

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Type 2 diabetes mellitus (T2DM) is one of the most common metabolic disorders in the world, increasing in prevalence with age [1]. Muscle mass gradually decreases with age after the fourth decade of life, even if body weight or body fat mass is unchanged or slightly increased [2]. Skeletal muscle is a major site for glucose uptake and deposition, and hence plays an important role in the regulation of blood glucose levels [3]. Therefore, low muscle mass may affect the development of insulin resistance and T2DM.
Although a few cross-sectional studies support an inverse association between muscle mass and insulin resistance or T2DM prevalence [456], other studies have failed to show this [789]. In a recent cross-sectional study, thigh muscle area directly measured by computed tomography (CT) was negatively associated with T2DM in South Asians but not Europeans, suggesting the possibility of ethnic differences in this relationship [8]. To our knowledge, no longitudinal research exists on the association between thigh muscle area and change in insulin resistance.
There are three prospective investigations that have examined the association between muscle mass and incident T2DM with conflicting results. First, overall muscle mass measured by dual-energy X-ray absorptiometry was not a risk factor for incident T2DM in an Australian community-dwelling cohort of men with 5-year follow-up in the Men Androgen Inflammation Lifestyle Environment and Stress study [10]. In the Health ABC study of white and black participants ages 70 to 79 years, no association was observed between abdominal and thigh muscle area measured by CT and incident T2DM [11]. However, there was a significant interaction with body mass index (BMI) for muscle mass in women, so that greater abdominal but not thigh muscle area predicted lower risk of incident T2DM for normal-weight women only, whereas higher thigh muscle mass was associated with greater risk of incident T2DM for overweight/obese women in adjusted models. On the contrary, Son et al. [12] reported low overall muscle mass was associated with a higher risk of T2DM in Korean adults using bioelectrical impedance for muscle measurement. These previous prospective studies have limitations, such as inclusion of male or elderly participants only, self-reported diagnosis of diabetes, and use of bioelectrical impedance, the accuracy of which can be affected by hydration status, age, medical conditions affecting fluid and electrolyte balance, and other factors [13].
The aim of this study was therefore to investigate the association of thigh muscle mass measured by CT imaging with insulin sensitivity and incident T2DM over a 10-year follow-up in a Japanese American cohort of men and women. We also examined whether generalized adiposity as reflected by BMI modifies the association between thigh muscle mass and incident T2DM.
METHODS
Study subjects
The study received approval from the University of Washington Human Subjects Division and all subjects provided written informed consent (Institutional Review Board number: 34469). Study subjects were from the Japanese American Community Diabetes Study, a cohort of second- and third-generation Japanese Americans of 100% Japanese ancestry. Details of the selection and recruitment of the study subjects have been described previously [14]. Briefly, study participants were selected as volunteers from a community-wide comprehensive mailing list and telephone directory that included almost 95% of the Japanese American population in King County, WA, USA. Participants had follow-up visits 10 to 11 years after the baseline study visit. Among 658 subjects in the original cohort, 166 were excluded because they had diabetes at baseline. Additionally, we excluded 12 subjects who did not have CT measurements of thigh muscle at baseline and 81 subjects who did not complete follow-up examinations. Thus, a total of 399 subjects without diabetes mellitus at baseline were available for analysis.
Clinical and laboratory examination
Personal medical history and lifestyle factors were determined using a standardized questionnaire. Family history of diabetes was considered positive if any first-degree relative had diabetes. Smoking status was divided into two categories (current smoker, former/never smoker). Moderate alcohol consumption was defined as intake of more than 6 g of ethanol per day [15]. Physical activity level was estimated by the Paffenbarger physical activity index questionnaire (usual kilocalories spent weekly) [16], and regular physical activity was defined as more than moderate intensity physical activity.
Blood samples were obtained after an overnight fast of at least 10 hours. Insulin sensitivity was estimated by homeostasis model assessment of insulin resistance (HOMA-IR) index calculated as [fasting serum insulin (µU/mL)×fasting serum glucose (mg/dL)]/405 [17] and the quantitative insulin sensitivity check index (QUICKI) [18]. Diabetes was diagnosed by 75-g oral glucose tolerance test (OGTT), fasting glucose level ≥126 mg/dL or 2-hour post-glucose load ≥200 mg/day, or by treatment with oral glucose-lowering agents or insulin [19].
A single (1-cm) CT scan slice was obtained of the left thigh at a level halfway between the greater trochanter and the superior margin of the patella and the abdomen at the level of the umbilicus [20]. CT scans were analyzed using density contour software. Tissue with a density of −250 to −50 Hounsfield units (HU) was classified as adipose tissue [20]. Total thigh and thigh subcutaneous fat cross-sectional areas (cm2) were measured and thigh muscle mass was estimated by calculating the difference between total thigh area and thigh subcutaneous fat area because directly measured thigh muscle area was unavailable. This proxy measure of thigh muscle area has been shown to be highly correlated with directly measured thigh muscle area in a validation study conducted in a Korean population (r=0.98; 95% confidence interval, 0.88 to 1.00) [21].
Statistical analysis
Continuous variables are expressed as mean±standard deviation, and categorical variables are expressed as numbers and percentages. The distribution of HOMA-IR was skewed and was therefore normalized using a logarithmic transformation for all analyses. An independent t-test was used to compare differences between means for continuous variables, and the chi-square test was used for categorical data. Multiple linear regression analysis was used to determine independent associations between insulin sensitivity at 10 years in relation to baseline thigh muscle mass area. Logistic regression analyses were conducted to estimate the associations between thigh muscle mass area and incident T2DM while adjusting for covariates. Interactions by BMI and sex with thigh muscle mass in relation to incident T2DM was assessed by insertion of first-order interaction terms into the logistic model. The data were analyzed using IBM SPSS Statistics for Windows version 22.0 (IBM Co., Armonk, NY, USA) and Stata version 14.2 (StataCorp, College station, TX, USA). A two-sided P<0.05 was considered to indicate statistical significance.
RESULTS
Baseline clinical characteristics
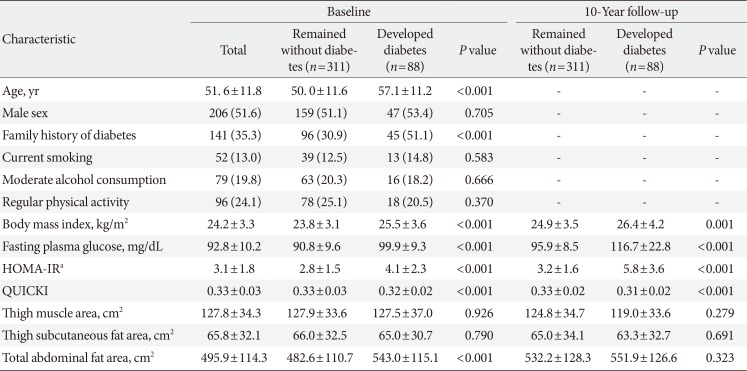
At baseline, study participants had a mean age of 51.6 years, 51.5% were men and they had a mean BMI of 24.2 kg/m2 (Table 1). Over a 10-year follow-up period, 88 of the 399 participants (22.1%) developed T2DM. Those developing incident T2DM were older, had higher BMI, fasting plasma glucose, HOMA-IR, QUICKI, total abdominal fat area, and a higher prevalence of a family history of diabetes compared to those who remained nondiabetic.
The association between thigh muscle area and insulin resistance
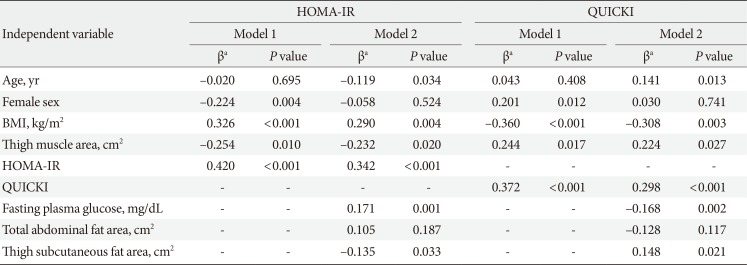
Table 2 lists the association of baseline thigh muscle area with HOMA-IR and QUICKI at 10-year follow-up. Thigh muscle area was inversely associated with future HOMA-IR after adjustment for age, sex, BMI, and baseline HOMA-IR (Model 1). This association persisted after further adjustment for fasting plasma glucose, total abdominal fat area, and thigh subcutaneous fat area (Model 2). In addition, thigh muscle area was independently associated with QUICKI as another insulin sensitivity surrogate index.
The association between thigh muscle area and incident T2DM
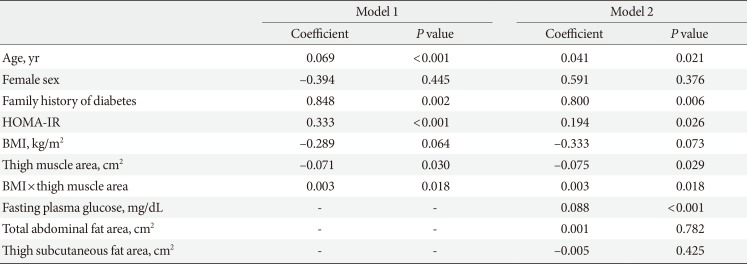
When we investigated the association between thigh muscle area and incident T2DM in multivariate logistic regression analysis, there was no significant association between thigh muscle area and incident T2DM after adjustment for age, sex, BMI, family history of diabetes, and HOMA-IR. However, when we examined an interaction between BMI and thigh muscle area using the first-order interaction terms inserted into the same logistic model, there was a significant positive interaction between BMI and estimated thigh muscle area (interaction term coefficient 0.003, P=0.022), with the coefficient for thigh muscle having a negative sign and being statistically significant (−0.071; P=0.030) (Table 3, model 1). In addition, interaction between BMI and thigh muscle area remained significant after insertion of fasting plasma glucose, total abdominal fat area, and thigh subcutaneous fat area as additional covariates into the model of Table 3 (model 2). There was no significant interaction between sex and thigh muscle (interaction term coefficient, −0.024; P=0.159) when these interactions were inserted into the logistic model in Table 3.
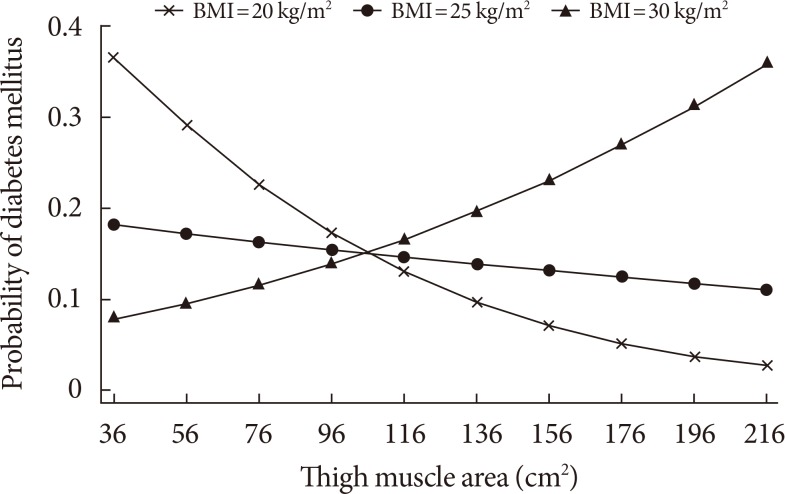
In Fig. 1, the calculated probability of incident T2DM from the logistic regression model from Table 3 that includes the thigh muscle×BMI interaction is shown across the range of thigh muscle area for three values of BMI, demonstrating that the protective effect exists for lower levels of BMI but disappears in the obese range (BMI=30 kg/m2).
DISCUSSION
These prospective data demonstrate that baseline thigh muscle mass area was inversely associated with future insulin resistance. We also observed an interaction between thigh muscle area and BMI in relation to T2DM. Namely, greater thigh muscle area was associated with lower risk of incident T2DM over 10 years for leaner subjects independent of age, sex, family history of diabetes, HOMA-IR, fasting plasma glucose, total abdominal fat area, and thigh subcutaneous fat area at baseline. We observed an inverse association between thigh muscle area and HOMA-IR change over 10 years that did not significantly vary by BMI. Thus greater muscle area was associated with less insulin resistance after 10 years but not a lower risk of T2DM in the presence of greater general adiposity. The potential benefit of less insulin resistance in association with greater muscle area may be overridden by higher general adiposity with regard to future T2DM risk.
Previous studies reported that lower body muscle such as leg muscle was more associated with insulin resistance than was upper body muscle [2223]. Furthermore, the rate of loss of lower limb muscle was more than twice the rate of loss of upper limb muscle with aging [22425]. Considering these characteristics and their large muscle content, preservation of leg muscles should be considered as a main target in the strategy to prevent insulin resistance and incident T2DM. However, there has been little prospective research on this topic.
We found that low thigh muscle area is independently associated with greater insulin resistance after 10 years in relatively healthy middle-aged and older Japanese Americans. To our knowledge, this is the first longitudinal study showing the long term association between thigh muscle mass and future insulin resistance. These findings support a previous cross-sectional study that demonstrated an inverse association between muscle mass and insulin resistance [4].
The association between baseline thigh muscle area and incident T2DM was modified by BMI in our cohort; that is, greater thigh muscle area predicted lower risk of incident T2DM among leaner participants. The association between thigh muscle area and T2DM risk was diminished at higher levels of BMI. Our findings thus support earlier findings from cross-sectional studies. Although measurement of lower limb circumferences is a simple method to reflect both leg muscle and fat mass, there was also a strong interaction between thigh circumference and obesity in relation to diabetes prevalence in a large-scale, cross-sectional study [26]. Smaller thigh circumference was associated with diabetes, but this association was stronger among non-obese individuals. This study, though, could not convincingly demonstrate an association between thigh muscle and diabetes risk due to its cross-sectional design, which prevents ascertainment of temporal sequence, and also its measurement of thigh circumference which reflects a combination of thigh fat and muscle mass. In another cross-sectional study of postmenopausal women that also suggested an association between greater muscle mass and lower T2DM prevalence, abdominal muscle area was inversely related with T2DM prevalence, especially for women with a BMI <25 kg/m2 [5].
To our knowledge the current study extends findings of the only other investigation that assessed risk of incident T2DM by regional muscle mass area using imaging (Health ABC Study), and which was conducted in an elderly Caucasian and African American population [10]. Ethnicity is an important determinant of body composition, with Asians known to have less muscle mass and more body fat compared to Western populations at the same BMI [27]. These characteristics are related with a higher risk of insulin resistance and T2DM [2829]. In addition, our population with a mean age of 51.6 years was relatively younger than those of the Health ABC Study, so our findings reflect the impact of a relatively higher range of muscle mass on the development of T2DM before advanced age-related sarcopenia. In addition, we used the OGTT along with a history of clinical diagnosis for identifying incident T2DM, and therefore were more likely to detect its occurrence as compared to the Health ABC Study that relied on fasting glucose and clinical history only [30].
We previously found that BMI acts as an effect modifier in the relationship between hand grip strength and incident T2DM in Japanese Americans, i.e., greater hand grip strength predicts a lower risk of incident T2DM among normal weight participants [31]. Combining this finding in the same cohort with the finding from the current analysis demonstrating a lower risk of T2DM with greater thigh muscle area in normal weight participants, it appears that obesity modifies the associations between muscle mass or muscle strength and incident T2DM in a similar pattern in our population. Based on these findings, we can assume that interventions aimed at increasing muscle mass and strength in lean individuals may be more effective to reduce the risk of T2DM than in overweight or obese individuals.
The underlying mechanism for the diminution of the inverse relationship between baseline thigh muscle area and T2DM risk at higher levels of BMI is not known. A possible reason is thigh muscle mass may have a relatively smaller impact on the development of T2DM in obese subjects due to preexisting metabolic imbalance caused by obesity. Therefore, the potential protective effects of greater muscle mass are overcome by much stronger effects of adiposity on T2DM risk. Our finding of a significant inverse association between thigh muscle area and future insulin resistance that did not vary by BMI further supports this theory, as this means that the potential mechanism for higher T2DM risk (i.e., greater insulin resistance) affects lean and non-lean similarly, and therefore must be overcome by other factors in the non-lean that prevent expression of this lower risk.
We noted that greater thigh subcutaneous fat area was associated with higher insulin sensitivity at 10 years. This finding might therefore be expected to result in lower risk of developing T2DM. However, we did not identify an association between thigh subcutaneous fat area and risk of T2DM in a previous analysis of these same data [32].
As for the strengths of our study, study participants were from a well-designed community-based cohort with a long-term follow-up period. This prospective study design permitted assessment of thigh muscle area prior to the outcome assessment, thereby helping to establish temporal sequence not possible in cross-sectional research. Additional strengths include use of imaging to measure muscle areas, and also our focus on regional muscle as opposed the generalized lean mass.
There are several limitations to be considered in this study. First, we estimated thigh muscle mass instead of directly measuring thigh muscle area using imaging. However, this method has been previously validated [21]. Second, we used HOMA-IR and QUICKI as a surrogate for insulin sensitivity. Although not the gold standard method, it is a frequently used tool for assessing insulin sensitivity in large population based studies [1833]. Finally, as this study was restricted to middle-aged and older Japanese Americans, caution should be taken when generalizing the results to other age or ethnic groups.
In conclusion, we found that thigh muscle area was inversely associated with future insulin resistance over 10 years in Japanese Americans. In addition, greater thigh muscle area was associated with lower risk of incident T2DM for leaner subjects independent of insulin resistance. These results suggest an important role for muscle mass in the development of T2DM that varies by degree of adiposity, and might lead to research to improve our understanding of the roles of both lean and non-lean body composition in the pathogenesis of hyperglycemia. Further intervention studies are needed to confirm whether increasing muscle mass can reduce the incidence of T2DM, and whether such effects vary according to BMI.
 XML Download
XML Download