

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Diabetes is a major public health problem in modern society because of its increasing prevalence and associated morbidity and mortality [1]. The mortality rate of patients with diabetes was reported to be 2- to 3-fold higher than that of the general population [23]. Along with progress in diabetes care, especially in the management of cardiovascular disease (CVD) risks [4], substantial decreases in overall, and CVD mortality rates have been observed in participants with diabetes [567]. Several studies have even reported a decreased gap in mortality rates between individuals with and without diabetes [2]. However, other studies have shown an increase in diabetes-related mortality [89]. This discrepancy is likely to be due to differences in study populations or regions, as well as the period in which the studies were conducted.
In developing countries in Asia, diabetes has become a serious health problem [101112]. According to the World Health Organization, approximately 80% of diabetes-related deaths occurred in low- and middle-income countries, including many Asian countries [11]. However, information on diabetes-related mortality in this region is insufficient and outdated. A previous report from South Korea showed that mortality rates for people with diabetes increased continuously from 1983 to 2001 [9]. However, some evidence indicates that diabetes care has improved and treatment rates for diabetes-related conditions have increased in South Korea [1314]. Thus, more recent and accurate evidence is required because such data would profoundly influence general public health policies.
We aimed to assess and compare all-cause and CVD mortality rates and recent trends for subjects with and without diabetes using a nationwide population-based cohort (2003 to 2013).
Go to : 
METHODS
Study population
The Korean National Health Insurance Service (NHIS) is responsible for health insurance and health promotion programs for all citizens of South Korea. Recently, the Korean NHIS released a National Sample Cohort (2002 to 2013) database comprising the data of 1,025,340 Koreans (approximately 2.2% of the total South Korean population in 2002) who were followed up until 2013, with samples for newborn infants updated annually. The database included information on medical care of the individuals, disease history, health check-up data, and basic demographic information. In addition, the database was merged with death records kept by the Korean National Statistical Office. More detailed descriptions of the NHIS study protocol and methods have been published elsewhere [15].
We divided all subjects from the database into two groups based on their diabetes status: those with diabetes mellitus (DM) group and those without (non-DM) group. Diabetes was defined as the clinical and pharmacy codes (E10–E14) for diabetes from the International Classification of Disease, 10th revision (ICD-10, Korean version).
Determination of cause of death
The date of death was identified in the cohort database. The cause of death was categorized in accordance with the ICD-10 codes: total CVD (I00–I99), ischemic heart disease (I20–I25), and ischemic stroke (I63–I66).
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Korea University Hospital (IRB number: ED14188). Informed consent was not obtained specifically because this study was based on the NHIS data which were fully anonymized and deidentified for the analysis.
Statistical analysis
To control for the effects of the different population structures of the two groups, we used standardized death rates and adjusted them for age and sex, using the 2003 population structure in the NHIS cohort data as the reference group [16]. The rates were then normalized to a common baseline to allow comparisons. The direct standardization method was calculated based on the following equation:
Here, the entire study population was divided into K age-sex groups. Pk is the proportion of the kth group in the 2003 reference population and dk the death rate of the kth group of the study population. We also calculated 95% confidence intervals for the standardized death rates, as described previously [17]. To analyze the time trends of the age- and sex-adjusted standardized death rates in the DM and non-DM groups, we fitted a simple regression model to each standardized death rate over time. Each time trend was then tested under a two-sided assumption, and its significance was addressed when the P value was <0.05.
All statistical analyses were performed using SAS version 9.4 software (SAS Institute Inc., Cary, NC, USA).
Go to :
RESULTS
The total number of subjects in this analysis ranged from 585,795 in 2003 to 670,020 in 2013. During this period, a total of 54,568 deaths occurred: 17,101 in the DM group and 37,467 in the non-DM group. The crude numbers and rates of death are displayed in the Table 1. In both groups, the death rates from CVD continuously declined over time.
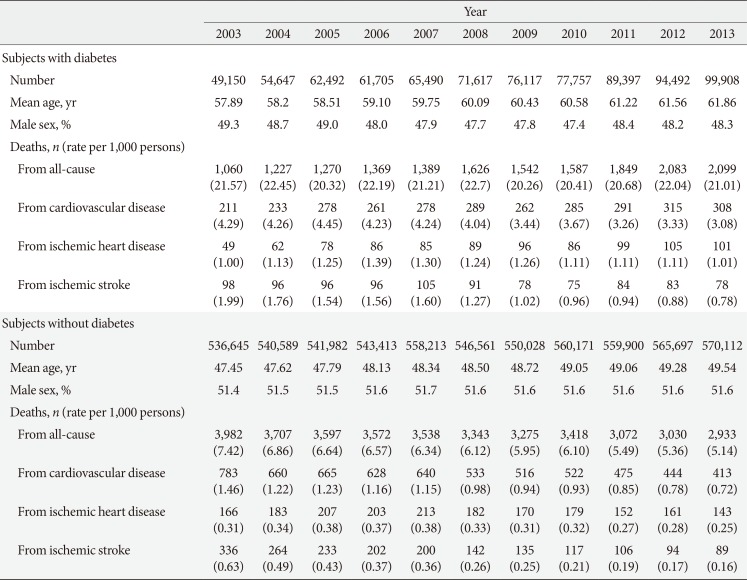
Table 1
Causes and annual number of deaths in subjects with and without diabetes from 2003 to 2013
![]()
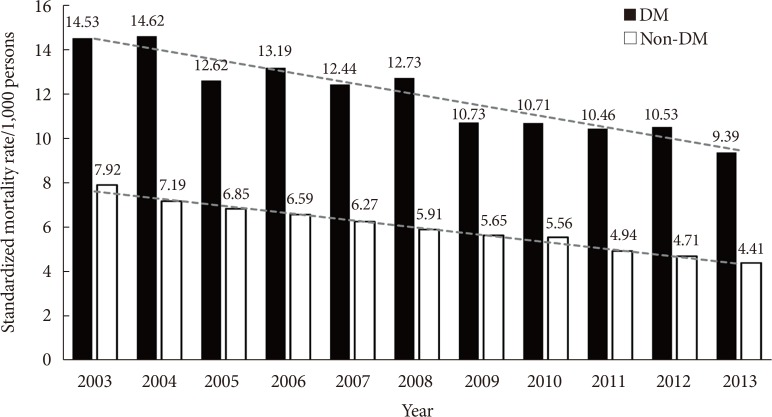
Fig. 1 shows the annual trends of the standardized mortality rates (per 1,000 persons) in both groups from 2003 to 2013. The all-cause standardized mortality rates consistently decreased in both groups: from 14.5 per 1,000 persons in 2003 to 9.4 per 1,000 persons in 2013 in the DM group and from 7.9 per 1,000 persons to 4.4 per 1,000 persons in the non-DM group (P value for trend <0.001 in both groups). In addition, the difference in the mortality rate for subjects with diabetes relative to those without diabetes also decreased from 2003 to 2013 (from 6.61 per 1,000 persons in 2003 to 4.98 per 1,000 persons in 2013).
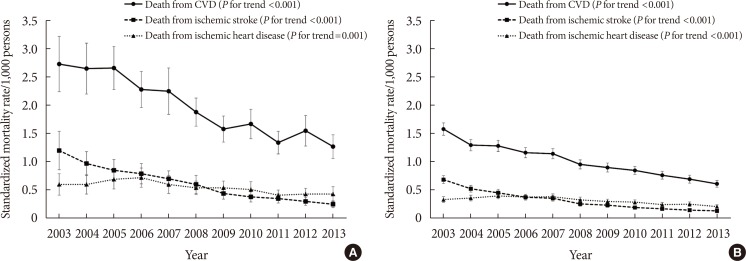
We also assessed the cause-specific standardized mortality rates from total CVD and CVD subtypes. Fig. 2A shows those annual trends in subjects with diabetes. Similar to the trends for all-cause mortality, the rate of CVD mortality decreased significantly by 53.5% in subjects with diabetes (from 2.73 to 1.27 per 1,000 persons, P for trend <0.001). Deaths from ischemic stroke (from 1.20 to 0.25 per 1,000 persons, P for trend <0.001) accounted for a larger proportion of that reduction compared to deaths from ischemic heart disease (from 0.60 to 0.43 per 1,000 persons, P for trend=0.001). Similar trends of CVD mortality decline were found in subjects without diabetes (Fig. 2B).
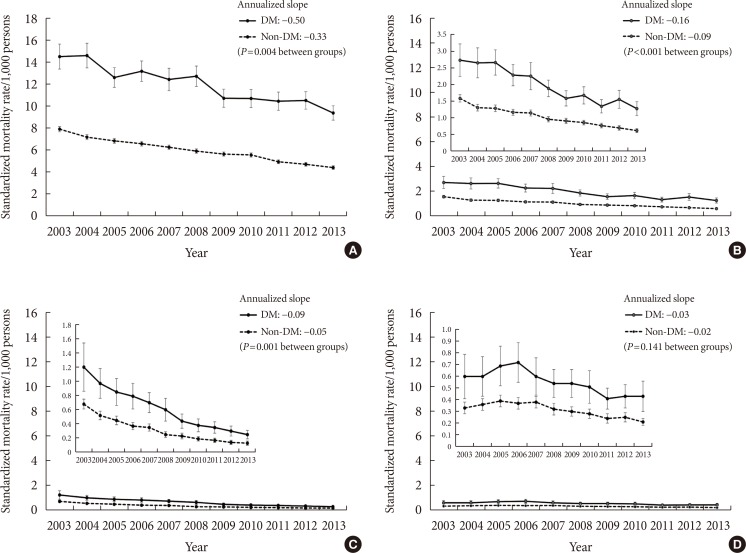
To compare the decreasing trends in mortality rates between subjects with and without diabetes, we measured the annualized slope of decline in both groups. The rate of decline was 1.52-fold greater in the DM group than in the non-DM group (regression coefficients of time: −0.50 and −0.33, respectively; P=0.004) (Fig. 3A). Similar patterns were observed for other types of cause-specific death, including total CVD (1.82-fold greater, P<0.001) (Fig. 3B) and ischemic stroke (1.78-fold greater, P=0.001) (Fig. 3C). However, the slope associated with the decreasing ischemic heart disease death rate was comparable between the two groups (Fig. 3D).
Go to :
DISCUSSION
In this population-based cohort study, we reported several important findings in terms of mortality rates and trends in individuals with and without diabetes in South Korea. First, between 2003 and 2013, all-cause and CVD mortality rates decreased substantially in subjects with and without diabetes. In addition, the mortality rate decreased more rapidly in subjects with diabetes than in those without diabetes, reducing the gap in mortality rates between the two groups. Finally, the decrease in CVD mortality was primarily attributable to a decrease in mortality from ischemic stroke, rather than from ischemic heart disease, among subjects with diabetes.
Previous studies have shown that recent all-cause and CVD mortality rates have decreased in patients with diabetes. According to the U.S. National Health Interview Survey, all-cause mortality decreased by 23% and CVD-related mortality decreased by 40% among adults with diabetes between 1997 and 2006 [2]. Similar findings were observed in studies from other developed countries during the same period [67]. These findings were largely attributable to improvements in the treatment of diabetes and its associated conditions, including hypertension and dyslipidemia [18]. The decline in the rate of diabetes-related complications over recent decades [19] also contributed to the improvements in mortality. However, this has not consistently been the case across different populations and different time periods. In a serial National Health and Nutrition Examination Survey study from 1971 to 2000, improvement in the mortality rate of patients with diabetes was limited to men [20]. Furthermore, in a Mexican population, the diabetes-related mortality rate increased from 1980 to 2000 [8]. These findings suggest that evidence of reduced diabetes-related mortality rates is limited to recent studies in developed countries.
A previous population-based study in South Korea reported disappointing results: from 1983 to 2000, the diabetes-related mortality rate increased substantially (from 5.3 to 18.4 deaths per 100,000 people) [9]. The researchers stated that the reasons for this increase were rapid urbanization, increased intake of foods in high calories, and decreased physical activity. However, using a nationwide cohort data since the 2000s (from 2003 to 2013), we showed the opposite results. Some evidence supports our findings. A serial Korean National Health and Nutrition Examination Survey study of diabetic patients indicated that the treatment rate substantially increased from 1998 to 2005 (from 26.8% to 48.8%) [13]. Recently, the Korean Diabetes Association reported that diabetes care had improved rapidly in South Korea, with medical costs for diabetes being 5.8-fold higher in 2013 than in 2002. In addition, the proportion of patients who adhered to their medication schedule by more than 80% per year increased 2.8-fold (from 24.1% to 67.2%) during the same period [14]. We postulated that progress in the management of diabetes care led to a significant decrease in mortality among people with diabetes in South Korea. Although there were no significant improvements of glycemic control rate over the last decade [2122], we suppose that factors other than glycemic control including wide use of anti-hypertensive drugs or statins may contributed to the improvement of mortality rate in patients with diabetes. In addition, easy medical accessibility which is one of the strength in terms of medical care in Korea might be one main reason of the mortality reduction. Meanwhile, widespread screening by the national checkup programs in Korea has increased early detection and early diagnosis of diabetes. It may have affected the decreased mortality rate in patients with diabetes.
Several reports in the United States and Canada found a substantial decrease in CVD-related mortality among patients with diabetes [23]. The results of the present study are consistent with those findings. An interesting finding of this study was the substantial decrease in ischemic stroke-related mortality in subjects with diabetes. The ischemic stroke mortality in subjects with diabetes was 2-fold higher than ischemic heart disease mortality in 2003. However, 10 years later, ischemic stroke mortality was even lower than ischemic heart disease mortality. Furthermore, the decreasing slope associated with ischemic stroke mortality was 3.5-fold steeper than that of ischemic heart disease mortality in people with diabetes.
Improvements in the management of ischemic stroke and its risk factors may have largely contributed to the decline of ischemic stroke mortality. The treatment rate for hypertension has increased by about 2-fold during the last two decades, currently exceeding 65% [1423]. The proportion of patients receiving lipid-lowering medications also increased, being 5-fold greater in 2013 than in 2003 [24]. Moreover, the index for acute management of stroke has improved. In the Korean Stroke Registry study, the percentage of patients who arrived at the hospital within 3 hours of the initiation of stroke symptoms increased from 20% to 29% and the rate of reperfusion therapy increased from 5.3% to 7.0% between 2002 and 2010 [25]. In addition, the number of hospitals with an installed stroke unit has increased substantially [26]. Currently, South Korea has the lowest in-hospital 30-day ischemic stroke-related fatality rate among Organization for Economic Co-operation and Development nations [27]. Consequently, prevalent use of antihypertensive and lipid-lowering agents and improved acute management of stroke in South Korea seem to be major contributors to the marked decrease in ischemic stroke mortality.
Our study has some limitations. First, we did not distinguish between type 1 diabetes mellitus and type 2 diabetes mellitus because of a lack of exact information to define the types of diabetes. Currently, approximately 5% of people with diabetes are presumed to have type 1 diabetes mellitus in Korea. Although it is a small percentage, it could limit the interpretation of our results. Second, approximately 10% of the total deaths in this cohort were classified as “unknown cause.” We speculated that the majority of those cases were sudden cardiac deaths or deaths related to cardiopulmonary disease. However, we did not include those deaths in the CVD mortality category. Therefore, it is possible that we underestimated the actual number of CVD deaths.
In summary, overall and CVD mortality rates continuously decreased in subjects with diabetes from 2003 to 2013 in South Korea. The reduction in CVD mortality was primarily attributable to a reduction in ischemic stroke mortality. The gap between the mortality rates of subjects with and without diabetes continuously decreased over time; however, the mortality rate of individuals with diabetes was still more than 2-fold higher than that of individuals without diabetes. Further studies about contributing factors associated with improvement of mortality rate in subjects with diabetes are needed to provide valuable therapeutic information in clinical practice.
Go to :
 XML Download
XML Download