1c) levels of ≥7.0% to ≤9.0%. The exclusion criteria were: (1) type 1 diabetes mellitus or secondary diabetes; (2) a history of ischemic heart disease or stroke; (3) typical chest pain or atypical chest pain with dyspnea; (4) an estimated glomerular filtration rate (GFR) of <60 mL/min/1.73 m2 based on the Modification of Diet in Renal Disease method; (5) pregnancy, breastfeeding, or planning to become pregnant during the study period; and (6) exclusion at the discretion of the attending physician.
The participants were screened for eligibility and within 2 weeks were randomly assigned 1:1 to receive 8 weeks of treatment using either metformin followed by dapagliflozin or dapagliflozin followed by metformin. The starting dose for metformin was 1,000 mg/day and could be increased up to 2,000 mg/day by the attending physician. The starting dose for dapagliflozin was 10 mg/day. The dapagliflozin treatment represents the initial first 8-week treatment in dapagliflozin→metformin group, and later 8-week treatment in metformin→dapagliflozin group in total 22 patients (vice versa for metformin treatment).
Measurement of the reactive hyperemic index
The reactive hyperemic index (RHI) was measured using the Endo-PAT2000 system (Itamar Medical Ltd., Keisarya, Israel) by a technologist who was not otherwise involved in the study. All measurements were performed under fasting conditions during the morning in a temperature-controlled room (25℃). After resting for ≥15 minutes, a pressure cuff was placed on the patient's forearm and inflated to 50 mm Hg above the systolic blood pressure to occlude the brachial artery. The cuff was released 5 minutes later and the diameters of the peripheral artery on the pre- and post-hyperemia images were used to calculate the change in the RHI.
Measurements of laboratory parameters
Concentrations of HbA1c were evaluated using high-performance liquid chromatography with Bio-Rad Variant II HbA1c analyzer (Bio-Rad, Montreal, QC, Canada). Concentrations of total ketone bodies, acetoacetate, and β-hydroxybutyrate were measured using gas chromatography/mass spectrometry with a gas chromatography/mass selective detector (Hewlett Packard, Palo Alto, CA, USA). Concentrations of nitrotyrosine and endothelin were evaluated using the Nitrotyrosine ELISA kit (Cell Biolabs Inc., San Diego, CA, USA), and Quantikine ELISA kit (R&D Systems, Minneapolis, MN, USA). Concentrations of β2-microglobulin were measured enzymatically using a β2-microglobulin kit (Immunotech, Prague, Czech) and concentrations of NAG were measured using the CicaFit NAG (Kanto Chemical Co., Tokyo, Japan).
Statistical analysis
Outcomes were evaluated using the full analysis set, which included all participants who were enrolled and assigned a treatment. Normally distributed data were presented as mean±standard deviation, non-normally distributed data were reported as median (interquartile range [IQR]), and categorical data were reported as number (%). The Mann-Whitney U test and Wilcoxon signed-rank test were used to analyze continuous variables and Fisher's exact test was used to analyze categorical variables. Differences were considered statistically significant at P values of <0.05 and all analyses were performed using IBM SPSS software version 22.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics
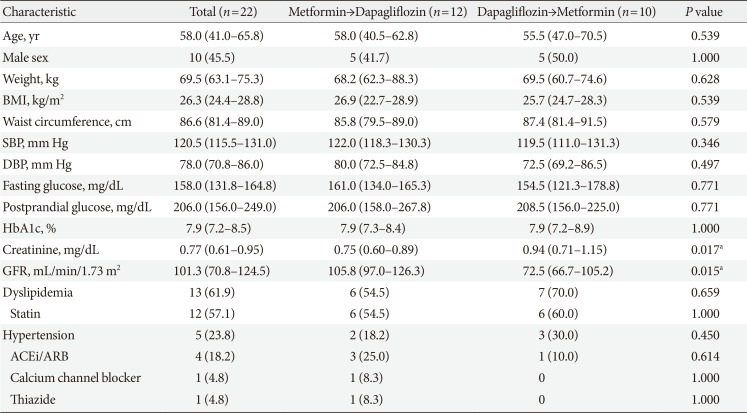
The participants' baseline characteristics are shown in Table 1. Twenty-three participants were originally enrolled, although one patient dropped out before the randomization and treatment. The groups had similar values for age, sex, body weight, body mass index, waist circumference, blood pressure, smoking status, medical history, fasting and postprandial glucose levels, and HbA1c levels. However, the group that received dapagliflozin first had significantly higher creatinine levels than the group that received metformin first (Table 1).
Changes in metabolic parameters
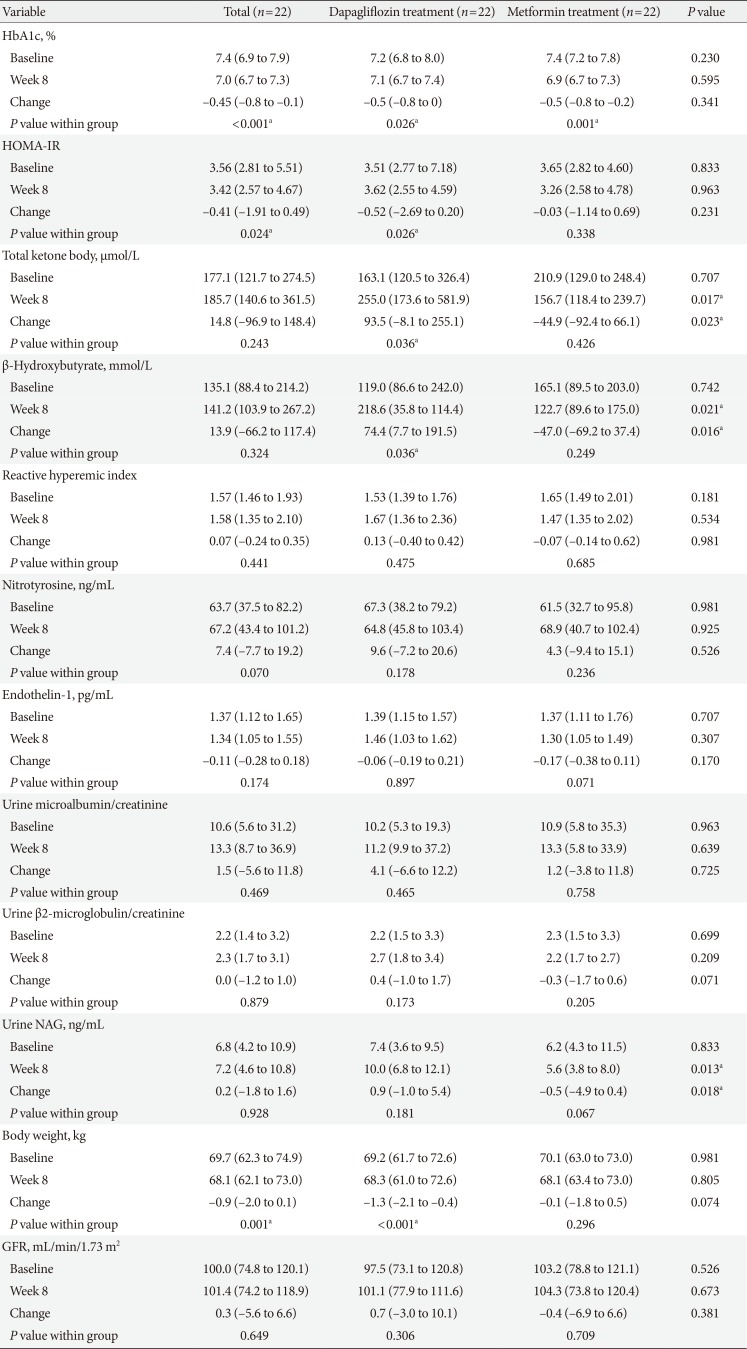
Both treatments significantly reduced the HbA1c levels. The changes in insulin levels, and lipid profiles were similar for the two treatments. After the dapagliflozin treatment, body weight and homeostatic model assessment of insulin resistance (HOMA-IR) were decreased, while plasma ketone and β-hydroxybutyrate levels were increased (Table 2).
Changes in systemic endothelial function and renal injury markers
The primary endpoint was the change in the RHI after 8 weeks, although no significant changes or inter-group differences were observed after 8 weeks of dapagliflozin treatment or after 8 weeks of metformin treatment. In addition, no significant changes or inter-group differences were observed for serum nitrotyrosine, and endothelin-1 levels. Furthermore, no significant changes or inter-group differences were observed for the urine microalbumin/creatinine ratio, the β2-microglobulin/creatinine ratio, and GFR. However, the NAG levels were significantly higher after 8 weeks of dapagliflozin treatment, and the change in the NAG level was greater for dapagliflozin treatment (Table 2).
DISCUSSION
This randomized, open-label, crossover study revealed no significant changes in the RHI, endothelin-1, and nitrotyrosine levels after dapagliflozin and metformin treatment. However, dapagliflozin induced greater increases than metformin in the values for NAG, serum ketones, and β-hydroxybutyrate. Furthermore, dapagliflozin treatment improved HOMA-IR and body weight, while glycemic control was similar for both treatments.
The present study failed to detect significant changes or inter-group differences in endothelial function. Although endothelial dysfunction is considered an early step in atherosclerotic plaque formation, cardiovascular mortality curves from the Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG OUTCOME) study began diverging approximately 3 months after empagliflozin treatment, which is likely too early to be explained by an effect of de novo atherosclerosis on cardiovascular mortality [10]. It is also possible that our limited sample size and short treatment period hindered our ability to detect significant treatment-related changes in endothelial function. Nevertheless, the study period was not shorter than those of previous studies that have revealed changes in endothelial function within 8 weeks of treatment [111213].
Dapagliflozin induced a greater change in urine NAG than metformin in the present study. Urine NAG is an early marker for acute kidney injury originating from the proximal tubular cells [14] and has been suggested to predict diabetic nephropathy [15]. However, urine NAG has not been well-validated as a marker for drug-induced renal injury. One report indicated that urine NAG increased after sergliflozin treatment, which is an SGLT2 inhibitor with an O-glycan structure [16]. However, this effect was not reported for other SGLT2 inhibitors. Although urine NAG levels were increased after dapagliflozin treatment in the present study, the increase was not associated with concomitant changes in renal function such as serum creatinine and creatinine clearance, urine microalbumin, or β2-microglobumin. Therefore, the clinical relevance of changes in urine NAG levels requires further study to determine whether it is a temporary phenomenon that appears early during SGLT2 inhibitor treatment.
The RHI method in this study measures the digital pulse amplitude augmentation to quantify peripheral vasodilation potential via nitric oxide [1718] and is more reliable than the flow-mediated dilation method because it has less inter-personal variability and quantitatively evaluates the hyperemic response.
This is the first randomized clinical study to measure endothelial function during SGLT2 inhibitor treatment using the RHI method, which is a reliable method with low inter-personal variability. Cross-over study design could help minimize any effects of differences in the groups' baseline characteristics. Furthermore, the present study eliminated the effects of previous treatments by selecting drug-naïve patients. However, patients had relatively well controlled glucose levels and good endothelial function at baseline, which could minimize any treatment-related effects on endothelial function or renal injury markers. Also, the sample size and study duration might be insufficient to detect changes in endothelial function.
In conclusion, 8-week dapagliflozin treatment did not alter systemic endothelial function and renal injury markers, except urine NAG, and provided similar glycemic control to that of metformin.
 XML Download
XML Download