

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Evaluation of individuals who present with acute chest pain, or other clinical features suggestive of acute coronary syndrome (ACS), is often a clinical challenge. Biomarkers reflecting distinct pathophysiological features have become fundamental tools for improvement of traditional diagnostic and risk-stratification methods for patients with ACS [123]. Multi-marker strategies employing biomarkers from different pathological pathways can contribute to successful methodologies [4]. Troponin I, N-terminal pro-B type natriuretic peptide (NT-proBNP), and high-sensitivity C-reactive protein (hs-CRP) are biomarkers for which consistent and reliable data are available on their diagnostic and prognostic values for ACS [56]. Evidence also suggests that proprotein convertase subtilisin/kexin type 9 (PCSK9) could have value as a potential biomarker for ACS [7].
PCSK9 is a liver-derived circulating protein that has an important role in the homeostasis of low density lipoprotein (LDL) via enhancement of degradation of the LDL receptor; thereby, reducing clearance of LDL-cholesterol (LDL-C) [8]. PCSK9 loss-of-function mutations are associated with reductions in circulating levels of LDL-C and in the risk of coronary heart disease [9]. Therefore, PCSK9 has received considerable attention as a promising target for lipid-lowering therapy [10]. A high plasma level of LDL-C is a major risk factor for cardiovascular diseases, including ACS, and results from genetic, experimental, and epidemiological studies show clear associations between PCSK9 function and cardiovascular risk [111213]. Moreover, levels of PCSK9 are driven up by cardiac ischemia during ACS events and may contribute to plaque vulnerability in coronary vessels [14]. Evidence suggests that PCSK9 antibodies have a potential role in the management of ACS. However, no data are available on the predictive value of serum PCSK9 concentrations for coronary angiographic severity.
In this study, our aim was to investigate whether a high level of serum PCSK9 is associated with a high risk and severity of ACS in individuals with coronary angiographic lesions. We also assessed the association of serum PCSK9 levels with SYNTAX (SYNergy between percutaneous coronary intervention with [paclitaxel-eluting] TAXUS stent and cardiac surgery) and GRACE (Global Registry of Acute Coronary Events) scores, which are indicators of the severity of coronary artery occlusion.
METHODS
Study population and data collection
A retrospective, cross-sectional, observational study was conducted involving individuals who attended the Kyungpook National University Hospital from December 2009 to July 2012. Screening involved 444 individuals with suspected ACS, including unstable angina and both ST-segment elevation myocardial infarction and non-ST-segment elevation myocardial infarction. Exclusion criteria were as follows: use of lipid-lowering drugs (statins, fibrates, nicotinic acid, or ezetimibe) within 3 months; infectious or systematic inflammatory diseases, significant hematological disorders, thyroid dysfunction, and severe hepatic and/or renal insufficiency; and female sex. The final study population consisted of 121 individuals, 100 of whom had one or more narrowing lesions of the coronary arteries (with ≥50% stenosis) on coronary angiography (CAG), and 21 of whom had no such lesions. The study protocol was approved by the Institutional Review Board of Kyungpook National University Hospital (IRB no.: 2015-10-019-001), and all subjects provided written informed consent before participation in the study.
Measurements of clinical and laboratory parameters
Details of age, sex, body mass index (BMI), past history of diabetes and hypertension, history of tobacco smoking, and familial history of ACS were retrospectively collected from electronic medical records. Laboratory data were acquired on the day of admission, before the CAG procedure. Serum levels of NT-proBNP were measured by an electrochemiluminescence immunoassay method (Modular Analytics E170; Roche Diagnostics, Mannheim, Germany). Other biochemical variables were measured by standard laboratory techniques. Levels of serum total cholesterol, high density lipoprotein cholesterol (HDL-C), LDL-C, triglycerides, hs-CRP, creatinine, white blood cells, aspartate transaminase, and alanine transaminase were determined from blood samples collected after an overnight fast (of ≥8 hours).
Measurement of PCSK9
Blood samples were collected into EDTA (ethylenediaminetetraacetic acid)-containing tubes in the morning after an overnight fast (of ≥8 hours), and centrifuged at 3,000 rpm for 10 minutes at 4℃ to obtain serum. All the samples for the measurement of PCSK9 levels were stored at −80℃ until analysis. Serum PCSK9 levels were measured in duplicate by enzyme-linked immunosorbent assay with a commercial kit (R&D Systems, Minneapolis, MN, USA) according to the manufacturer's instructions, with a 1:1 dilution of samples in dilution buffer before the assay.
Measurement of the severity of coronary artery occlusion
The severity of coronary artery occlusion was evaluated by calculation of SYNTAX scores and GRACE scores. The detailed methodologies for calculating these scores have been described elsewhere.
SYNTAX score
SYNTAX is an anatomically based scoring system that quantitatively characterizes coronary vessels according to the number, complexity, location, and functional aspect of obstructive lesions on CAG. Vessels with diameters >1.5 mm that contain lesions with stenosis diameters ≥50% are assessed. Each coronary segment is given a weight factor that is determined by the lesion location and severity. Lesion characteristics, including total occlusion, trifurcation, bifurcation, calcification, tortuosity, length >20 mm, thrombus, and diffuse or small-vessel disease, are combined to give a final score via the SYNTAX calculator (www.syntaxscore.com). The SYNTAX score is an objective angiography-based tool for grading of the complexity and severity of coronary artery disease (CAD).
GRACE risk score
The GRACE score is a prognostic risk-assessment tool for use in patients with ACS. Calculation of the score takes account of age, Killip class, systolic blood pressure, ST-segment deviation, cardiac arrest during presentation, serum creatinine levels, heart rate, and elevated cardiac enzyme or marker levels. An online calculator is used for derivation of GRACE scores (http://www.outcomes-umassmed.org/grace).
Statistical analysis
Continuous variables are presented as the mean±standard deviation, and categorical variables are presented as the frequencies (and percentages) in each category. Student t-tests were used for comparison of the means of continuous variables and chi-square tests were used for comparison of the distributions of categorical variables. Analysis of covariance was used for identification of differences in serum levels of PCSK9 in groups of patients with different numbers of involved coronary arteries. The models were adjusted for age, BMI, past history of diabetes and hypertension, smoking, and familial history of ACS. The study population was divided into tertiles according to serum levels of PCSK9. Multivariable logistic regression models were used for calculation of the odds ratios (ORs) for the presence of one or more coronary angiographic lesions in patients in tertile 2 (T2) and tertile 3 (T3) compared with tertile 1 (T1). The models were also adjusted for multiple confounding factors. Multivariable linear regression models were applied for characterization of the association between serum levels of PCSK9 and SYNTAX and GRACE scores. Results of statistical tests were considered significant for P<0.05. Statistical analysis was performed with SPSS version 18.0 software (SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics
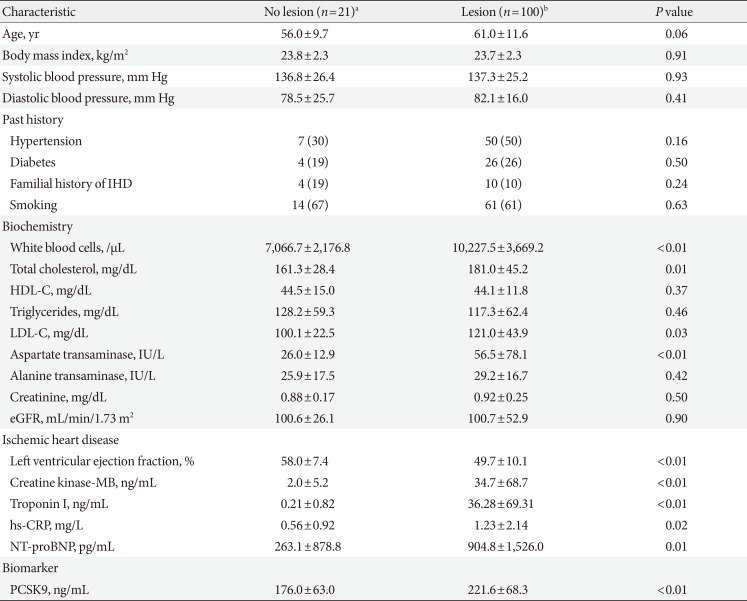
The baseline characteristics of study participants are shown in Table 1. The means or frequencies of age, BMI, HDL-C, triglycerides, creatinine, systolic and diastolic pressure, past history of hypertension and diabetes, familial history of ACS, and history of tobacco smoking showed no significant differences between patients with no CAG lesions (n=21) and those with lesions (n=100). Mean levels of total cholesterol and LDL-C were significantly higher in patients with CAG lesions than in those without lesions. Levels of white blood cells, aspartate transaminase, creatine kinase-MB, troponin I, hs-CRP, and NT-proBNP were significantly higher (as a result of cardiac damage) in patients with CAG lesions than in those without lesions. Serum levels of PCSK9 were significantly higher in patients with CAG lesions than in those without CAG lesions.
Baseline characteristics in tertiles stratified by levels of PCSK9
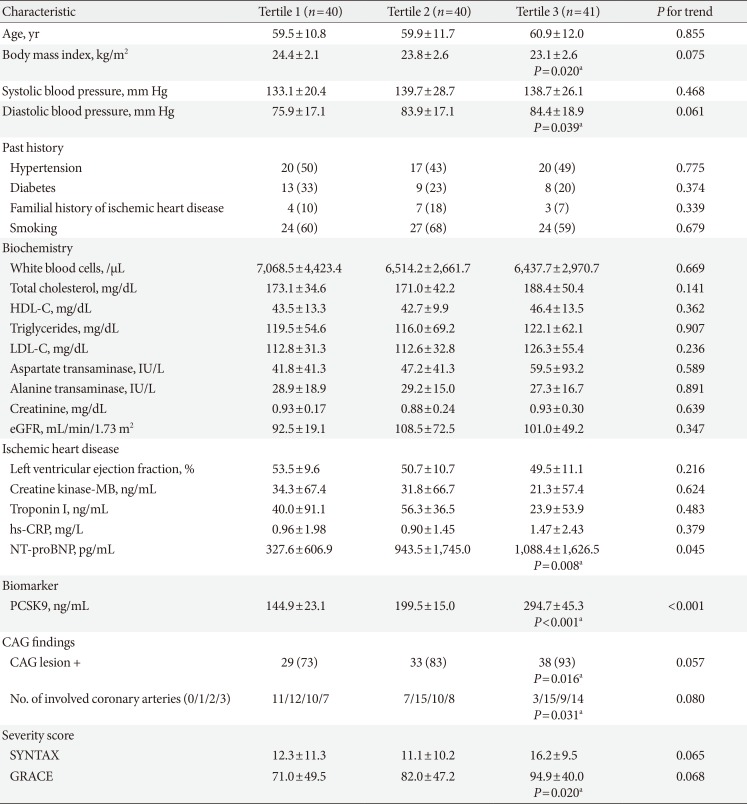
To assess the associations between serum levels of PCSK9 and different variables related to ACS, we stratified the study population into tertiles according to PCSK9 levels (Table 2). With the exception of NT-proBNP (and PCSK9), the baseline characteristics did not show statistical trends related to PCSK9 stratification. However, in comparisons of T1 with T3, proBNP, positive findings of CAG lesions, the number of involved coronary arteries, and GRACE scores were all significantly higher in T3 than in T1, whereas diastolic blood pressure was significantly lower in T3 than in T1. Although LDL-C levels and SYNTAX scores showed numerical increases from T1 to T3, statistical significance was not observed.
Association between PCSK9 levels and the occurrence of CAG lesions
The proportion of individuals with CAG lesions was significantly higher in T3 than in T1 (unadjusted OR, 4.805; 95% confidence interval [CI], 1.227 to 18.814; P=0.024) (Table 3). The difference between T3 and T1 was enhanced by adjustment for age, BMI, past history of diabetes and hypertension, smoking, and familial history of ACS (OR, 7.468; 95% CI, 1.582 to 35.249; P=0.011). The P for trend of increasing proportions of individuals with CAG lesions from T1 to T3 were significant (P=0.009 for the adjusted model 2).
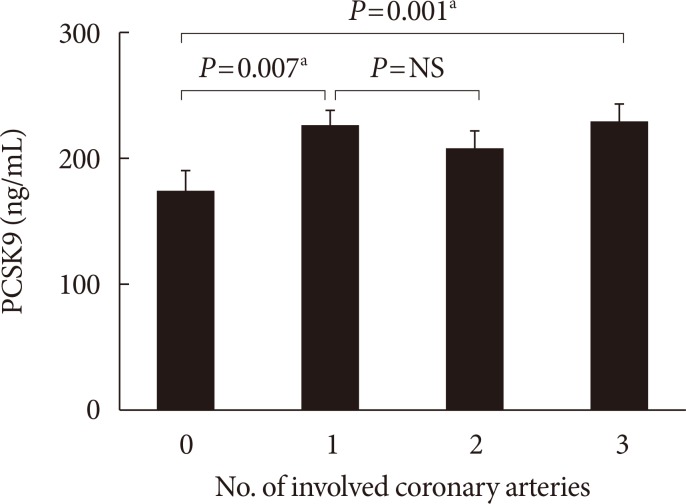
Associations between serum PCSK9 concentrations and numbers of involved coronary arteries
Serum levels of PCSK9 were measured in 121 patients who were assessed for coronary angiographic lesions. Mean PCSK9 levels in patients with 0 (n=21), 1 (n=42), 2 (n=29), and 3 (n=29) involved arteries were compared by analysis of covariance. After adjustment for age, BMI, past history of diabetes and hypertension, smoking, and familial history of ACS, individuals with one or more coronary artery lesions had significantly higher mean serum PCSK9 levels than individuals without coronary artery lesions (Fig. 1).
Associations between PCSK9 levels and scores indicating the severity of coronary artery occlusion
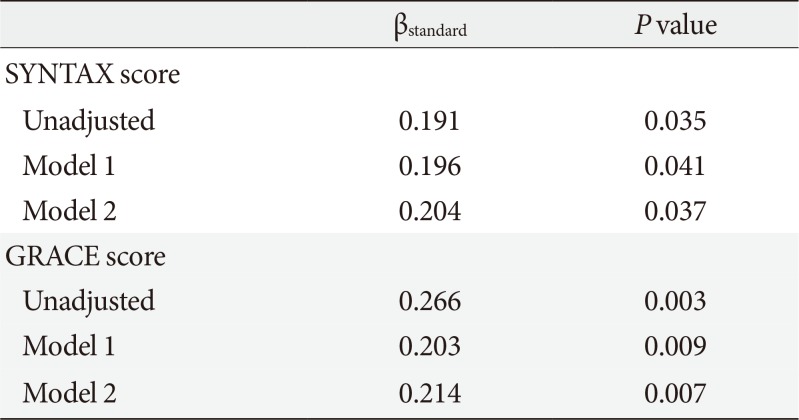
Multivariable linear regression models revealed that the serum PCSK9 concentration was positively associated with the SYNTAX score, which is an angiographic grading tool to determine the complexity of CAD (βstandard=0.191; P=0.035) (Table 4). The GRACE risk score, which is a risk-prediction tool for use in patients with ACS, was also significantly associated with PCSK9 concentrations (βstandard=0.266; P=0.003). Furthermore, after adjusting for age, BMI, past history of diabetes and hypertension, smoking, and familial history of ACS, PCSK9 levels were still positively correlated with SYNTAX scores (βstandard=0.204; P=0.037) and GRACE scores (βstandard=0.214; P=0.007).
DISCUSSION
In this study, we demonstrated that serum PCSK9 concentrations were significantly associated with the proportions of patients with CAG lesions. This association was still significant after adjustment for multiple variables. In addition, we found that PCSK9 levels were significantly associated with the number of affected coronary arteries, SYNTAX scores, and GRACE scores.
Evidence suggests that circulating PCSK9 levels are associated with the incidence of CAD [121314]. In one study involving patients who were not receiving treatment with statins or fibrates at the time of recruitment, higher serum PCSK9 levels were seen in one group of patients with angiographic CAD including ACS (385.0±146.9 ng/mL) than in controls without CAD (340.4±125.2 ng/mL, P<0.001) [15]. However, there was no association of PCSK9 with the number of lesions in the Ottawa group of participants [15]. In a prospective cohort study of 4,232 men and women 60 years-of-age at the time of recruitment, baseline serum levels of PCSK9 were associated with future risk of cardiovascular disease, even after adjustment for established risk factors [16]. In a study involving 2,030 patients with ACS undergoing CAG, mean levels of serum PCSK9 were found to increase over time [7]. In our study population, serum PCSK9 levels were positively associated with the proportion of patients with CAG lesions, and this association was still significant after adjustment for multiple variables. Our results, therefore, contribute to the evidence of a relationship between circulating PCSK9 levels and the development and progress of CAD including ACS.
It is well known that PCSK9 decreases hepatic clearance of plasma LDL-C by degrading the LDL receptor. Although plasma PCSK9 levels are associated with the abundance of the LDL receptor in hepatocytes, it is not clear whether its levels directly reflect LDL receptor activity. Recent several studies demonstrated the direct effects of PCSK9 on vascular cells [141718]. High circulating PCSK9 levels are associated with inflammation, a higher amount of necrotic component in coronary plaque, and a higher thrombotic substrate level, suggesting that circulating PCSK9 levels are associated with the severity of anatomical vascular disease, as measured by angiography [14]. Moreover, mitochondrial reactive oxygen species, generated during stressful states, may be an importance initiator of PCSK9 expression in vascular cells [1718]. Therefore, it is possible that PCSK9 has a direct role in the development of atherosclerosis. To our knowledge, our study is the first to characterize the association of serum PCSK9 concentrations with coronary angiographic severity using SYNTAX scoring system, and show the definite association between PCSK9 levels and coronary angiographic severity. Nonetheless, the prognostic value of the PCSK9 level in patients with ACS has not yet been conclusively demonstrated, and further investigation will be needed to compare PCSK9 and other prognostic biomarkers of CAD.
The present study has several limitations. First, this study is a retrospective and cross-sectional study. Therefore, causal relationship between PCSK9 and CAG finding could not be determined. Second, relatively small number of participants reduced the clarity of the results in our study. Third, to exclude variable hormonal effect, we only included male participants. This did not show the utility of PCSK9 in general population.
In conclusion, we found that high serum PCSK9 levels were associated with high proportions of patients with CAG lesions. Moreover, in our population, PCSK9 concentrations were associated with SYNTAX and GRACE scores. Large-scale, prospective studies will be required to validate our findings and determine the potential utility of PCSK9 measurements in routine clinical practice.

 XML Download
XML Download