This article has been
cited by other articles in ScienceCentral.
Abstract
We analyzed circulating soluble epidermal growth factor receptor (sEGFR) levels in humans. Serum sEGFR levels were higher in subjects with newly diagnosed type 2 diabetes mellitus compared with controls. Serum sEGFR was positively correlated with glycosylated hemoglobin and serum glucose and negatively correlated with serum insulin and C-peptide levels.
Go to :

Keywords: Biological assay, Diabetes mellitus, type 2, Receptor, epidermal growth factor
INTRODUCTION
The epidermal growth factor receptor (EGFR; also known as ErbB1 and HER1) gene is a member of the ErbB receptor tyrosine kinase family [
1]. The soluble epidermal growth factor receptor (sEGFR) is a 110 kDa peptide generated through proteolytic cleavage of a cell surface precursor of an alternately spliced EGFR isoform [
2]. sEGFR has been detected in normal and malignant cells, many tissues, and in biological fluids. Recent studies suggest that sEGFR is a useful circulating serum biomarker in patients with cancer. However, the relationship between metabolic disorders and serum sEGFR levels remains poorly understood. In this study, we measured serum sEGFR levels in subjects with newly diagnosed type 2 diabetes mellitus (T2DM) and explored the correlations between serum sEGFR levels and various metabolic parameters.
Go to :
METHODS
Study design
A total of 103 subjects with newly diagnosed T2DM and 109 healthy subjects without diabetes aged 18 years or older were recruited from the department of endocrinology at Chungnam National University Hospital from 2014 to 2016. Exclusion criteria included a history of taking oral hypoglycemic medication or tyrosine kinase inhibitors (TKIs). Subjects with acute infectious disease and a history of malignancy were also excluded. Medical history (age, sex, drugs used, smoking, and underlying disease) and anthropometric measurements (height and weight) were taken. Plasma samples were obtained from all subjects to measure biochemical markers at baseline and 2 hours after ingesting a 75-g oral glucose load. T2DM was diagnosed according to the 2016 American Diabetes Association criteria [
3]. The Institutional Review Board (2014-12-013-001) of Chungnam National University Hospital approved the protocol for this research, and written informed consent was obtained from all participants.
Biochemical data
Blood samples were collected using ethylenediaminetetraacetic acid tubes in the morning after an overnight fast >8 hours and 2 hours after ingesting a 75-g oral glucose load. The lipid profile (high density lipoprotein cholesterol [HDL-C], low density lipoprotein cholesterol [LDL-C], total cholesterol [TC], and triglycerides [TGs]) was measured using a blood chemistry analyzer (Hitachi 747; Hitachi, Tokyo, Japan). Insulin was quantified using an immunoradiometric assay kit (DIAsource INS-IRMA Kit; DIAsource, Louvain-la-Neuve, Belgium). Glycosylated hemoglobin (HbA1c) was measured using high-performance liquid chromatography (BioRad Laboratories, Hercules, CA, USA). Homeostatic model assessment of insulin resistance (HOMA-IR) and homeostatic model assessment of β-cell function (HOMA-β) were calculated as:
HOMA-IR=fasting serum insulin (µU/mL)×fasting plasma glucose (mmol/L)/22.5
HOMA-β=20×fasting serum insulin (µU/mL)/[fasting plasma glucose (mmol/L)−3.5]
Fasting serum sEGFR levels were measured using a quantitative sandwich enzyme immunoassay technique with an enzyme-linked immunosorbent assay kit (Abcam, Cambridge, UK; catalog no. ab193764).
Statistical analyses
All parameter values were calculated as mean±standard deviation. A P<0.05 was considered statistically significant. The chi-square and Mann-Whitney U tests were used to compare the clinical characteristics and biochemical data between the two groups. Univariate and multivariate logistic regression analyses were used to assess the relationships between clinical characteristics, biochemical variables, and sEGFR levels.
Go to :
RESULTS
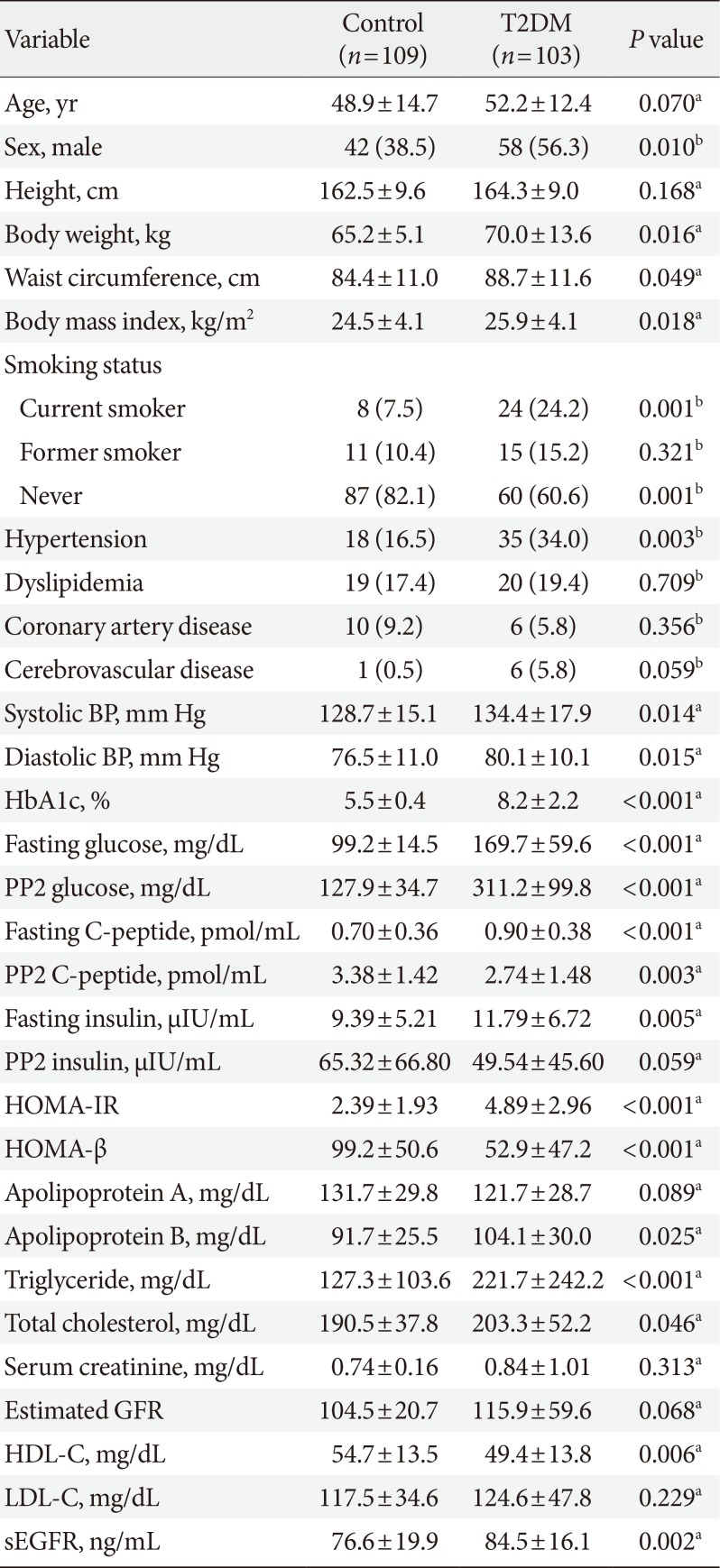
The clinical characteristics of the study participants are presented in
Table 1. Body mass index (BMI), body weight, waist circumference, glucose (fasting and 2-hour postprandial), C-peptide (fasting and 2-hour postprandial), insulin (fasting), HbA1c, HOMA-IR, HOMA-β, and TC in the T2DM group were higher than those in the controls; male gender, hypertension, and current smoker were more common in the T2DM group. HDL-C was lower in the T2DM group than that in the control group. Additionally, sEGFR levels were significantly higher in participants with T2DM than in those without T2DM. We further adjusted for age, sex, BMI, serum creatinine, and smoking status as confounders. Even after adjustments, there were still significant differences in sEGFR levels between subjects with and without T2DM (
P=0.002) (data not shown).
Table 1
Baseline characteristics
|
Variable |
Control (n=109) |
T2DM (n=103) |
P value |
|
Age, yr |
48.9±14.7 |
52.2±12.4 |
0.070a
|
|
Sex, male |
42 (38.5) |
58 (56.3) |
0.010b
|
|
Height, cm |
162.5±9.6 |
164.3±9.0 |
0.168a
|
|
Body weight, kg |
65.2±5.1 |
70.0±13.6 |
0.016a
|
|
Waist circumference, cm |
84.4±11.0 |
88.7±11.6 |
0.049a
|
|
Body mass index, kg/m2
|
24.5±4.1 |
25.9±4.1 |
0.018a
|
|
Smoking status |
|
|
|
|
Current smoker |
8 (7.5) |
24 (24.2) |
0.001b
|
|
Former smoker |
11 (10.4) |
15 (15.2) |
0.321b
|
|
Never |
87 (82.1) |
60 (60.6) |
0.001b
|
|
Hypertension |
18 (16.5) |
35 (34.0) |
0.003b
|
|
Dyslipidemia |
19 (17.4) |
20 (19.4) |
0.709b
|
|
Coronary artery disease |
10 (9.2) |
6 (5.8) |
0.356b
|
|
Cerebrovascular disease |
1 (0.5) |
6 (5.8) |
0.059b
|
|
Systolic BP, mm Hg |
128.7±15.1 |
134.4±17.9 |
0.014a
|
|
Diastolic BP, mm Hg |
76.5±11.0 |
80.1±10.1 |
0.015a
|
|
HbA1c, % |
5.5±0.4 |
8.2±2.2 |
<0.001a
|
|
Fasting glucose, mg/dL |
99.2±14.5 |
169.7±59.6 |
<0.001a
|
|
PP2 glucose, mg/dL |
127.9±34.7 |
311.2±99.8 |
<0.001a
|
|
Fasting C-peptide, pmol/mL |
0.70±0.36 |
0.90±0.38 |
<0.001a
|
|
PP2 C-peptide, pmol/mL |
3.38±1.42 |
2.74±1.48 |
0.003a
|
|
Fasting insulin, µIU/mL |
9.39±5.21 |
11.79±6.72 |
0.005a
|
|
PP2 insulin, µIU/mL |
65.32±66.80 |
49.54±45.60 |
0.059a
|
|
HOMA-IR |
2.39±1.93 |
4.89±2.96 |
<0.001a
|
|
HOMA-β |
99.2±50.6 |
52.9±47.2 |
<0.001a
|
|
Apolipoprotein A, mg/dL |
131.7±29.8 |
121.7±28.7 |
0.089a
|
|
Apolipoprotein B, mg/dL |
91.7±25.5 |
104.1±30.0 |
0.025a
|
|
Triglyceride, mg/dL |
127.3±103.6 |
221.7±242.2 |
<0.001a
|
|
Total cholesterol, mg/dL |
190.5±37.8 |
203.3±52.2 |
0.046a
|
|
Serum creatinine, mg/dL |
0.74±0.16 |
0.84±1.01 |
0.313a
|
|
Estimated GFR |
104.5±20.7 |
115.9±59.6 |
0.068a
|
|
HDL-C, mg/dL |
54.7±13.5 |
49.4±13.8 |
0.006a
|
|
LDL-C, mg/dL |
117.5±34.6 |
124.6±47.8 |
0.229a
|
|
sEGFR, ng/mL |
76.6±19.9 |
84.5±16.1 |
0.002a
|

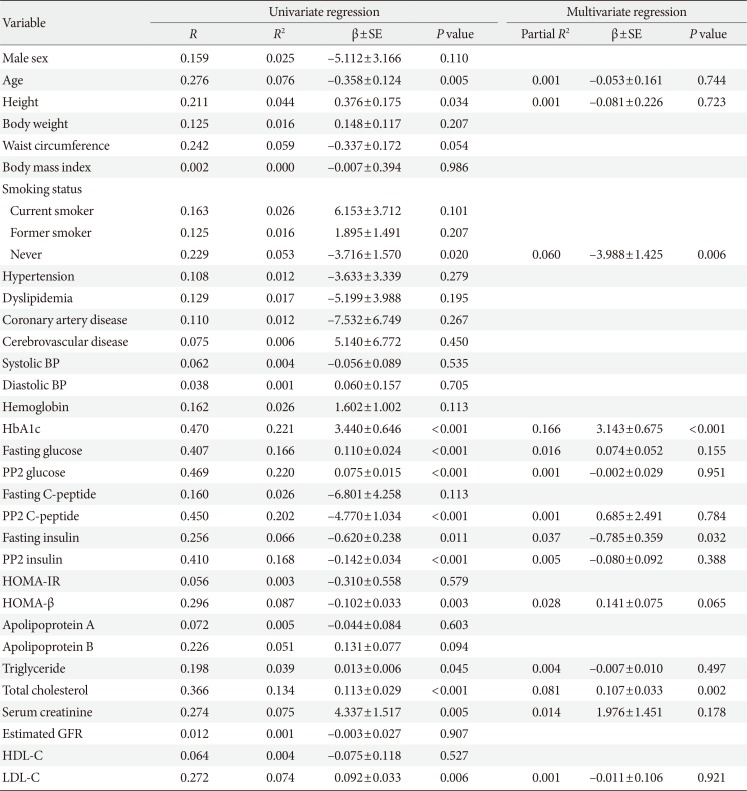
We also investigated the associations between sEGFR and clinical variables in the T2DM group. Univariate logistic regression indicated that sEGFR levels were strongly associated with HbA1C (
r=0.470,
P<0.001), fasting glucose (
r=0.407,
P<0.001), postprandial glucose (
r=0.469,
P<0.001), postprandial C-peptide (
r=0.450,
P<0.001), and insulin (
r=0.410,
P<0.001). We also found a correlation between HOMA-β (
r=0.296,
P=0.003), TC (
r=0.366,
P<0.001), TG (
r=0.198,
P=0.045), serum creatinine (
r=0.274,
P=0.005), and LDL-C (
r=0.272,
P=0.006). Multivariate analysis revealed that sEGFR level was associated with HbA1c (
P<0.001) (
Table 2).
Table 2
Regression analysis between various clinical factors and the soluble epidermal growth factor receptor in T2DM group
|
Variable |
Univariate regression |
Multivariate regression |
|
R
|
R2
|
β±SE |
P value |
Partial R2
|
β±SE |
P value |
|
Male sex |
0.159 |
0.025 |
−5.112±3.166 |
0.110 |
|
|
|
|
Age |
0.276 |
0.076 |
−0.358±0.124 |
0.005 |
0.001 |
−0.053±0.161 |
0.744 |
|
Height |
0.211 |
0.044 |
0.376±0.175 |
0.034 |
0.001 |
−0.081±0.226 |
0.723 |
|
Body weight |
0.125 |
0.016 |
0.148±0.117 |
0.207 |
|
|
|
|
Waist circumference |
0.242 |
0.059 |
−0.337±0.172 |
0.054 |
|
|
|
|
Body mass index |
0.002 |
0.000 |
−0.007±0.394 |
0.986 |
|
|
|
|
Smoking status |
|
|
|
|
|
|
|
|
Current smoker |
0.163 |
0.026 |
6.153±3.712 |
0.101 |
|
|
|
|
Former smoker |
0.125 |
0.016 |
1.895±1.491 |
0.207 |
|
|
|
|
Never |
0.229 |
0.053 |
−3.716±1.570 |
0.020 |
0.060 |
−3.988±1.425 |
0.006 |
|
Hypertension |
0.108 |
0.012 |
−3.633±3.339 |
0.279 |
|
|
|
|
Dyslipidemia |
0.129 |
0.017 |
−5.199±3.988 |
0.195 |
|
|
|
|
Coronary artery disease |
0.110 |
0.012 |
−7.532±6.749 |
0.267 |
|
|
|
|
Cerebrovascular disease |
0.075 |
0.006 |
5.140±6.772 |
0.450 |
|
|
|
|
Systolic BP |
0.062 |
0.004 |
−0.056±0.089 |
0.535 |
|
|
|
|
Diastolic BP |
0.038 |
0.001 |
0.060±0.157 |
0.705 |
|
|
|
|
Hemoglobin |
0.162 |
0.026 |
1.602±1.002 |
0.113 |
|
|
|
|
HbA1c |
0.470 |
0.221 |
3.440±0.646 |
<0.001 |
0.166 |
3.143±0.675 |
<0.001 |
|
Fasting glucose |
0.407 |
0.166 |
0.110±0.024 |
<0.001 |
0.016 |
0.074±0.052 |
0.155 |
|
PP2 glucose |
0.469 |
0.220 |
0.075±0.015 |
<0.001 |
0.001 |
−0.002±0.029 |
0.951 |
|
Fasting C-peptide |
0.160 |
0.026 |
−6.801±4.258 |
0.113 |
|
|
|
|
PP2 C-peptide |
0.450 |
0.202 |
−4.770±1.034 |
<0.001 |
0.001 |
0.685±2.491 |
0.784 |
|
Fasting insulin |
0.256 |
0.066 |
−0.620±0.238 |
0.011 |
0.037 |
−0.785±0.359 |
0.032 |
|
PP2 insulin |
0.410 |
0.168 |
−0.142±0.034 |
<0.001 |
0.005 |
−0.080±0.092 |
0.388 |
|
HOMA-IR |
0.056 |
0.003 |
−0.310±0.558 |
0.579 |
|
|
|
|
HOMA-β |
0.296 |
0.087 |
−0.102±0.033 |
0.003 |
0.028 |
0.141±0.075 |
0.065 |
|
Apolipoprotein A |
0.072 |
0.005 |
−0.044±0.084 |
0.603 |
|
|
|
|
Apolipoprotein B |
0.226 |
0.051 |
0.131±0.077 |
0.094 |
|
|
|
|
Triglyceride |
0.198 |
0.039 |
0.013±0.006 |
0.045 |
0.004 |
−0.007±0.010 |
0.497 |
|
Total cholesterol |
0.366 |
0.134 |
0.113±0.029 |
<0.001 |
0.081 |
0.107±0.033 |
0.002 |
|
Serum creatinine |
0.274 |
0.075 |
4.337±1.517 |
0.005 |
0.014 |
1.976±1.451 |
0.178 |
|
Estimated GFR |
0.012 |
0.001 |
−0.003±0.027 |
0.907 |
|
|
|
|
HDL-C |
0.064 |
0.004 |
−0.075±0.118 |
0.527 |
|
|
|
|
LDL-C |
0.272 |
0.074 |
0.092±0.033 |
0.006 |
0.001 |
−0.011±0.106 |
0.921 |
Go to :
DISCUSSION
In previous studies, sEGFR has been mainly evaluated as it relates to cancer, as plasma sEGFR is useful for predicting survival in advanced non-small cell lung cancer [
4], and sEGFR is a useful marker for predicting the prognosis or therapeutic response for cervical, colorectal, ovarian, and breast cancers [
1]. However, few studies have been reported on other diseases, such as metabolic disease. In several studies, hyperglycemia has been reported as a side effect with increased use of a TKI as a target therapy in patients with cancer [
56]. On the other hand, hypoglycemia was observed after TKI treatment in subjects with diabetes [
7]. Taken together, sEGFR is related to glucose metabolism because many TKIs affect glucose metabolism and the EGFR. In this study, sEGFR level was higher in subjects with T2DM compared with that in the controls. A univariate analysis of the T2DM group revealed that sEGFR was correlated with HbA1c, fasting and 2-hour postprandial serum glucose, suggesting a possibility that EGFR could be a diagnostic marker for T2DM. Recently Kyohara et al. [
8] reported that sEGFR was increased in T2DM patient, which is the same as our study result. However, this study has several limitations that insignificant difference of sEGFR levels, small study population, and the drug effect could not be ruled out because diabetic patients treated with oral hypoglycemic agents were included. In addition, since the above study was conducted on inpatients, there was likely to be a bias based on general health problem. In our study, we included more patients and healthy controls, and patients were drug- naïve state. The correlation between HOMA-IR and sEGFR levels showed negative in this study and positive in the study of Kyohara et al. [
8]. However, both were not statistically significant.
Moreover, a significant correlation was observed between LDL-C, TC, and serum creatinine in the diabetic group, which was expected to play roles as diagnostic markers for diabetes and help predict the risk of complications in patients with diabetes. In addition, a negative correlation was observed between C-peptide and insulin levels, which may be helpful in predicting insulin reserve in patients with newly diagnosed diabetes. Kyohara et al. [
8] reported that there was a positive correlation between serum fasting insulin and sEGFR levels, though correlation was not statistically significant. Additional studies will be needed to investigate this issue.
This study has several limitations. First, this was a retrospective and cross sectional study, and sEGFR was measured only in the fasting sample. The change in sEGFR level according to glucose fluctuation was not confirmed. Second, the mechanism for increased sEGFR in diabetes was unclear. Considering the previous studies [
8910], it is presumed that sEGFR may be associated with insulin signaling or pancreatic β-cell mass regulation. In order to investigate this issue, additional studies will be needed. The study of the mechanism may also help to confirm the correlation between fasting insulin and sEGFR mentioned earlier.
In conclusion, our study demonstrates for the first time that sEGFR levels are higher in patients with newly diagnosed T2DM. Moreover, sEGFR was significantly correlated with HbA1c and serum glucose in patients with T2DM.
Go to :
ACKNOWLEDGMENTS
The biospecimens and data used for this study were provided by the Biobank of Chungnam National University Hospital, a member of the Korea Biobank Network. This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean Government (NRF-2016R1D1A1A09916900).
Go to :
Notes
Go to :
References
1. Guillaudeau A, Durand K, Bessette B, Chaunavel A, Pommepuy I, Projetti F, Robert S, Caire F, Rabinovitch-Chable H, Labrousse F. EGFR soluble isoforms and their transcripts are expressed in meningiomas. PLoS One. 2012; 7:e37204. PMID:
22623992.

2. Wilken JA, Perez-Torres M, Nieves-Alicea R, Cora EM, Christensen TA, Baron AT, Maihle NJ. Shedding of soluble epidermal growth factor receptor (sEGFR) is mediated by a metalloprotease/fibronectin/integrin axis and inhibited by cetuximab. Biochemistry. 2013; 52:4531–4540. PMID:
23731208.
3. American Diabetes Association. 2. Classification and diagnosis of diabetes. Diabetes Care. 2016; 39(Suppl 1):S13–S22. PMID:
26696675.
4. Jantus-Lewintre E, Sirera R, Cabrera A, Blasco A, Caballero C, Iranzo V, Rosell R, Camps C. Analysis of the prognostic value of soluble epidermal growth factor receptor plasma concentration in advanced non-small-cell lung cancer patients. Clin Lung Cancer. 2011; 12:320–327. PMID:
21729651.
5. Racil Z, Razga F, Drapalova J, Buresova L, Zackova D, Palackova M, Semerad L, Malaskova L, Haluzik M, Mayer J. Mechanism of impaired glucose metabolism during nilotinib therapy in patients with chronic myelogenous leukemia. Haematologica. 2013; 98:e124–e126. PMID:
23716549.
6. Villadolid J, Ersek JL, Fong MK, Sirianno L, Story ES. Management of hyperglycemia from epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) targeting T790M-mediated resistance. Transl Lung Cancer Res. 2015; 4:576–583. PMID:
26629426.
7. Huda MS, Amiel SA, Ross P, Aylwin SJ. Tyrosine kinase inhibitor sunitinib allows insulin independence in long-standing type 1 diabetes. Diabetes Care. 2014; 37:e87–e88. PMID:
24757248.
8. Kyohara M, Shirakawa J, Okuyama T, Kimura A, Togashi Y, Tajima K, Hirano H, Terauchi Y. Serum quantitative proteomic analysis reveals soluble EGFR to be a marker of insulin resistance in male mice and humans. Endocrinology. 2017; 158:4152–4164. PMID:
29028997.
9. Miettinen PJ, Ustinov J, Ormio P, Gao R, Palgi J, Hakonen E, Juntti-Berggren L, Berggren PO, Otonkoski T. Downregulation of EGF receptor signaling in pancreatic islets causes diabetes due to impaired postnatal beta-cell growth. Diabetes. 2006; 55:3299–3308. PMID:
17130473.
10. Miettinen P, Ormio P, Hakonen E, Banerjee M, Otonkoski T. EGF receptor in pancreatic beta-cell mass regulation. Biochem Soc Trans. 2008; 36(Pt 3):280–285. PMID:
18481942.
Go to :


 PDF
PDF ePub
ePub Citation
Citation Print
Print



 XML Download
XML Download