

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In several cross-sectional studies and a longitudinal study, increased value of baseline serum albumin was positively associated with metabolic syndrome (MetS) prevalence or incidence [123]. Over-nutrition, as indicated by elevated serum albumin level, has been suggested as one of the elucidation [124]. However, serum albumin, which is also a negative acute-phase protein, has been reported to drop during chronic inflammation [356]. In a cross-sectional study, elevated serum albumin level, which was positively linked to the prevalence of MetS, was associated with decreased prevalence of carotid plaques [1]. Also, in another study, high serum albumin concentrations were linked to increased odds ratios for MetS, whereas low albumin levels were associated with increased prevalence of inflammation, which was defined as a C-reactive protein level of 0.4 mg/dL or more [2].
Serum uric acid level has been consistently reported as a predictor of incident MetS [789]. Also, it has been reported that hyperuricemia can lead to endothelial dysfunction and low-grade inflammation by impaired nitric oxide production [91011].
Although there have been studies to clarify the relationship between MetS and serum albumin or uric acid level, the association of MetS incidence in combination with uric acid and albumin concentrations has not yet been analyzed. Moreover, the association between elevated serum albumin and the risk of MetS may be diminished in hyperuricemic subjects by the chronic low-grade inflammation associated with hyperuricemia. Therefore, we aimed to explore the association of baseline serum albumin and uric acid levels with the risk of incident MetS in subgroups determined by the levels of these two parameters.
METHODS
Study population and design
This was a retrospective longitudinal study of participants who had undergone annual health check-up programs at least four times at the Health Promotion Center of Samsung Medical Center between 2006 and 2012. Among 24,185 subjects who received yearly check-ups for 4 or more years, those with missing waist circumference (WC) measures, those who had MetS at baseline, those who were diagnosed with MetS at the first follow-up visit, and those with jaundice, hepatitis B or C, abnormal liver function test results, or decreased renal function were excluded. The exclusion criteria and process of enrollment and exclusion were described in more detail in our previous report [12]. Finally, 11,613 individuals (6,890 men and 4,723 women) with a mean age of 50.9 years (range, 18 to 89 years) were enrolled. They were observed till the development of incident MetS. If they were not diagnosed with MetS until the final visit, the last visit was considered to be the end of follow-up. This study was approved by the Institutional Review Board (IRB) of Samsung Medical Center (IRB File number; SMC 2017-07-141-001) and was conducted in accordance with the Declaration of Helsinki. An exemption from informed consent was granted by the board because all data were analyzed anonymously.
Clinical and biochemical measurements
During check-ups, surveys on medical history, smoking status, and alcohol history were carried out. Anthropometric measurements and laboratory tests were also performed. With regard to smoking status, subjects were classified as never, past, or current smokers. Participants were required to answer questionnaires regarding whether they take statins or not, and whether they take aspirin or not. They were dichotomously categorized as drinkers and non-drinkers according to their answer to the questionnaire, which asked whether they drink alcohol or not; patients were categorized in this way since data on the amount or frequency of alcohol consumption were not available. Note that even this dichotomous information was not available in 2,130 subjects (1,347 men and 783 women). Blood pressure (BP) was measured by trained nurses with mercury sphygmomanometers on the patients' right arms after at least 5 minutes of rest. WC was defined as the circumferential measure at the midpoint between the costal margin and iliac crest at the end of expiration in the erect position. Body mass index (BMI) was derived from body weight in kilograms divided by height in meters squared (kg/m2). The Modification of Diet in Renal Disease (MDRD) equation [13] was utilized to calculate estimated glomerular filtration rate (eGFR). The homeostatic model assessment index 2 for insulin resistance (HOMA2-IR), which reflects insulin resistance, was determined by the HOMA calculator (http://www.dtu.ox.ac.uk) [14].
Venous blood samples were drawn after an overnight fast. Serum albumin level was derived using bromocresol green and a Roche modular DP analyzer (Roche Diagnostics, Basel, Switzerland). Fasting high density lipoprotein cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C), triglycerides (TGs), and serum uric acid were measured using the enzymatic colorimetric method with a Modular D2400 (Roche Diagnostics). The hexokinase method with Bayer Reagent Packs on an automated chemistry analyzer (Advia 1650 Autoanalyzer; Bayer Diagnostics, Leverkusen, Germany) was utilized to measure plasma glucose levels. Plasma insulin values were determined using an immunoradiometric assay (DIAsource Co., Louvain-la-Neuve, Belgium). However, in 4,705 participants (2,352 men and 2,353 women), plasma insulin levels were not obtained.
Definition
The 2005 revision of the National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III) criteria, with Asian-specific cut-off values for abdominal obesity (WC ≥90 cm in men, ≥80 cm in women) were used to define MetS [1516].
The serum uric acid value was stratified into lower (L) and higher (H) levels by the sex-specific medians of the study population. Serum albumin was also categorized into two binary variables (L and H) at cut-off points of sex-specific median values. Four groups (group 1 to 4) were established according to the binary category of serum albumin and uric acid (serum albumin L, serum uric acid L; serum albumin H, serum uric acid L; serum albumin L, serum uric acid H; serum albumin H, serum uric acid H).
Statistical analyses
The SPSS software version 23 (IBM Co., Armonk, NY, USA) was used for statistical analyses. Continuous variables with normal distributions were presented as the mean±standard deviation, while continuous variables with non-normal distributions were expressed as the median and interquartile ranges. Categorical data were presented as the frequency and percentage. One-way analysis of variance (ANOVA) and Tukey's multiple comparison were utilized for continuous variables with normal distributions. The Kruskal-Wallis test followed by the post hoc Mann-Whitey U test using the Bonferroni correction was applied for continuous variables with non-normal distributions to assess baseline characteristics of the study population according to the four groups set by the sex-specific medians of serum albumin and uric acid at initial visit. For categorical variables, Pearson's chi-square test was performed.
Pearson's correlation analyses between serum uric acid and parameters associated with MetS were performed, and these results were compared to those between serum albumin and the same variables. Scatter plots were used to visually express these correlations.
Multivariate Cox regression analysis was conducted to evaluate the hazard ratios (HRs) and 95% confidence intervals (CIs) for MetS incidence according to the four groups stratified by the sex-specific medians of baseline serum albumin and uric acid. Cox regression models were adjusted for potential confounders including age, BMI, WC, systolic BP, alanine aminotransferase (ALT), eGFR, fasting glucose, smoking status, whether taking aspirin or statins, the presence of baseline diabetes mellitus, LDL-C, and high-sensitivity C-reactive protein (hs-CRP). Also, in those with corresponding information, additional adjustment for alcohol history (n=9,483) or HOMA2-IR was applied. Two-tailed probability values less than 0.05 were considered to be statistically significant.
RESULTS
Characteristics of the study population according to four groups stratified by serum albumin and uric acid category
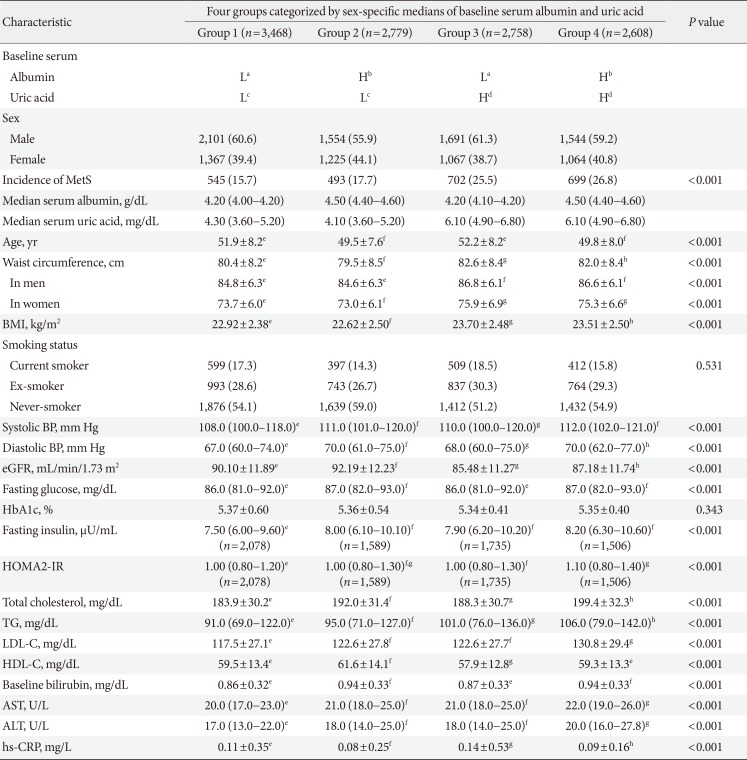
During 55,407 person-years of follow-up (a mean follow-up of 4.8±1.3 years), 2,439 cases (1,695 in men and 744 in women) of incident MetS developed (21.0% in all subjects; 24.6% in men and 15.8% in women). The baseline clinical characteristics and laboratory data of the study participants according to four groups categorized by the sex-specific medians of serum albumin and uric acid are presented in Table 1. The sex-specific median of the serum uric acid level was 5.8 mg/dL in men and 4.1 mg/dL in women, while that of the serum albumin level was 4.3 g/dL in men and 4.2 g/dL in women. These values were used as cut-off points to categorize the groups. Subjects in group 3 (serum albumin L and serum uric acid H) and group 4 (serum albumin H and serum uric acid H) had higher WC, BMI, hs-CRP, total cholesterol, TG, LDL-C, aspartate aminotransferase (AST), and ALT values than those who were in group 1 (serum albumin L and serum uric acid L) and group 2 (serum albumin H and serum uric acid L), respectively. HDL-C and eGFR levels were significantly lower in group 3 (serum albumin L and serum uric acid H) compared to those in group 1 (serum albumin L and serum uric acid L). They were also lower in group 4 (serum albumin H and serum uric acid H) compared to those in group 2 (serum albumin H and serum uric acid L). Total cholesterol, TG, LDL-C, AST, and ALT levels were significantly higher in group 2 (serum albumin H and serum uric acid L) than in group 1 (serum albumin L and serum uric acid L). Also, they were significantly higher in group 4 (serum albumin H and serum uric acid H) compared to those in group 3 (serum albumin L and serum uric acid H). On the other hand, in the same category of baseline uric acid level, hs-CRP was significantly lower in groups with increased albumin category (serum albumin H).
Correlations between serum albumin, serum uric acid, and other parameters
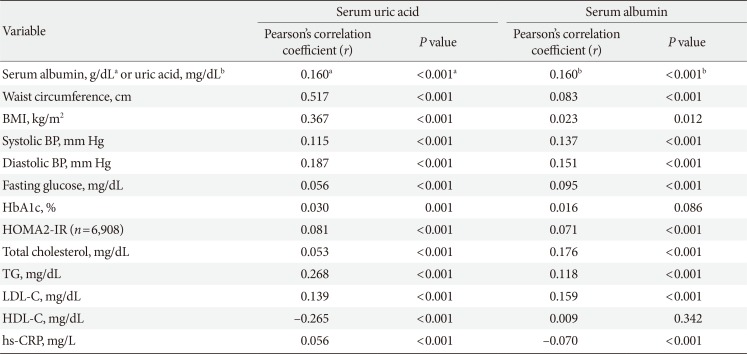
Correlations between baseline serum albumin or uric acid and parameters including MetS components, hs-CRP and BMI were calculated (Table 2 and Supplementary Fig. 1). Although both uric acid and albumin were positively correlated with WC, BMI, and TG, uric acid showed stronger correlations than albumin did. Fasting glucose, glycosylated hemoglobin, and HOMA2-IR (n=6,908) showed a weak positive correlation with serum uric acid and albumin. HDL-C was negatively correlated only with uric acid, and no significant correlation between HDL-C and serum albumin level was observed. There was an inverse correlation between serum albumin concentration and hs-CRP level while uric acid level was positively correlated with hs-CRP.
Metabolic syndrome incidence according to serum albumin and uric acid categories
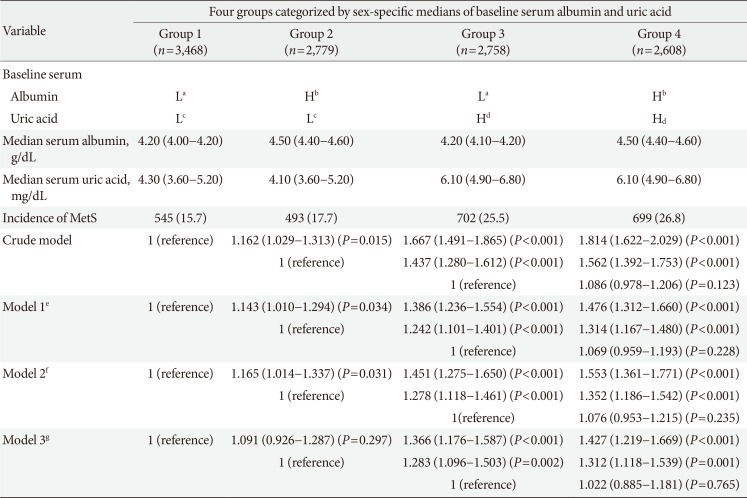
The incidence of MetS was calculated separately in four groups divided by the sex-specific medians of serum albumin and uric acid (Table 3). In the same category of baseline albumin level, the incidence of MetS increased as the serum uric acid category advanced. The HR for incident MetS in group 3 (serum albumin L and serum uric acid H) was 1.386 (95% CI, 1.236 to 1.554), compared to group 1 (serum albumin L and serum uric acid L) after fully-adjusting for possible confounding factors (model 1). In group 4 (serum albumin H and serum uric acid H), the HR was 1.314 (95% CI, 1.167 to 1.480) compared to group 2 (serum albumin H and serum uric acid L).
However, the incidence of MetS increased significantly with the increased albumin category only in subjects with uric acid concentrations of sex-specific medians or less. The HR for MetS incidence in the fully adjusted model (model 1) was 1.143 (95% CI, 1.010 to 1.294) in group 2 (serum albumin H and serum uric acid L) compared to group 1 (serum albumin L and serum uric acid L). However, even this statistical significance was not present when the model was additionally adjusted for HOMA2-IR in the subgroup with fasting insulin measurements (model 3 in Table 3).
The HR for incident MetS in the group with higher uric acid and lower albumin (group 3) was 1.242 (95% CI, 1.101 to 1.401) compared to the group with higher albumin and lower uric acid (group 2).
DISCUSSION
To the best of our knowledge, this was the first study to analyze the association of MetS incidence considering both uric acid and albumin levels. This longitudinal study demonstrated that higher levels of serum albumin were associated with increased risk of incident MetS only in individuals in the lower uric acid category. On the contrary, elevated serum uric acid concentration was positively linked to risk of incident MetS regardless of the category of serum albumin level.
When HOMA2-IR was included as a potential confounding factor, the increased albumin category was not associated with higher MetS incidence even in subjects with uric acid levels of sex-specific medians or less, suggesting that the effect of serum albumin concentration on MetS incidence may be mediated by insulin resistance, as indicated by HOMA2-IR. In a previous report, serum albumin concentration was associated with HOMA-IR value above the highest quartiles [17]. Further, in our study, HOMA2-IR showed a weak positive correlation with serum albumin concentration. Insulin resistance, as indicated by the high levels of HOMA-IR, is directly linked to compensatory hyperinsulinemia [1718], which is a predisposing condition for the development of MetS [17].
Our results suggest that baseline serum uric acid concentration may be a useful marker for predicting the development of MetS regardless of serum albumin level, whereas the usefulness of serum albumin concentration may by diminished by certain conditions associated with hyperuricemia. For this reason, when considered separately, serum uric acid rather than serum albumin level may be a more helpful marker in predicting the incidence of MetS. In our study, both serum albumin and uric acid were positively correlated with WC, BMI, and TG. However, uric acid was more strongly correlated with these parameters than albumin. Moreover, only serum uric acid, not albumin, showed a significant negative correlation with HDL-C. In addition, only uric acid concentration was positively correlated to hs-CRP level, which may be reflective of the chronic inflammation, which is known to play an important role in the initiation and advancement of MetS [1219]. In our data, the risk of incident MetS in subjects with higher uric acid and lower albumin category was significantly higher than that in individuals with higher albumin and lower uric acid category.
The usefulness of albumin as a predictor of MetS incidence was decreased in groups with higher uric acid category. Although the mechanism cannot be determined based on this study because of its retrospective design, changes in albumin levels in chronic low-grade inflammation associated with hyperuricemia may be involved. Serum albumin levels can be affected by the nutritional status as a nutritional marker [12]. In several cross sectional studies, high serum albumin level has been related to parameters indicative of over-nutrition, such as obesity and MetS [1234]. However, at the same time, serum albumin concentration is influenced by inflammation [2356]. Albumin is a well-known negative acute-phase protein [56], and its level also decreases during chronic inflammation [35]. Hyperuricemia has been reported to induce endothelial dysfunction and low-grade inflammation through inhibition of nitric oxide production and generation of reactive oxygen species [91011]. In accordance with these reports, in our data, uric acid concentration showed a significant positive correlation with hs-CRP level while serum albumin level was inversely correlated with hs-CRP. Increased levels of serum albumin may reflect over-nutritional status in the body, and this can provide an explanation for the association of elevated serum albumin level with risk of MetS. However, in the chronic inflammatory situation associated with hyperuricemia, even in the over-nutrition state, the albumin level may decrease due to inflammation, which may reduce the usefulness of albumin as an indicator of over-nutrition and as a marker in predicting incident MetS.
Our study has several limitations. First, participants in our study were self-selected through voluntary annual health check-ups for four or more times at a single center. These subjects might not represent the general Korean population, and the possibility of selection bias cannot be excluded. In addition, information on drugs known to affect the level of serum uric acid, such as allopurinol and diuretics, and lifestyle factors such as diet and exercise were not collected. Moreover, the retrospective design of this study may limit the clarification of causal relationships and underlying mechanisms.
Although higher serum uric acid level was associated with risk of incident MetS regardless of serum albumin value, elevated serum albumin concentration was positively linked to MetS incidence only in individuals with lower uric acid level in a healthy Korean population. This may be due to a decrease in serum albumin concentration in chronic inflammatory conditions associated with hyperuricemia, which may inhibit the role of albumin as an indicator of over-nutrition and as a predictor of incident MetS. Therefore, when considered individually, serum uric acid may be a more useful single marker in predicting the development of MetS compared to serum albumin. Further studies are needed to confirm these suggestions.
 XML Download
XML Download