

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The global prevalence of overweight and obesity has increased dramatically over the past several decades. The World Health Organization estimated that in 2014 more than 1.9 billion adults worldwide were overweight (39%), defined as a body mass index (BMI) of 25.0 to 29.9 kg/m2, and 600 million adults were obese (13%) (BMI ≥30 kg/m2) [1]. Overweight and obesity are established risk factors for the development of metabolic diseases such as diabetes, hypertension, dyslipidemia, cardiovascular disease, and certain cancers [2]. Nevertheless, the association between overweight/obesity and mortality remains an area of interest, importance, and debate. Some previous research has shown a U- or J-shaped association between BMI and mortality, with higher mortality in underweight or obese subjects [34]. On the contrary, reviews of other research have demonstrated that adults with a higher BMI have lower mortality compared with leaner individuals in population-based samples with various clinical conditions [56]. The lower mortality seen in overweight and obese persons presents a paradox given that greater adiposity is associated with higher risk of multiple chronic conditions associated with a shorter lifespan, and, in particular, type 2 diabetes mellitus.
Obesity is closely linked with the etiology of type 2 diabetes mellitus. Previous research has shown that the relative risk for overweight (25.0≤BMI≤29.9 kg/m2) adults to develop type 2 diabetes mellitus is 4.6-fold for women and 3.5-fold for men compared with their normal weight (18.5≤BMI≤24.9 kg/m2) same sex peers [7]. A Japanese study demonstrated that an increase in BMI of 1 kg/m2 (corresponding to a body weight gain of 2.4 to 2.9 kg) may increase the risk of diabetes by 25% [8]. In addition, weight reduction achieved through a hypocaloric diet or bariatric surgery increases the probability of remission from type 2 diabetes mellitus [910]. Furthermore, a lifestyle intervention has been shown to prevent the development of type 2 diabetes mellitus in overweight persons at high risk for this outcome, with weight loss being the dominant predictor of reduced diabetes risk [11]. However, as for the association between BMI and longevity, the predominant evidence from longitudinal observational studies implies that overweight or obese individuals with diabetes have lower mortality compared with normal weight individuals [6]. We reviewed the literature for research on the obesity paradox in type 2 diabetes mellitus to determine how consistently this has been observed and to discuss potential causal and non-causal explanations for this phenomenon.
CLINICAL STUDIES SUPPORTING THE OBESITY PARADOX IN DIABETES
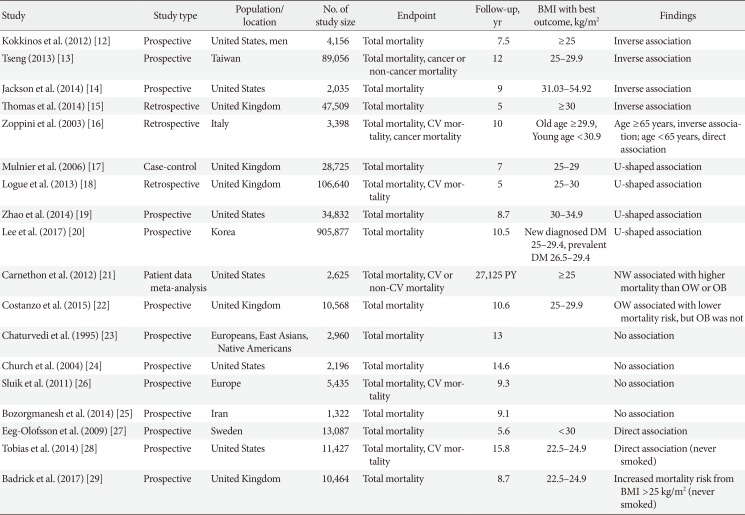
We identified 17 studies investigating the association between obesity defined by BMI and mortality in diabetes that included more than 1,000 subjects who were followed for more than 4 years (Table 1). Eleven studies showed that being overweight or obesity was associated with lower mortality rate. Four studies reported an inverse relationship between BMI and mortality rate [12131415]. Among men with diabetes from Veterans Affairs medical centers, normal weight subjects had a higher mortality than those with class II obesity (BMI ≥35 kg/m2) [12]. Tseng [13] showed BMI was inversely associated with all cause and cancer or diabetes complication mortality in Taiwanese patients with type 2 diabetes mellitus. Zoppini et al. [16] found that the relationship between body weight and mortality varied by age. In older type 2 diabetes mellitus patients (age ≥65 years), the highest BMI quartile (≥29.9 kg/m2) was associated with lowest all-cause mortality. By contrast, among those <65 years, the highest BMI quartile (≥30.9 kg/m2) had a significantly higher mortality compared to patients in the lowest BMI quartile (≤25.4 kg/m2).
Four studies showed a U-shaped association between mortality and BMI [17181920]. Mulnier et al. [17] reported those with a BMI 15 to 19 or ≥30 kg/m2 had an increased risk of mortality compared with a BMI 20 to 24 kg/m2 in a cohort of British patients with diabetes but no significant mortality risk difference was seen in those with a BMI 25 to 29 kg/m2 compared to 20 to 24 kg/m2. When Logue et al. [18] retrospectively examined subjects within a year of diagnosis of type 2 diabetes mellitus in Scotland, patients with normal weight (20 to <25 kg/m2) or obese (≥35 kg/m2) exhibited higher mortality compared with the overweight group. The U-shaped association between BMI and mortality was also seen among black and white patients with type 2 diabetes mellitus, with obese patients generally at lowest risk of death compared to both normal weight and overweight patients [19]. In the largest study to date that contained nearly 900,000 participants with previously diagnosed or newly diagnosed diabetes based on fasting glucose measurement, Lee et al. [20] also observed a U-shaped association between BMI and mortality in Korean diabetes patients, with lowest mortality between 25.0 to 30.9 kg/m2 depending on sex and new or previously diagnosed diabetes status. Carnethon et al. [21] reported a 2-fold higher all-cause mortality rate in normal weight subjects with new-onset diabetes compared with overweight or obese adults in an analysis of pooled data from five longitudinal cohort studies. Costanzo et al. [22] also showed that the optimal BMI for survival in a British cohort of patients with type 2 diabetes mellitus followed for a median of 10.6 years was 25.0 to 29.9 kg/m2 compared to normal weight or obese BMI categories.
CLINICAL STUDIES AGAINST THE OBESITY PARADOX IN DIABETES
The majority of published research provides evidence favoring the existence of an obesity paradox in type 2 diabetes mellitus. The authors of a number of studies, though, conclude that their results do not support this finding or can be explained by other factors. Chaturvedi and Fuller [23] examined mortality in a population of persons with diabetes from Europe, East Asia, and Native North Americans, but found no clear association between BMI and mortality risk. Although this study included 2,960 diabetic participants, the analysis was subdivided into three groups based on the population sampled, and different BMI cutpoints were used to define excess adiposity. The reduction in power due to such stratification may have resulted in the null findings regarding the association between BMI and mortality. Church et al. [24] observed a higher mortality risk among diabetic obese men (≥30 kg/m2) that disappeared after adjustment for fitness. Bozorgmanesh et al. [25] report that there is no obesity paradox in their population of 1,322 new-onset diabetic patients after adjustment for waist and hip circumference, but Fig. 2D of Bozorgmanesh et al. [25] showing mortality risk by BMI suggests a nadir in the overweight range, which may not have reached significance due to the relatively smaller sample size of this population. Although Sluik et al. [26] conclude that they observed no associations between BMI and mortality in their cohort of European diabetic participants followed for a median of 9.3 years, the results presented in Table 2 of Sluik et al. [26] show a significantly lower mortality risk in men with BMI 25.0 kg/m2 or greater in models adjusted for waist/height ratio, supporting the existence of the obesity paradox. We conclude that these “negative” studies do not convincingly refute the existence of the obesity paradox in type 2 diabetes mellitus.
In addition, two studies observed a direct relationship between BMI and mortality in subjects with diabetes. Eeg-Olofsson et al. [27] reported that the relative risk of total mortality for a 5-unit increase in BMI was 27% in a cohort of 13,087 diabetic participants followed for 6 years. But in this population, there was no significant difference in mortality risk comparing overweight (BMI 25.0 to 29.9 kg/m2) to normal weight participants [27]. In the Nurses' Health Study and Health Professionals Follow-up Study, Tobias et al. [28] found that a J-shaped association between BMI and mortality among all type 2 diabetes mellitus patients and among those who had ever smoked and a direct linear relationship among those who had never smoked suggesting that effect modification by smoking status acts in this association. Furthermore, there was no evidence of lower mortality among diabetes patients who were overweight or obese compared to those with normal weight in this study of health professional populations, whose weight and height were assessed shortly before diagnosis, thereby limiting potential bias due to reverse causation [28]. A prospective study of 10,464 individuals with newly diagnosed diabetes in the United Kingdom and approximately three controls per diabetic case showed no evidence of the obesity paradox in never smokers, but did see a lower mortality risk in ever smokers with BMI between 25.0 to 34.9 kg/m2 [29]. Lastly, a large prospective Swedish study examined mortality in diabetic patients compared to controls within BMI strata, but did not compare mortality within the diabetic population only by degree of adiposity [30]. Therefore, the results of this paper do not directly pertain to this overview that has focused on the role of obesity as a predictor of mortality in diabetes only.
POSSIBLE EXPLANATIONS FOR THE OBESITY PARADOX IN DIABETES
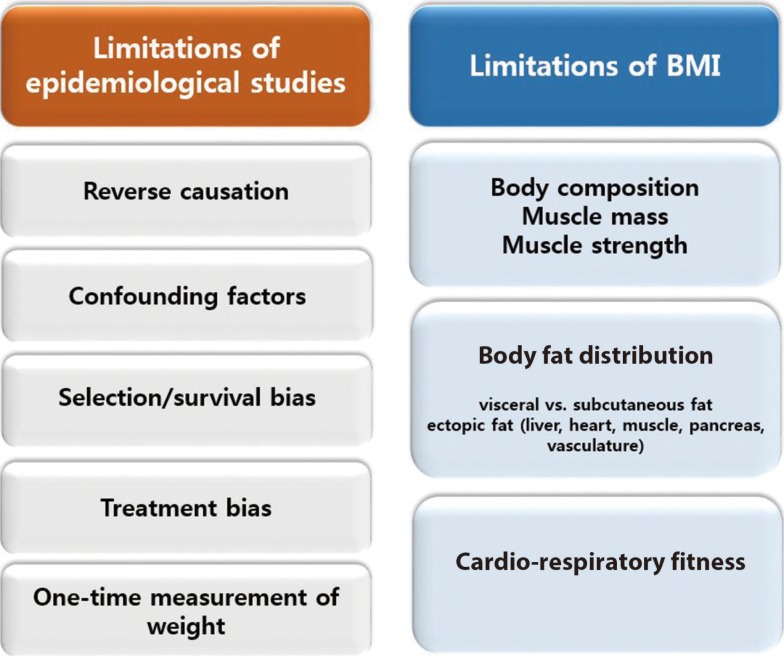
Associations observed in epidemiologic and clinical research may arise due to causation but also for many other reasons. We explore further potential mechanisms that explain the obesity paradox in diabetes by focusing on limitations in study design, the validity of BMI as an indicator of adiposity, and the value of BMI to reflect other important features of body composition.
Limitations of previous epidemiological studies
Discordant findings in observational research can often be attributed to population differences, study design issues, and measures taken to reduce and/or control for bias. Specific issues pertinent to the understanding of the obesity paradox are shown in Fig. 1 and discussed further below.
Reverse causation
Reverse causation refers to the outcome causing a change in the exposure instead of the other way around. If the onset of diabetes resulted in a change in body weight such that more severe disease resulted in weight loss, then this would result in an association between lower body weight/BMI and a higher rate of complications or mortality. Much of the research on the obesity paradox in diabetes measured body composition well beyond the onset of diabetes and therefore may be susceptible to reverse causation bias. A notable exception is the study of two populations of health professionals, which included measurements of body weight and height from before diabetes diagnosis in incident cases [28], finding no evidence of the obesity paradox. To mitigate reverse causation by chronic disease induced weight loss, analyses should consider exclusion of patients with major illnesses (cancer, cardiovascular disease, pulmonary disease) at baseline or who died early during follow-up.
Confounding factors
These are factors that are associated with the exposure (BMI) and the outcome (mortality), such as smoking and occult or preexisting chronic disease that lead to both lower BMI and higher mortality risk [9]. Preston and Stokes noted the absence of the obesity paradox among nonsmoking participants of National Health and Nutrition Examination Survey (NHANES) III and NHANES 1999 to 2004 with dysglycemia (glycosylated hemoglobin ≥5.7%) or prior diagnosis of diabetes, and concluded that higher mortality in normal diabetes participants can be explained by the strong inverse correlation between obesity and smoking [31]. Other factors that attenuated the obesity paradox after adjustment include fitness and waist and hip measurements reflecting body composition [2425].
Selection/survival bias
Patients who develop type 2 diabetes mellitus in the absence of overweight or obesity may have more severe disease or higher mortality risk or both due to genetic susceptibility or the presence of other risk factors for adverse outcomes and a higher mortality rate independent of body composition [3233]. Thinner diabetes patients in the United Kingdom with BMI <25 kg/m2 were more likely to be treated with insulin than their heavier counterparts [1727]. Insulin use has been associated with higher risk of adverse outcomes in patients with diabetes, such as, for example, hospitalizations, foot ulcer, and mortality [3435], and may therefore reflect greater diabetes severity. Lajous et al. [36] examined the outcomes of incident diabetes and mortality in a cohort of 88,373 French women followed for a mean of 16.7 years, and noted lower mortality associated with an overweight or obese BMI in those with diabetes, but higher mortality with the same BMI elevation in women without diabetes. The authors concluded through an analysis of casual diagrams that the apparent better survival with greater BMI among the diabetic women could be explained by selection of persons with diabetes only for assessment of the effect of obesity on mortality since risk of diabetes is affected by the exposure (obesity). They advised against assessing the effects of adiposity on mortality in persons with a disease (diabetes) for which excess adiposity is a risk factor. Badrick et al. [29], however, noted the obesity paradox among not only diabetic participants who smoked, but also non-diabetic participants, and concluded that the selection factors (bias) do not explain this phenomenon. Greater BMI was associated with better survival among older (≥65 years) patients with diabetes in two studies [1637], suggesting that selective survival may account for the obesity paradox if patients with unhealthy obesity do not survive into old age, while those with a more healthy obesity phenotype do, and comprise a biased comparison group for evaluation of mortality differences with normal weight diabetic patients [38].
Treatment bias
Anti-diabetic medication and behavioral therapy (i.e., diet and physical activity changes) may result in weight loss. We speculate that obese patients may be diagnosed earlier with diabetes resulting in earlier initiation of treatment and potentially few diabetic and cardiovascular complications, leading to improved survival.
One-time measurement of weight
Weight measurement only once at baseline may not reflect a person's weight history. In a recent report that included the Nurses' Health Study I and II and the Health Professionals Follow-Up Study, when BMI was defined using a single baseline measurement, a significant inverse association between overweight and mortality was observed [39]. However, this paradoxical association was reversed in analyses using instead the maximum BMI over 16 years of weight history. Having a history of being overweight or obese was linked to an increase in all-cause mortality risk. Thus, this study implies that maximum BMI reflects weight history better for mortality prediction and its use may reduce reverse causation bias associated with a single BMI assessment.
Limitations of BMI as an obesity index
Although BMI is a simple, convenient, and noninvasive surrogate measure of body fat, it is a measure of excess weight per height rather than a direct measure of fat mass. In addition, age, sex, ethnicity, and muscle mass can affect the relationship between BMI and body fat. To our knowledge, there is no demonstration of an “obesity paradox” based on a direct measurement of body fat. Until such demonstration is made, whether the obesity paradox equals the BMI paradox or the adiposity paradox will remain unknown.
Body composition/muscle mass/muscle strength
BMI fails to distinguish between fat and muscle mass, so that very muscular persons may have a high BMI and be misclassified as overweight or obese. Because low muscle mass has been independently associated with mortality [40], it is possible that higher mortality in normal weight subjects may associated with low muscle mass and not low adiposity [41]. On the other hand, many obese individuals have not only increased fat mass but also increased muscle mass [4243]. Thus, relatively higher muscle mass may contribute to better survival outcomes in persons classified as obese. In addition, recent research has demonstrated a role for muscle function as well by demonstrating that greater muscle strength predicts lower risk of mortality [444546]. Hamasaki et al. [46] reported that greater handgrip strength was significantly associated with lower mortality in Japanese men with type 2 diabetes mellitus.
Body fat distribution
BMI does not capture information on body fat distribution. Previous research suggests that the fat distribution pattern has a greater influence on cardiometabolic risk than BMI [4748]. Whereas visceral adiposity plays an important role in development of obesity-associated metabolic disorders, others have proposed that peripheral fat depots may protect against cardiovascular disease [49]. Visceral fat accumulation is greatest in younger adults, and thus would be expected to increase risk of cardiometabolic conditions for many decades [5051]. Although best assessed using imaging, satisfactory surrogate measures of visceral fat exist such as waist circumference, waist/hip ratio, and waist/height ratio, that are all positively associated with mortality [26]. BMI, however, is not able to capture differences in body fat distribution and therefore may misrepresent some diabetic patients as “normal” when in fact excess visceral adiposity is present. In addition, ectopic fat undetectable by measurement of BMI may occur in multiple other anatomic locations including liver, heart, pancreas, and muscle, and is also linked in these locations to adverse cardiometabolic outcomes [52].
Cardiorespiratory fitness
The Aerobics Center Longitudinal Study showed no significant association between BMI and mortality after adjustment for fitness in males with diabetes, and furthermore observed that fitness predicted mortality independent of BMI [24]. McAuley et al. [53] confirmed these findings in male veterans with type 2 diabetes mellitus. Thus, the level of fitness may affect survival of obese individuals, and potentially may confound research on the association between BMI and mortality in persons with diabetes.
CONCLUSIONS
The obesity paradox in type 2 diabetes mellitus has undergone extensive scrutiny by many investigators of whom many have concluded that high BMI does not cause lower mortality. Some of the theories proposed to explain the obesity paradox as due to bias as opposed to a causal benefit of high BMI on lowering mortality are not universally supported by the data identified in this review. For example, if the obesity paradox is simply the result of bias due to selection (conditioning) of patients with diabetes, why then was it observed in a non-diabetic control population of ever smokers [2936]? Furthermore, why was the obesity paradox not evident in two well conducted studies that selected diabetic participants [2728]? We believe that the obesity paradox most likely represents a non-causal association between higher BMI and mortality in diabetes, but await a comprehensive explanation of the remaining loose ends. We believe that the findings of obesity paradox should not change current clinical advice regarding the importance of weight reduction in patients with type 2 diabetes mellitus who are overweight or obese. We agree with Lajous et al. [54] who conclude that we should not recommend that patients with chronic diseases gain weight. A systematic review of randomized controlled trials of weight loss interventions for adults with obesity concluded that these interventions may reduce premature all-cause mortality in adults with obesity [55]. We believe that the literature also provides good support for recommending weight loss to overweight and obese patients who have type 2 diabetes mellitus. The Look AHEAD Study conducted an intensive lifestyle intervention in 5,145 overweight or obese patients with type 2 diabetes mellitus to assess whether this would reduce cardiovascular morbidity and mortality [56]. The intervention group succeeded in losing 8.6% of body weight by year 1 and 6.0% by the end of the study. Although this randomized controlled trial did not demonstrate a reduction in cardiovascular morbidity or mortality, no increase in either of these outcomes occurred, which might have been expected if excess adiposity conferred a survival benefit consistent with the obesity paradox. This clinical trial therefore has a 2-fold benefit as it argues against the obesity paradox and provides reassurance to clinicians that overweight and obese patients with diabetes may safely attempt to reduce weight.
 XML Download
XML Download