

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The assessment of diabetic peripheral neuropathy (DPN) may be simple or complex and will be defined by what we are trying to achieve. In a busy clinic it is sufficient to establish whether an individual has symptoms, particularly of painful DPN and indeed through the use of a monofilament examination, whether or not the patient is at high risk of foot ulceration. However, for the assessment of early nerve damage and more precise phenotyping of somatic and autonomic neuropathy, a large number of specialized screening and diagnostic tests are available, which can be easily deployed. Clinically however, there is a nihilistic attitude towards diagnosing diabetic neuropathy. After all, apart from providing relief of painful neuropathic symptoms, there are no currently approved disease-modifying therapies. Therein lies another problem in relation to the modalities used to evaluate an improvement in diabetic neuropathy in clinical trials of new therapies. We have witnessed and will continue to witness spectacular and very costly failures of new therapeutics for DPN and indeed other peripheral and central neurodegenerative disorders. This review will consider the pros and cons of old established and newer methods for both diagnosing and evaluating DPN.
Go to : 
CLINICAL DIAGNOSIS OF DIABETIC PERIPHERAL NEUROPATHY
Damage to the small sensory nerve fibers is one of the earliest manifestations of DPN and may be accompanied by continuous or episodic pain [1]. Evaluation of neuropathic symptoms and signs using validated questionnaires and clinical bedside testing form the mainstay of DPN diagnosis along with a detailed history to exclude other possible causes [23]. In this section we summarize the most commonly used clinical diagnostic modalities (Table 1).
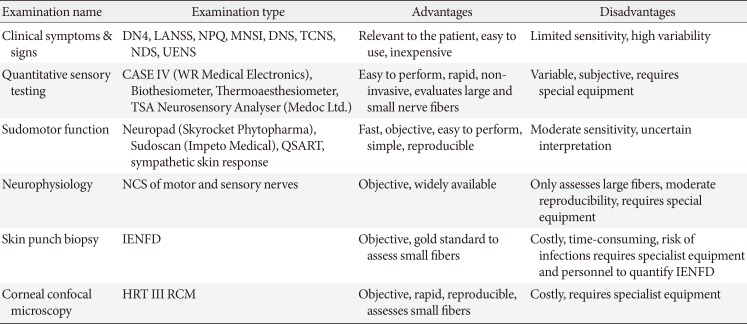
Table 1
Summary of methods for the diagnosis of diabetic peripheral neuropathy
DN4, Douleur Neuropathique en 4; LANSS, Leeds Assessment of Neuropathic Symptoms and Signs; NPQ, Neuropathic Pain Questionnaire; MNSI, Michigan Neuropathy Screening Instrument; DNS, Diabetic Neuropathy Symptom; TCNS, Toronto Clinical Neuropathy Score; NDS, neuropathy disability score; UENS, Utah Early Neuropathy Scale; QSART, Quantitative Sudomotor Axon Reflex Test; NCS, nerve conduction studies; IENFD, intra-epidermal nerve fiber density; HRT III RCM, Heidelberg Retina Tomograph III Rostock Corneal Module.
![]()
Symptoms and signs
The Douleur Neuropathique en 4 (DN4) includes questions for different types of neuropathic pain such as burning, painful cold, electrical shocks, tingling, pins and needles, numbness, and itching and a physical exam to test for touch and pin hypoesthesia and tactile dynamic allodynia and has shown excellent sensitivity (83%) and specificity (90%) for neuropathic pain [4]. The Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) scale is similar, elicits five symptoms and two signs of DPN and has a comparable sensitivity and specificity [5]. Other screening tests include the Neuropathic Pain Questionnaire (NPQ) (12 questions) [6], the Neuropathic Pain Symptoms Inventory (NPSI) (12 questions) [78], the Neurological Symptom Score (NSS) (17 questions) [9], Diabetic Neuropathy Symptom (DNS) score (four questions) [10]. These are all interview-based assessments of sensory, motor, and autonomic deficits, with moderate sensitivity and specificity. Several screening tests have also been validated to diagnose and stratify the severity of DPN. The Toronto Clinical Neuropathy Score (TCNS) [11] includes an assessment of symptoms (present or absent), sensory loss (normal or abnormal), and reflexes (normal, reduced, or absent). Based on the outcome a score of 6 to 8 denotes mild neuropathy, 9 to 11 moderate, and ≥12 severe neuropathy. The Michigan Neuropathy Screening Instrument (MNSI) consists of 15 self-administered questions adapted from the neuropathy symptom profile [12] and a score ≥7 is considered abnormal [13]. Similar to other clinical composite tests, the MNSI involves a foot examination, whereby each foot with an ulcer or other findings such as dry skin, infections, calluses, fissures, or deformities is scored 1. Other components include testing for vibration sensation using a 128-Hz tuning fork and Achilles reflexes using the Jendrassic manoeuver. The neuropathy disability score (NDS) [14] is a composite measure of vibration perception with a 128-Hz tuning fork, thermal perception with a metallic rod, pin-prick sensation, and Achilles tendon reflexes. The NDS is commonly used in research studies to stratify DPN severity as none (0 to 2), mild (3 to 5), moderate (6 to 8), and severe (9 to 10). The Utah Early Neuropathy Scale (UENS) is designed to identify signs of a predominantly small fiber neuropathy [15]. It consists of pin sensation, allodynia/hyperesthesia, large fiber and deep tendon reflex examinations and motor deficits, with a maximum score of 42.
Quantitative sensory testing
Quantitative sensory testing (QST) can be used to quantify small and large nerve fiber function. Commercially available devices include CASE IV (WR Medical Electronics, Stillwater, MN, USA), the thermoaesthesiometer, the biothesiometer, and the TSA II Neurosensory Analyzer (Medoc Ltd., Ramat Yishai, Israel). These devices create temperature and vibratory stimuli and rely on the subject's response to define sensory thresholds. QST is painless and non-invasive, requires minimal training and is relatively easy to perform, which make it an attractive option to diagnose neuropathy. However, several studies have reported variable sensitivity ranging from as low as 36% to 85% [1617], due to the impact of patient co-operation, enrolment of cohorts of different neuropathic severity and the use of different computers and algorithms to perform QST [18]. Early studies reporting poor reproducibility, which improved in subsequent studies [19] possibly due to improved algorithms and devices and taking into account patient reaction time to an external stimulus. The Neuropathy in Diabetes Study group has recommended the use of QST to diagnose DPN in combination with other tests [20], while the American Academy of Neurology considers QST to be of limited use in individual patients but of possible value in longitudinal studies of large cohorts [18]. Indeed, in a study of 498 patients with type 2 diabetes mellitus (T2DM) and 434 controls a significantly elevated warm detection threshold was the most common abnormality, followed by an abnormal cold detection threshold and sural nerve conduction velocity (NCV), which were related to symptoms and glycemic control [21]. However, a detailed study of 59 subjects with and without DPN showed that warm detection thresholds did not differentiate patients with and without symptoms, unlike cold detection threshold and intra-epidermal nerve fiber density (IENFD) [22]. QST has been employed as an outcome measure in clinical trials of neuropathy primarily due to ease of use, but with mixed results [2324]. Indeed, multi-risk factor control in the Steno-2 study [23] failed to show an improvement in DPN measured by vibration perception. In a phase III trial of human recombinant nerve growth factor, QST as a secondary endpoint failed to detect a significant treatment benefit [24].
Go to :
DIABETIC AUTONOMIC NEUROPATHY
Diabetic autonomic neuropathy (DAN) often coexists with diabetic somatic neuropathy. DAN may affect a number of different organ systems including the cardiovascular, gastrointestinal, genitourinary and sudomotor systems. Cardiovascular autonomic neuropathy (CAN) is clinically the most important form of DAN and is associated with abnormalities of heart rate control and vascular dynamics. Its prevalence varies from 16.8% to 34.3%, and clinical manifestations include resting tachycardia, exercise intolerance, silent myocardial ischemia, and orthostatic hypotension [25]. The most widely used assessments of CAN are based on the time-domain heart rate response to deep breathing, Valsalva manoeuver and change in posture. Gastrointestinal autonomic neuropathy represents a complex disorder that affects gastrointestinal motor and sensory control and leads to esophageal dysmotility, gastroparesis, constipation, diarrhea, and fecal incontinence [26]. It can be assessed with the Diabetes Bowel Symptom Questionnaire [27] and by evaluating gastric emptying using a radionuclide labeled meal [28]. Bladder dysfunction has an estimated prevalence of 25% to 87% [29] and symptoms may include dysuria, nocturia, incomplete bladder emptying, and recurrent urinary tract infections [20]. Assessments for bladder dysfunction include a lower urinary tract symptoms questionnaire, measurement of peak urinary flow rate and post-void residual volume [30]. Erectile dysfunction complicates around 52.5% [31] of men with diabetes and can be assessed by means of the International Index of Erectile Function and the Sexual Encounter Profile, nocturnal penile tumescence, penile Doppler ultrasound, sacral response, bulbocavernosus reflex, dorsal sensory nerve conduction of the penis, amplitude and latency of penile sympathetic skin response, and pudendal nerve somatosensory-evoked potentials [32]. Sudomotor dysfunction may be one of the earliest manifestations of DAN resulting in loss of sweating and can be evaluated via several modalities. Sympathetic skin response previously failed to detect DPN in a study of 337 patients with diabetes [33], but more recently it was shown to predict the risk of foot ulceration, comparable to abnormalities in NDS and vibration perception [34]. The quantitative sudomotor axon reflex test evaluates postganglionic axonal integrity, whilst the sympathetic skin response assesses polysynaptic pathways and has previously been shown to be superior for detecting early neuropathy compared to the sympathetic skin response in a small series of 31 patients with diabetes [35]. The sweat indicator plaster [36] (Neuropad) is a visual test, which uses a timed color change to define the integrity of skin sympathetic cholinergic innervation. A prospective study of 109 patients with diabetes mellitus (DM) [37] reported that abnormalities on Neuropad in subjects without DPN were a strong predictor for the subsequent development of DPN, within 5 years. This is an important finding given that abnormal sweating is associated with small fiber neuropathy [38] commonly missed with bedside testing. The thermoregulatory sweat test [39] is a method of assessing location specific alterations by delivering a controlled heat stimulus to induce a generalized sweat response. The patient's response is detected by assessing a significant color change in cornstarch, sodium carbonate, or alizarin red, which are applied uniformly over the body. Finally, the Sudoscan test (Impeto Medical, San Diego, CA, USA) assesses electrochemical skin conductance as an indicator of sweat gland function and can differentiate patients with and without neuropathy and controls with high sensitivity and specificity as well as patients with and without CAN [40].
Go to :
NEUROPHYSIOLOGY
Nerve conduction studies (NCS) are considered to be the gold standard for the diagnosis of DPN. The Toronto consensus [20] recommended the use of abnormal NCS with a symptom or sign to diagnose DPN. The typical electrophysiological findings in DPN are amplitude reduction of the compound muscle action potential, slowing of sensory and motor NCV, prolonged F-wave latency and an absent Hoffman reflex. Although NCS provide an objective means of quantifying peripheral large nerve fiber dysfunction it cannot assess small sensory fiber damage, the earliest manifestation of DPN. A recent study [22] in DM patients with/without sensory symptoms and normal NCS showed that IENFD and thermal thresholds were significantly reduced compared to healthy controls but also differed between the symptomatic and asymptomatic groups. This finding highlights that small fiber injury occurs early in DPN and cannot be captured by NCS. Another major limitation is poor reproducibility and lack of measurement standardization across centers. Dyck et al. [41] found poor interobserver repeatability amongst expert neurophysiologists who independently assessed eight attributes of NCS in the same patients with diabetes on consecutive occasions. The magnitude of variability was a major point of concern and the authors rather than questioning the viability of this test, simply recommended that the same examiners should perform all NCS assessments in clinical trials of neuropathy.
Several studies [4243444546] have reported NCS abnormalities in patients with impaired glucose tolerance (IGT) and DM. Sumner et al. [42] found a reduction in IENFD, sural nerve amplitude and conduction velocity in patients with IGT and DM, with more marked abnormalities in patients with DM with a predominantly small fiber neuropathy in the IGT group. Glycemic control, DM duration, age, male gender, and height are associated with electrodiagnostic abnormalities in patients with DM [45]. More recently it has been suggested that quantification of the Hoffman reflex as a result of anhidrotic stimulation of type 1a sensory fibers may be a sensitive electrophysiological measure of DPN and a marker of spinal disinhibition [47]. Indeed, Millan-Guerrero et al. [48] reported that the Hoffman reflex was absent in 39.3% of T2DM patients compared to only 9.3% with abnormal NCS. Another recent study [49] found that assessment of rate dependent depression, a measure of change in amplitude of the Hoffman reflex, is able to identify differences in experimental and human DPN in relation to the contribution of spinal inhibitory pathways driving neuropathic pain.
Despite serial failure as an end point, most clinical trials [5051525354] have used NCS as the primary outcome to assess treatment efficacy. Kennedy et al. [50] failed to demonstrate any improvement in neurophysiological measures of DPN 24 months after simultaneous pancreas and kidney (SPK) transplantation in 61 type 1 diabetes mellitus (T1DM) patients. The Neurological Assessment of Thioctic Acid in Diabetic Neuropathy 1 (NATHAN-1) study [51], a 4-year multicenter randomized controlled trial of alpha lipoic acid demonstrated no benefit in neurophysiology, QST and DPN composite scores. However, Malik et al. [52] demonstrated an improvement in neurophysiology in normotensive patients with DPN and subsequently the Delapril and Manidipine for Nephroprotection in Diabetes (DEMAND) study [53] demonstrated a significant reduction in the odds ratios for DPN assessed by neurophysiology, QST, symptoms and signs, and autonomic dysfunction. A recent 52-week phase III trial [54] of weekly C-peptide replacement compared to placebo in 250 patients with T1DM did not show an improvement in electrophysiological variables. A surprising finding was that at the end of the trial, NCV improvement in the placebo treated group exceeded the gains observed in the active treatment group. This long list of failed clinical trials makes apparent that currently advocated endpoints of neuropathy lack the required sensitivity to capture treatment effects early and are in part responsible for the lack of U.S. Food and Drug Administration (FDA)-approved treatments for DPN.
Go to :
SKIN BIOPSY
Skin biopsy allows morphometric quantification of intra-epidermal nerve fibers (IENFs), expressed as the number of IENFs per length of section (IENF/mm). This technique has good reproducibility and an accurate quantification method has been established for assessing IENF pathology along with normative age-matched ranges [55]. There is an age- and sex-related decline in IENFD, but unlike neurophysiology it is not affected by weight and height [56]. The European Federation of Neurological Societies have published guidelines on its use in the diagnosis of peripheral neuropathies [57]. However, the diagnostic yield of skin biopsy depends on the reference and cutoff values selected and the definition of small fiber neuropathy.
Several studies have shown loss of IENFD in people with DM and IGT compared to healthy controls [58]. Therefore, the assessment of IENFD is a valid measure of diabetic neuropathy and may also be useful in predicting the development of clinical neuropathy [57]. A lower IENFD can identify early DPN and may be lower in people with painful as compared to painless DPN [59]. A recent study [60] showed a reduction in IENFD in patients with T2DM over 5 years, due to slower nerve regeneration in people with diabetes [61]. Narayanaswamy et al. [62] examined 29 patients with DPN and found that the annual rate of mean IENF loss was 3.76 fibers/mm. A 1-year diet and exercise intervention in people with IGT improved IENFD [63]. An inverse correlation also exists between IENFD and the severity of DPN defined on the basis of neuropathy disability and impairment scores. However, a recent study has demonstrated no correlation between IENFD and the neuropathy symptom score, but interestingly an inverse correlation with the severity of pain [64]. Alam et al. [65] has recently shown that IENFD has a diagnostic sensitivity of 0.61 and specificity of 0.80 for DPN. Because IENFD is considered to be the gold standard for the evaluation of small fiber neuropathy it has been advocated as a measure of treatment response in clinical trials. However, skin biopsy is an invasive technique, which requires experience and expertise to perform reliable IENFD staining with protein gene product 9.5 and subsequent quantification. The chance of bleeding and infection in DM patients also reduces its appeal as a diagnostic test for DPN and it therefore cannot be recommended in longitudinal and interventional studies. Furthermore, it has not been shown to be of value as a measure of therapeutic efficacy in a number of clinical trials in diabetic and human immunodeficiency virus (HIV) neuropathy [66].
Go to :
CORNEAL CONFOCAL MICROSCOPY
Corneal confocal microscopy (CCM) is a non-invasive and reiterative ophthalmic imaging technique, which allows in vivo examination of the cornea. The primary application of CCM was in the diagnosis and management of corneal disease. However, in the early 2000s two landmark studies by Rosenberg et al. [67] and Malik et al. [68] reported a progressive loss of corneal sub-basal nerve fibers in patients with increasing severity of DPN. Subsequently, multiple centers have confirmed these findings in different populations and the use of CCM to study DPN and neurodegeneration more broadly has grown exponentially [69].
Human corneal innervation
The cornea is one of the most densely innervated tissues of the human body receiving sensory innervation from the trigeminal ganglion. Myelinated nerve fiber bundles penetrate the peripheral limbal cornea and run towards the anterior central cornea where they terminate at the subbasal nerve plexus (SNP), a dense network of unmyelinated axons (19,000 to 44,000 axons within 90 mm2) equally distributed in the central and peripheral-central cornea. Previous studies [70] using electron-microscopy and immunohistochemistry have confirmed these nerve fibers to be C-fibers. Physiologically, corneal innervation plays an important role in the maintenance of a healthy ocular surface and in wound healing by regulating epithelial cell growth, proliferation and differentiation via the release of soluble growth factors, cytokines and neuropeptides such as substance P and calcitonin gene related peptide amongst others [71]. It is well established that corneal nerve dysfunction due to herpetic infections [72], trigeminal nerve lesions [73], neurosurgical injury [73], or intracranial disease [74] can result in neurotrophic keratitis. Indeed, neurotrophic corneal ulcers have been described in patients with DM as early as 1977 [75].
Image acquisition with CCM
The type of CCM used, i.e., white light or laser can significantly impact on the image acquisition process and quality. Over the last decade, the vast majority of research centers have utilized the laser CCM (Heidelberg Retina Tomograph III Rostock Corneal Module; Heidelberg Engineering GmbH, Heidelberg, Germany) due to its superior image quality and rapid scanning time. This CCM offers three modes to capture images namely: section, volume, and sequence. There is currently limited consensus on the optimal method to capture and analyze CCM images to assess the impact of DPN on corneal nerve morphology. In a healthy cornea the SNP is normally visible at 50 to 90 µm with a laser CCM. Section mode allows the examiner to capture images by manually focusing the field of view on the area of interest and may be more suitable for more experienced users. The other two modes, sequence and volume, allow the acquisition of sequential confocal images separated by 1 µm from a pre-specified area of the tissue. Most studies [76] have mostly analyzed five to eight high-quality, non-overlapping images from the central and peripheral-central cornea while others [77] have proposed that one ‘technically sound’ image offers adequate accuracy. A study by Vagenas et al. [78] showed that the selection of five to eight images was optimal to quantify corneal nerve morphology. Schaldemose et al. [79] described an objective method of randomly sampling and analyzing CCM images with the use of software which considers only in-focus nerves for quantification. They found small albeit significant differences when randomized sampling was used compared to human observer selection concluding that with the increased use of CCM worldwide a consensus on sampling is needed. One limitation of CCM is the small field of view (40×40) and some centers [80] have used wide field imaging techniques to produce maps of the SNP. Allgeier et al. [81] showed that an automated algorithm can create mosaics from the SNP within 145 seconds. However, the study population consisted of healthy controls and as the technique requires significant subject co-operation it poses a question regarding feasibility in morbid subjects. Although wide-field imaging allows an enhanced view of corneal nerve morphology it significantly prolongs the examination time, and indeed analysis of the composite image is highly laborious and has questionable added benefit. A recent study [82] estimated the nerve densities from the same participants using either three representative CCM images or wide field composite images and found no significant difference. The authors concluded that analysis of representative CCM images from a single scan provides adequate accuracy and could be used in clinical studies. Nevertheless, wide-field imaging could be more suitable for a research setting in order to study and characterize in detail the onset and extent of corneal nerve pathology in DPN while sampling of five to eight representative images may be the method of choice for a clinical setting.
CCM image quantification
The vast majority of studies have reported results from four morphological parameters namely corneal nerve fiber density (CNFD), corneal nerve branch density (CNBD), corneal nerve fiber length (CNFL), the tortuosity coefficient (TC) and more recently the inferior whorl length (IWL) [83]. CNFD refers to the total number of main nerve fibers in a CCM image (fibers/mm2), CNBD is defined as the number of branches connecting to the main nerve fiber (branches/mm2), CNFL is the sum of the length of all nerve fibers and branches in a CCM image (mm/mm2), and the TC is a unit-less measurement of the tortuosity of the main nerve fibers in a CCM image, independent of the orientation of the nerves. IWL is defined as the length of the nerves at the inferior whorl of the SNP, an anatomically distinct area where the nerves are arranged in a whorl like pattern. Other reported parameters include nerve fiber beading (number/100 µm) [84], corneal nerve connection points and average weighted corneal nerve fiber thickness which essentially measures nerve fiber width [85]. Nerve fiber area may be optimal for detecting change in clinical trials of new therapeutics [86]. A recent study proposed that the novel parameter of corneal nerve fractal dimension analysis, a measurement of morphological complexity, could be a useful and highly sensitive parameter to assess neurodegeneration in T1DM [87]. The vast majority of studies report results using either CCMetrics or ImageJ (https://imagej.nih.gov/ij/download.html). CCMetrics is a software capable of manual and fully automated analysis, which has been specifically designed and validated for CCM corneal nerve quantification [76]. ImageJ is a more generic software widely used for image processing and its usability for quantifying nerve morphology can be extended with the use of purpose-built plugins such as NeuronJ [88]. Recently, two novel algorithms for fully automated tracing of corneal nerve density [89] and length [90] in wide-field mosaics have been described but their performance is yet to be validated in larger studies. DPN may also induce clustering of corneal nerve fibers compared to the equally distributed nerve fibers in the healthy cornea. Spatial pattern analysis of CCM mosaics, an advanced computing method which allows the estimation of corneal nerve branching points, has been found to improve the detection of corneal nerve loss when used in combination with conventional measures of nerve morphometry [91].
CCM in diabetic peripheral neuropathy
Reduced corneal sensation in diabetes as a result of polyneuropathy was reported as early as 1974 [92]. Schwartz [92] first studied corneal sensitivity in a group of 44 patients with DM and found significantly reduced sensation in clinically normal corneas which was symmetrical, occurred early and was related to disease duration. Another study [75] reported the occurrence of treatment-resistant neurotrophic corneal ulcers in young patients with T1DM. Both studies did not report the DPN status in the study population. In the early 2000s, Rosenberg et al. [67] showed subbasal nerve alterations using CCM in patients with clinically confirmed DPN and Malik et al. [68] showed that the severity of corneal nerve pathology was related to DPN severity.
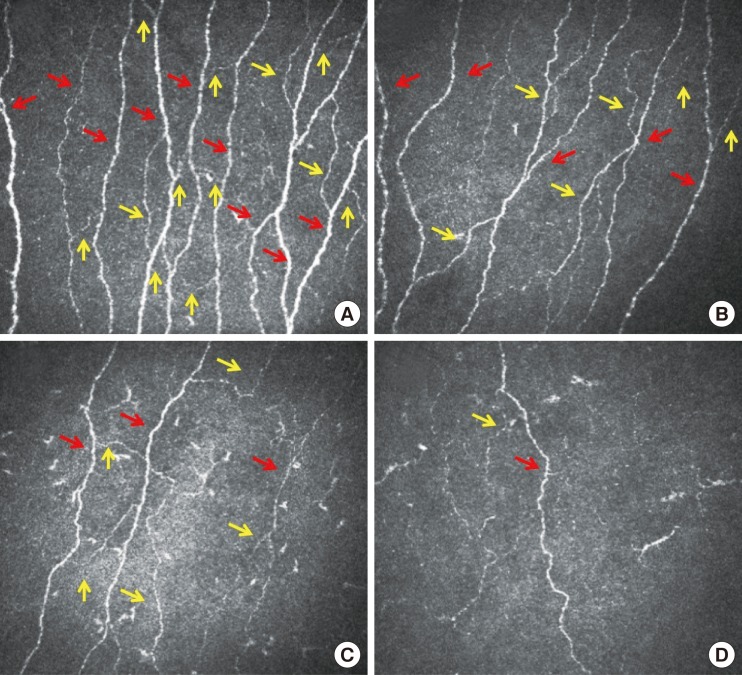
We, and others have shown that CCM can be used to detect early corneal nerve alterations [8093] with excellent reproducibility between examiners, occasions and quantification methods (Fig. 1) [9495969798]. We have established a multinational normative reference database for corneal nerve morphology [99] and shown that healthy individuals exhibit morphometric stability over time [100]. CNFD significantly correlates with IENFD and QST while corneal and IENF length can differentiate patients with and without painful neuropathy [93]. These results were not confirmed by an independent study employing CCM and IENFD, which reported a patchy pattern of loss between the cornea and skin, suggesting that the exact temporal relationship needed further clarification [80]. However, studies have demonstrated that CCM has comparable diagnostic performance to IENFD with the advantage that it is rapid and non-invasive compared to skin punch biopsy [65]. CNFL has a high sensitivity (91%) and specificity (93%) [77] for the diagnosis of DPN and cardiac autonomic neuropathy [84101] and a reduced CNFD or CNFL are associated with an odds ratio for DPN of 16.5 and 12.9, respectively [76]. A recent study has also shown that reduced corneal innervation is associated with erectile dysfunction [102]. IWL reduction is more prominent in patients with painful neuropathy [103] and its evaluation improves the diagnostic performance of CCM compared to central CNFL, indicating a dying back neuropathy; whilst its distinct morphology could make it an ideal anatomical location for reproducible follow-up assessments [103] in longitudinal studies and particularly in clinical trials [83]. Subtle, albeit significant alterations have been reported even in normoglycemic subjects with elevated glycosylated hemoglobin (HbA1c) indicating the ability of CCM to detect subclinical axonal degeneration [104]. A shorter CNFL is associated with functional deficits in cold detection threshold, laser Doppler image flare, and heart rate variability [105] and corneal nerve alterations precede overt diabetic retinopathy and microalbuminuria [106], which has significant implications for the screening of microvascular complications. A recent study shows significant corneal nerve fiber changes in pediatric T1DM patients, along with thinning of the retinal nerve fiber layer [107].
A higher HbA1c and lower high density lipoprotein cholesterol impact on subbasal nerve morphology [83] and it has been shown to improve with treatment of glycaemia, blood pressure, and lipids [108] as well as in patients with T1DM on continuous subcutaneous insulin [109]. In the most dramatic example of curing diabetes with a SPK transplantation, CCM was able to detect significant corneal nerve regeneration 12 months after transplantation without an improvement in IENFD, QST, and NCV [110]. Hence CCM can detect early nerve fiber repair, missed by currently advocated measures of DPN. Indeed, recent phase 2 clinical trials have used CCM as a primary co-endpoint to show the efficacy of ARA-290, a novel first-in-class peptide [111] in patients with sarcoidosis-related neuropathy [112113] and T2DM [114]. Daily subcutaneous administration of ARA-290 over 28 days compared to placebo was associated with a significant improvement in CNFD along with an improvement in cutaneous temperature sensitivity and exercise capacity [112]. In a subsequent phase 2b randomized control study, improvement in corneal nerve morphology was strongly correlated with the expression of GAP-43+ IENF, indicating neuronal repair, and an improvement in pain intensity after 28 days [113]. In a pilot trial of seal oil omega-3 polyunsaturated fatty acids supplementation in patients with T1DM over 12 months showed a 29% increase in CNFL, a primary outcome, with no change in the secondary outcomes of NCV and sensory function [115]. Interestingly, a recent trial in T2DM rats showed that a combination therapy of Menhaden oil, alpha lipoic acid, and enalapril for 12-week was most effective for showing an improvement in the primary outcomes of corneal nerve density and sensitivity [116]. The case for inclusion of CCM as an outcome marker for trials of neuropathy is compelling.
Results from longitudinal studies suggest that CCM has prognostic value. Pritchard et al. [117] reported that the 4-year incidence of DPN amongst non-neuropathic patients with T1DM was 18% and was associated with a lower baseline CNFL, longer diabetes duration, higher triglycerides, worsening retinopathy and nephropathy, impaired sensation to temperature and vibration and slower peroneal and sural nerve conduction velocities. Lovblom et al. [118] reported a 17% incidence of DPN in patients with T1DM followed over approximately 4 years, and a baseline CNFL of <14.9 mm/mm2 was the strongest predictor of new onset DPN. Another prospective study [58119] in subjects with IGT showed that lower baseline CNFD, CNBD, CNFL and mean dendritic length of IENF were the strongest predictors of progression to T2DM. Remarkably, those subjects who returned to normoglycaemia showed a small but significant improvement in their CCM parameters while IENFD continued to decline during the same period of time. The NIH CCM consortium study is an international pooled multi-center analysis to assess the diagnostic validity and determine diagnostic thresholds for identification of DPN by CCM. Early results from 516 participants have shown that measurement of CNFL has high sensitivity and specificity for the detection of DPN and support the implementation of CCM in trials of neuropathy [120]. A recent meta-analysis by Jiang et al. [69] of 13 studies in 1,680 subjects, independently confirmed CNFD, CNFL, and CNBD to be the best parameters to differentiate patients with and without DPN compared to healthy controls.
CCM beyond diabetic neuropathy
While there is strong evidence to support the utility of CCM in DPN, multiple studies suggest that CCM could also be used to characterize the extent of axonal injury in many other peripheral neuropathies and central neurodegenerative disorders. We and others have reported corneal nerve alterations in Charcot-Marie-Tooth disease type 1A [121], HIV sensory neuropathy [122], idiopathic small fiber neuropathy [123], Fabry' disease [124], chronic inflammatory demyelinating polyneuropathy [125], chemotherapy induced peripheral neuropathy [126], chronic migraine [127], Parkinson's disease [128], amyotrophic lateral sclerosis [129], stroke [130], and multiple sclerosis [131132133]. Importantly, in most of these studies corneal nerve alterations were associated with clinical and neurological disability and functional outcomes, suggesting that corneal subbasal innervation is a highly sensitive and accessible site to assess neurodegeneration.
Go to :
CONCLUSIONS
DPN is a serious and underdiagnosed complication of diabetes of multifactorial etiology. Currently advocated endpoints of neuropathy lack sensitivity to capture early abnormalities before overt neuropathy has developed, are invasive or have repeatedly failed as surrogate end-points of therapeutic efficacy in clinical trials of DPN. CCM has emerged as a powerful diagnostic tool for the detection of small fiber neuropathy, the earliest manifestation of DPN, and has shown prognostic utility in identifying those who develop clinical DPN as well as showing remarkable consistency demonstrating early nerve regeneration in a number of clinical trials. Given the rapid and non-invasive methodology and automated quantification it allows community level screening of DPN, similar to digital retinal photography for diabetic retinopathy.
Go to :
 XML Download
XML Download