

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
High blood pressure is a leading cause of cardiovascular disease and mortality worldwide. In 2000, approximately one-fourth of the adult population had hypertension, and this number is estimated to increase by about 60% in 2025 [1]. In clinical practice, hypertension is frequently accompanied by other cardiovascular risk factors, including obesity, type 2 diabetes mellitus, and dyslipidemia [2].
Cardiovascular risk factors are often correlated, such that the presence of one often predicts the presence of others at present or in the future. For instance, African Americans and whites with high blood pressure were more likely to develop diabetes during a median 8.9-year follow-up period [3]. In addition, atherogenic dyslipidemia was associated with the development of hypertension in both men and women [456]. In the Women's Health Study population, there was a graded association between baseline non-high density lipoprotein (HDL) cholesterol level and risk for incident hypertension during over 10 years of follow-up; an inverse association was observed with baseline HDL cholesterol level [4]. In the Physician's Health Study population, men in the highest quintile of non-HDL cholesterol had a 39% higher risk of developing hypertension compared with those in the lowest quintile of non-HDL cholesterol and the highest quintile of HDL cholesterol had a 32% lower risk over a mean follow-up of 14.1 years [5].
Plasma HDL particles are inhomogeneous and consist of different sizes, densities, apolipoprotein composition, and lipid content [7]. Consequently, cardiovascular protective effects might differ according to HDL subclass. The majority of studies on cardiovascular disease risk have suggested that HDL2 is more protective than HDL3 [8]. However, little is known about the associations between different HDL cholesterol subclass and risk for future development of hypertension. Therefore, the aim of this study was to determine associations between HDL cholesterol subclasses, ratios of HDL cholesterol subclasses, and future development of hypertension.
METHODS
Study population
The study population consisted of Japanese American men and women enrolled in the Japanese American Community Diabetes Study, a cohort of second- (Nisei) and third-generation (Sansei) Japanese Americans of 100% Japanese ancestry. A detailed description of the selection and recruitment of study subjects has been published previously [9]. In brief, study participants were selected as volunteers from a community-wide comprehensive mailing list and telephone directory that included nearly 95% of the Japanese American population in King County, Washington. Among 658 subjects in the original cohort, 262 subjects were excluded because they had hypertension at baseline. Seventy-one subjects who did not complete follow-up examinations at 5 to 6 and/or 10 to 11 years after baseline examination were also excluded from this analysis. Additionally, 55 subjects were excluded due to one of the following: (1) computed tomography (CT) data to measure abdominal fat were not available at baseline (n=9); (2) taking lipid-lowering medications at baseline and/or at follow-up (n=52); or (3) plasma insulin was not available at baseline (n=3). Thus, a total of 270 subjects (130 men, 140 women) aged 34 to 75 years (mean age of 49.5 years) were enrolled in the analysis. The study received approval from the University of Washington Human Subjects Division, and written informed consent was obtained from all subjects (Institutional Review Board number: 34469).
Clinical and laboratory examination
All evaluations were performed at the General Clinical Research Center, University of Washington. A complete physical examination was performed at baseline. Personal medical history and lifestyle factors that possibly affect HDL cholesterol level, including cigarette smoking, alcohol consumption, and physical activity were determined using a standardized questionnaire. Smoking was classified into three groups (current smoker, past smoker, and never smoker). Alcohol consumption was measured in grams per week. The Paffenbarger physical activity index questionnaire was used to determine physical activity level (usual kilocalories expended weekly) [10]. Daily dietary sodium intake in milligrams was assessed from a food frequency questionnaire at baseline, as described previously [11].
Body mass index was calculated as weight in kilograms divided by the square of the height in meters. Waist circumference was measured at the level of the umbilicus. Blood pressure was measured with a mercury sphygmomanometer read to the nearest 2 mm Hg with subjects in a recumbent position. Systolic blood pressure was determined by the first perception of sound and diastolic blood pressure was determined at the disappearance of sounds (fifth-phase Korotkoff). Average blood pressure was calculated from the second and third of three consecutive measurements. Single 10-mm slice CT scans were performed at the abdomen to measure cross-sectional fat area (cm2), as described previously [12]. Visceral adipose tissue (VAT) and subcutaneous adipose tissue (SAT) areas were measured at the umbilicus level. Attenuation range for identification of fat was -250 to -50 Hounsfield units.
Biochemical measurements were performed at the time of sample collection using fresh samples as reported previously [13]. All blood samples were obtained following a 10-hour overnight fast. Plasma glucose was measured by the hexokinase method using an autoanalyzer (Department of Laboratory Medicine, University of Washington, Seattle, WA, USA). Plasma insulin was measured by radioimmunoassay (Diabetes Research Center, University of Washington, Seattle, WA, USA). To estimate insulin sensitivity, the homeostasis model assessment of insulin resistance (HOMA-IR) was used based on fasting glucose and insulin concentration [14]. Lipid measurements were performed according to modified procedures of the Lipid Research Clinics (Northwest Lipid Research Laboratory, Seattle, WA, USA). Total HDL cholesterol was determined in the supernatant after precipitation of apoB-containing lipoproteins with dextran sulfate. A second precipitation with high-molecular-weight dextran sulfate was performed on the supernatant containing HDL to separate HDL2 and HDL3 subclasses [1516].
Diabetes was defined by the presence of one of the following: (1) fasting glucose level ≥7.0 mmol/L; (2) treatment involving oral hypoglycemic agents or insulin therapy; (3) 2-hour post-glucose load ≥11.1 mmol/L; or (4) previous history of diabetes in the health interview [17]. Hypertension was defined as the presence of one of the following: (1) systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg; (2) taking antihypertensive medications; or (3) previous diagnosis of hypertension in the health interview [18]. The presence of cardiovascular disease was diagnosed by clinical history [19].
Statistical analyses
Data are expressed as mean±standard deviation (SD) or median (interquartile range) for continuous measures or as proportions for categorical variables. Differences between groups were tested by Student t-test or Mann-Whitney U test for continuous variables and the chi-square test or Fisher's exact test was used for categorical variables. Multiple logistic regression analysis with backward selection was used to determine whether plasma total HDL cholesterol and HDL cholesterol subclass were independently associated with incident hypertension. Odds ratios (ORs) with 95% confidence interval (CI) were calculated for independent variables included in logistic models, with a 1-SD increment used for OR calculations for continuous measurements. The presence of interaction was assessed in multivariate models by testing the significance of first order interaction terms. A variance inflation factor >4.0 was used as an indicator of multicollinearity. All statistical analyses were performed using PASW version 18.0 (SPSS Inc., Chicago, IL, USA). A P value of <0.05 was considered significant.
RESULTS
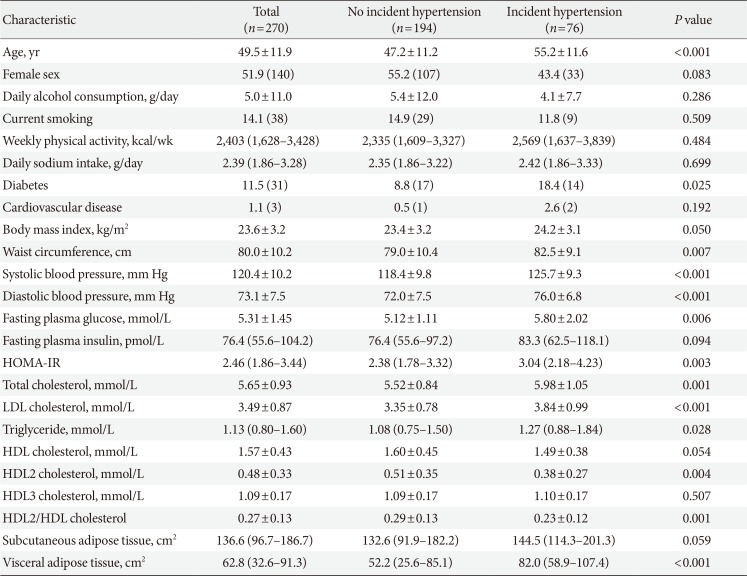
Over 10 years of follow-up, more than one-fourth of subjects without hypertension at baseline (28.1%, 76/270) developed hypertension. Table 1 shows the baseline characteristics of study subjects by incident hypertension. Mean age was 49.5 years and approximately half of the subjects were women. In terms of personal history possibly affecting plasma HDL cholesterol level, there were no differences in daily alcohol consumption, smoking status, and physical activity between the two groups. In addition, there was no difference in daily sodium intake at baseline between the two groups. Compared to subjects with incident hypertension, those who did not progress to hypertension showed a tendency to have higher levels of baseline total HDL cholesterol (P=0.054). In addition, baseline HDL2 cholesterol level was significantly higher in subjects who did not develop hypertension compared to those who did (0.51±0.35 mmol/L vs. 0.38±0.27 mmol/L, P=0.004, respectively); however, no difference was noted in baseline HDL3 cholesterol level between the two groups (P=0.507). In addition, the ratio of HDL2 to total HDL cholesterol was significantly higher in subjects who did not develop hypertension compared to those who did (0.29±0.13 vs. 0.23±0.12, P=0.001, respectively). Subjects who developed hypertension also have significantly greater mean VAT area, and a borderline significantly higher mean SAT area.
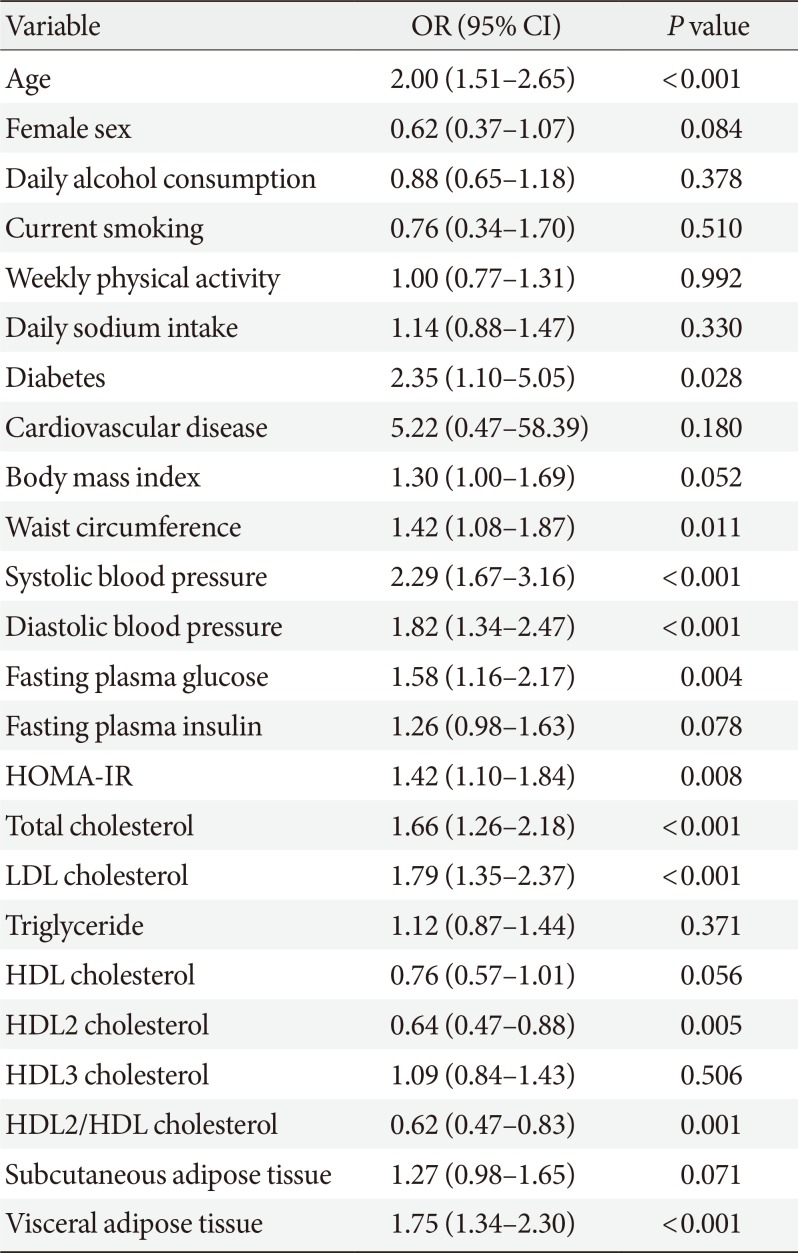
In univariate analysis, well-known risk factors for hypertension including age, waist circumference, baseline blood pressures, plasma glucose level, and HOMA-IR showed positive associations with the development of hypertension. In addition, presence of diabetes and greater VAT were associated with a higher risk for incident hypertension. Total cholesterol and low density lipoprotein (LDL) cholesterol levels were significantly and positively associated with future hypertension risk. Total HDL cholesterol was marginally associated with risk for incident hypertension, but this result was not statistically significant (OR per 1-SD increment, 0.76; 95% CI, 0.57 to 1.01; P=0.056). In contrast, HDL2 cholesterol (OR per 1-SD increment, 0.64; 95% CI, 0.47 to 0.88; P=0.005) was significantly and inversely associated with incident hypertension. No significant association was observed between HDL3 cholesterol (OR per 1-SD increment, 1.09; 95% CI, 0.84 to 1.43; P=0.506) and future hypertension risk (Table 2). Furthermore, HDL2/HDL cholesterol (OR per 1-SD increment, 0.62; 95% CI, 0.47 to 0.83; P=0.001) was associated with a lower risk for future hypertension, respectively. Other factors possibly affecting plasma HDL cholesterol level or hypertension risk, including alcohol consumption, smoking, physical activity, and daily sodium intake, did not show any association with the development of hypertension in this analysis.
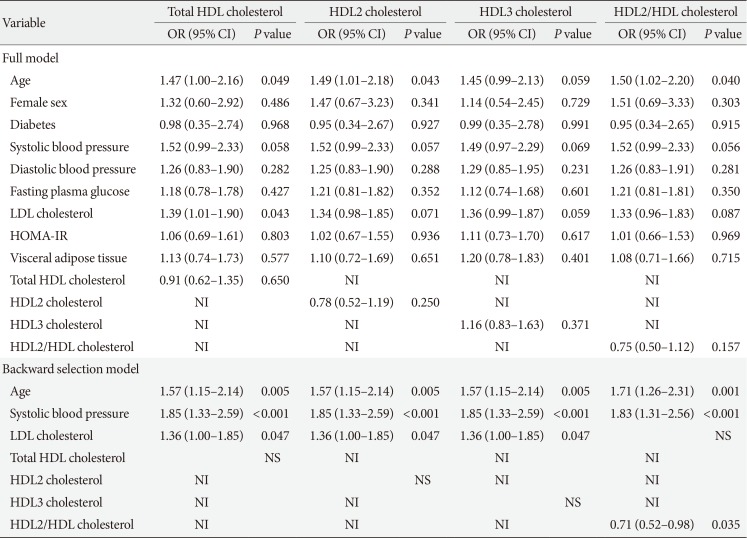
In multivariate analysis, model starting points for the backwards elimination algorithm included age, sex, baseline diabetes, fasting glucose level, HOMA-IR, systolic blood pressure, diastolic blood pressure, LDL cholesterol, and VAT area. HDL cholesterol, HDL2 cholesterol, and HDL3 cholesterol were included in each model based on univariate analysis. Waist circumference was excluded from this model because it causes multicollinearity with VAT. Total cholesterol and LDL cholesterol were highly correlated with one another, but only LDL cholesterol was chosen for inclusion in the model due to its higher OR in univariate analysis. After backwards elimination, only age (OR per 1-SD increment, 1.57; 95% CI, 1.15 to 2.14; P=0.005), baseline systolic blood pressure (OR per 1-SD increment, 1.85; 95% CI, 1.33 to 2.59; P<0.001), and LDL cholesterol level (OR per 1-SD increment, 1.36; 95% CI, 1.00 to 1.85; P=0.047) were independently associated with risk of future hypertension. However, neither total HDL cholesterol level nor any subclasses were independently associated with risk for incident hypertension (Table 3). No significant interactions were observed between sex and each of the independent variables in the multivariate model in predicting incident hypertension.
We next determined whether the ratio of HDL2 to total HDL cholesterol is associated with risk for future hypertension. The full model is shown using the same methodology as employed in Table 3. After backwards elimination, age and baseline systolic blood pressure were independently associated with incident hypertension. In addition, HDL2/HDL cholesterol ratio (OR per 1-SD increment, 0.71; 95% CI, 0.52 to 0.98; P=0.035) was inversely associated with incident hypertension, independent of age and baseline systolic blood pressure (Table 3).
DISCUSSION
In the current prospective study performed in Japanese American men and women, subjects who developed incident hypertension had lower baseline HDL2 cholesterol level compared with subjects who did not develop hypertension. In addition, subjects with a higher proportion of HDL2 cholesterol among total HDL cholesterol were associated with lower risk of future development of hypertension independent of age, sex, baseline diabetes, fasting glucose, HOMA-IR, LDL cholesterol, VAT, and even systolic and diastolic blood pressure. These results argue for HDL2 as the most important subclass of HDL in the prediction of future hypertension.
Our results agree in part with those of previous studies [456]. Results from these studies consistently demonstrated that higher baseline HDL cholesterol level is independently associated with lower risk of incident hypertension. However, to the best of our knowledge, there has been only one prospective study showing the association between HDL subclass and incident hypertension [20]. The study participants were recruited from the Women's Health Study population and followed up for 8 years. In this study, higher HDL cholesterol was associated with lower risk of incident hypertension. However, risk for incident hypertension differed with HDL particle size determined by nuclear magnetic resonance spectroscopy. Small and medium HDL particles, which constitute most of the total HDL particles, were associated with higher risk for incident hypertension whereas large HDL particles were protective against the development of hypertension even after adjusting for biomarkers of inflammation/endothelial function, hyperglycemia, and nonlipid risk factors. In addition, the addition of particle subclass resulted in better prediction for incident hypertension than a model with traditional lipids and risk factors. The results partly agree with our observation that measurement of HDL cholesterol subclass had additional benefits over total HDL cholesterol level in predicting future hypertension risk. The proportion of specific HDL cholesterol subclasses among total HDL cholesterol is more important than total HDL cholesterol level in determining future hypertension risk. That is, a higher proportion of large HDL2 cholesterol among total HDL cholesterol was inversely associated with hypertension risk. However, our current study differs from the aforementioned studies [45620] in showing associations between HDL cholesterol and/or HDL subclass and incident hypertension risk due to the following. First, all these studies included either men or women, and it is uncertain whether the results are applicable to both sexes. Our study was performed in both men and women together and no significant interactions were observed between sex and HDL cholesterol, HDL cholesterol subclass, and their ratios. Therefore, our results can be generalized to both sexes. Second, in the Women's Health Study [420] and Physicians' Health Study [5], baseline and incident hypertension were ascertained based on self-reported hypertension status. In our study, blood pressure was measured using a standardized protocol with a mercury sphygmomanometer and average blood pressure was calculated from the second and third of three consecutive measurements. Third, in addition to conventional risk factors for hypertension, we further adjusted for VAT area, a strong predictor for incident hypertension in our previous studies [2122].
Diverse mechanisms for the relationship between HDL cholesterol subclass and incident hypertension are possible. First, insulin resistance is a key pathophysiologic mechanism underlying the clustering of multiple cardiovascular risk factors including glucose intolerance, high blood pressure, and dyslipidemia [2]. Insulin sensitivity determined by the glucose disposal rate during the hyperinsulinemic-euglycemic clamp was positively correlated with HDL particle size. In addition, when study subjects were divided into insulin sensitive, insulin resistant, and diabetes groups, large HDL progressively decreased combined with an increase in small HDL; however, no significant difference in HDL cholesterol level was noted [23]. In the current study, adjustment for HOMA-IR, a surrogate measure of insulin resistance, and VAT, a determinant of insulin resistance, did not affect the association between HDL cholesterol subclass and incident hypertension. Thus, insulin resistance appears to play a partial or limited role in the association between HDL subclass and incident hypertension. Second, interaction between the renin-angiotensin system and dyslipidemia has been reported [24]. It was suggested that the vascular protective effect of HDL mediates downregulation of upregulated angiotensin II type 1 receptor under diabetic conditions [25]. In a study performed in young patients with high normal blood pressure, incident hypertension was more common in patients with elevated serum cholesterol compared to patients with normal cholesterol level. In particular, high plasma renin activity increased the risk of hypertension in subjects with both high cholesterol level and normal cholesterol level. The authors concluded that hypercholesterolemia can elevate blood pressure by affecting the circulating renin angiotensin system in patients with high normal blood pressure [26]. Third, in addition to reverse cholesterol transport, HDL has diverse cardioprotective properties, including anti-oxidation, anti-thrombotic properties, anti-inflammation, and improved endothelial function [27]. These diverse effects on vessels may reduce blood pressure [27].
In the current study, total HDL cholesterol had limited value for predicting future development of hypertension. Similar to our results, baseline HDL cholesterol levels were similar between subjects who remained normotensive and subjects who progressed to hypertension during 8 years of follow-up in the Strong Heart Study [28]. In a population-based cohort study from Iran, HDL cholesterol level was not predictive of incident hypertension in both crude and adjusted models after 7 years of follow-up [29]. However, our results showed that specific HDL cholesterol subclasses, particularly expressed as the ratio of subclass to total HDL cholesterol, provided additional information and had clinical relevance in predicting future risk for incident hypertension. In addition to predicting incident hypertension, measurement of HDL cholesterol subclass might be useful in predicting diverse cardiometabolic risk factors. First, in our previous study with the same cohort, HDL2 cholesterol level was more strongly associated with lower incidence of type 2 diabetes mellitus than total HDL cholesterol level [16]. Second, in 1,155 Japanese subjects, the HDL2/HDL3 cholesterol ratio was inversely associated with HOMA-IR and positively associated with high-molecular-weight adiponectin level. As the number of metabolic syndrome components increased, the ratio gradually decreased [30]. Third, liver fat determined by magnetic resonance spectroscopy was more strongly correlated with HDL2 cholesterol and HDL2-to-HDL3 cholesterol than total HDL cholesterol [31]. Collectively, these studies suggest that HDL cholesterol subclasses and their ratios can be used to predict a variety of cardiometabolic risk factors and phenotypes more accurately than simple total HDL cholesterol level.
Our study has some limitations. First, our population was relatively small (270 subjects). Second, study participants were 100% Japanese American, and the results may not be generalizable to other ethnic groups. It is possible that HDL cholesterol subclasses have different associations with incident hypertension among different ethnic groups. Third, the analytic method used to measure HDL cholesterol and HDL subclass has evolved in recent years. Methodological differences may explain, at least in part, the inconsistent association between HDL subclass and cardiovascular disease [7]. In this study, HDL cholesterol subclass was determined using a differential precipitation method; however, good agreement between HDL subclass measured by dextran precipitation and preparative ultracentrifugation for HDL2 [32] and a novel homogeneous assay for HDL3 [33] were reported. Lastly, HDL cholesterol level may change over time; however, we did not investigate the association between changes in total HDL cholesterol and subclasses and future hypertension risk.
In summary, the measurement of total HDL cholesterol concentration alone had a limited clinical usefulness for predicting future hypertension risk in this Japanese American population. On the other hand, HDL cholesterol subclass provided additional information compared to total HDL cholesterol in predicting the risk of incident hypertension. In particular, a higher proportion of HDL2 cholesterol among total HDL cholesterol was independently associated with a lower risk for incident hypertension during 10 years of follow-up.
 XML Download
XML Download