

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Breath tests can measure the levels of hydrogen and methane gases in expired breath.12 This is a simple and noninvasive method of detecting the intestinal fermentation of carbohydrates by the intestinal flora.1 Therefore, it is used widely in clinical practice to evaluate small intestinal bacterial overgrowth (SIBO), carbohydrate intolerance, or alterations in orocecal transit.
The results of the breath tests are associated with the gut microbial environment of the host. Changes in the gut microbial environment are associated with host factors, such as sex, age, BMI, and other clinical conditions, including metabolism disorders, related inflammatory conditions, and autoimmune disorders.3 A recent meta-analysis showed that the predictors of SIBO diagnosed by a jejunal culture or breath tests in irritable bowel syndrome (IBS) patients were female sex, older age, and IBS-diarrhea subtypes.4 In two retrospective cohort studies, positive breath-test results were associated with female sex, lower BMI, steroid use, and comorbid diseases, including gastrointestinal diseases, such as peptic ulcer disease, gastroesophageal reflux disease, and gastroparesis.5 On the other hand, data on the effect of host intrinsic factors, such as sex, aging, and BMI, on the breath-test results are limited and conflicting.678
The initial breath tests were based on the measurements of hydrogen as a reflection of gut fermentation.9 Currently, the technology has evolved to include measurements of carbon dioxide and methane. Methane may be an important confounder because there is an interaction between methane and hydrogen during gut fermentation.10 On the other hand, the relationship between hydrogen and methane production in patients with gastrointestinal symptoms is unclear. This study examined the demographic and clinical factors associated with positive breath-test results as well as the relationship between hydrogen and methane production in patients with suspected IBS.
SUBJECTS AND METHODS
1. Patients
Three hundred and seven consecutive patients with abdominal discomfort, abdominal bloating, gaseousness, and/or changes in bowel habits underwent a lactulose breath test between March 2011 and February 2017 at Chonnam National University Hospital. Of these 307 patients, 14 patients with a history of upper gastrointestinal tract or lower gastrointestinal tract surgery were excluded. Twenty-five patients, who were under 18 years of age or over 80 years. No patients had history of inflammatory bowel diseases. Finally, 268 patients (143 females) were included in this study. The Institutional Review Board of Chonnam National University Hospital approved this study (CNUH-2019-320).
2. Lactulose breath test
All patients were instructed to refrain from antibiotic use for 28 days, to discontinue probiotics for 7–10 days, and not to take any other drug that could influence bowel function. In addition, dietary avoidance of fruits, vegetables, grains, beans and bran cereals for at least 24 hours prior to the procedure was recommended.
The patients were instructed to gargle with 20 mL of 0.05% chlorhexidine. Cigarette smoking and physical exercise were not permitted for 30 minutes before or during the test. First, a baseline breath sample was collected from each patient. In cases of a baseline hydrogen concentration of >10 ppm or a baseline methane concentration of >10 ppm, the patients were asked to gargle one more time, and the baseline breath sample was collected again. The patients then ingested 10 g of lactulose syrup. The concentration (ppm) of hydrogen, methane, and carbon dioxide in the breath test were measured every 15 min for 180 min using a Breath Tracker SC (QuinTron, Milwaukee, WI, USA). Several modified parameters for the lactulose breath-test results were defined based on previous reports.211 First, in terms of the hydrogen breath test, positive results were classified as 1) baseline hydrogen >20 ppm, 2) ≥20 ppm increase in hydrogen within 90 min (early hydrogen increase), and 3) ≥20 ppm increase in hydrogen between 90 min and 180 min (late hydrogen increase). In terms of the methane breath test, the positive results were classified as follows: 1) baseline methane >10 ppm, 2) ≥10 ppm increase in methane within 90 min (early methane increase), and 3) ≥10 ppm increase in methane between 90 min and 180 min (late methane increase).
3. Statistical analysis
The continuous variables are expressed as the median and range, whereas the categorical variables are expressed as the number and percentage. The continuous variables were analyzed using an independent t-test or Mann-Whitney U-test, whereas the categorical variables were analyzed using a chi-square test. Univariate and multivariate logistic regression analyses were performed to examine the association between the demographic factors and each parameter on the lactulose breath test. The correlation between the expiratory hydrogen levels and expiratory methane levels was performed using a non-parametric rank correlation (Spearman's correlation). A p-value of <0.05 was considered significant. All statistical analyses were performed using SPSS version 20.0 for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
Of the 268 subjects included in this study, 143 (53.4%) were women. The median age of the patients was 58.0 years (range, 18.0–80.0 years). Table 1 lists the baseline characteristics and comorbidities of the included patients.
1. Associations between the lactulose breath-test results and demographic factors
Among the 268 patients, 19 (7.1%) patients had ‘baseline hydrogen >20 ppm’. In the hydrogen gas parameter, 54 (21.1%) patients showed an early hydrogen increase, and 141 (52.6%) patients showed a late hydrogen increase. In the methane gas parameter, 28 (10.4%) patients showed an early methane increase and 73 (27.2%) patients showed a late methane increase.
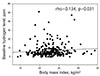
No significant differences in the comorbidities or the presence of abdominal discomfort, abdominal bloating, gaseousness, and/or changes in bowel habits according to the suggested parameters, were observed (Table 1). In addition, there were no significant differences in the suggested parameters on the lactulose breath-test results according to age (Table 2). On the other hand, there was a weak positive correlation between the BMI and baseline hydrogen level (rho=0.134, p=0.031) (Fig. 1). A significant difference in the late hydrogen increase, according to the BMI, was observed (Table 2). Women were significantly more likely to show an early hydrogen increase (Table 1). Similarly, women were significantly more likely to show an ‘early methane increase’ and a ‘late methane increase’ compared to men (Table 2 and Supplementary Table 1).
Logistic regression analysis was performed for the parameters that showed positive results based on sex. After adjusting for age and BMI, women were significantly more likely to show positive results for an early hydrogen increase. Furthermore, a positive early methane increase and late methane increase were observed more frequently in women. The BMI was associated with a late hydrogen increase (Table 2).
2. Associations between hydrogen production and methane production
Significant associations were observed between the hydrogen gas analysis and methane gas analysis results. The baseline hydrogen level was related to the baseline methane level (rho=0.592, p<0.001) (Fig. 2A). A maximal hydrogen level within 90 min was related to the maximal methane level within 90 min (rho=0.721, p<0.001) (Fig. 2B).
Patients with a baseline hydrogen level (>20 ppm) (10/19, 52.6%) were more likely to show a positive baseline methane level (>10 ppm) than patients without a baseline hydrogen level (>20 ppm) (20/249, 8.0%, p<0.001). Patients with early hydrogen increase (28/64, 43.8%) had more positive results for an early methane increase compared to patients without an early hydrogen increase (0/204, 0%, p<0.001). Patients with a delayed hydrogen increase (72/141, 51.1%) were more likely to show a positive delayed methane increase compared to patients without a delayed hydrogen increase (1/127, 0.8%, p<0.001).
DISCUSSION
This study showed the following results. More women showed positive results for an early hydrogen increase, early methane increase, and late methane increase. In addition, in patients with IBS, the baseline hydrogen levels were related to the baseline methane levels, and the maximal hydrogen level within 90 min was related to the maximal methane level within 90 min. Patients with an early hydrogen increase were more likely to show a positive early methane increase than patients without an early hydrogen increase.
The fermentation of carbohydrates by the gut microbiota produces hydrogen gas and methane gas. Many studies have reported conflicting results for the intestinal bacterial composition, which might be explained by the sex ratio, age distribution, and grade of obesity in each study group.6121314 Although several studies on the gut microbiota profiles in patients with IBS reported conflicting results, there are several consistent trends, including the increased levels of firmicutes, decreased levels of bacteroidetes, and increased firmicutes/bacteroidetes ratio.12131415 Haro et al.12 reported that the gut microbiota composition differed according to sex in age- and diet-matched subjects. Age-matched study showed different distribution of Bacteriodes genus, Veillonella, Methanobrevibacter genera between men and women.12 Santos-Marcos et al.13 showed Firmicutes/Bacteroidetes ratio, a higher relative abundance of Lachnospira and Roseburia in pre-menopausal women than in men. These influences of gender on gut microbiota may lead to differences of breath test results between men and women.
A lactulose breath test was performed to obtain indirect information on the fermentation of carbohydrates by gut flora in patients with suspected IBS. In this study, there were no significant differences in the hydrogen or methane parameters on the lactulose breath-test results based on age. On the other hand, there was a weak positive correlation between the BMI and baseline hydrogen level. Previous studies showed that the prevalence of SIBO is higher in women than in men.4516 In addition, women were more likely to show a positive early hydrogen increase, early methane increase, and late methane increase compared to men.
In this study, an early hydrogen increase was observed in 23.9% of patients, whereas an early methane increase was found in 10.4% of patients. Furthermore, 43.8% of patients with an early hydrogen increase had an early methane increase. A previous retrospective study reported that 24%, 18%, and 4% of patients had positive results for hydrogen, positive results for methane, and positive results for both hydrogen and methane, respectively.17
Methane is produced from hydrogen and carbon dioxide during methanogenesis.18 The presence of hydrogen in the breath comes from the gut microbiota only, whereas methane gas is produced by methanogenic flora, such as Methanobrevibacter smithii, Methanospaera stadmagnae, and Methannobrevibacter oralis, which can convert four atoms of hydrogen to one molecule of methane.1019 Therefore, the methane gas levels in the breath mirror the hydrogen gas levels. Bjørneklett and Jenssen20 suggested typical patterns of hydrogen and methane production in healthy subjects, showing either high excretion of hydrogen and low excretion of methane or low excretion of hydrogen and high excretion of methane. On the other hand, this may not always be the case in patients with functional gastrointestinal diseases. Although methanogenic flora is associated with delayed colonic transit in patients with chronic constipation,21 a recent study reported that breath methane production was not associated with colonic transit and that the hydrogenogenic and hydrogenotrophic genes in the colonic mucosa and feces were correlated with constipation or colonic transit.22 Therefore, hydrogen or methane gas production by intestinal fermentation might be interrelated and complicated. The present study showed that the baseline hydrogen levels were related to the baseline methane levels, and that the maximal hydrogen level within 90 min was related to the maximal methane level within 90 min in patients with IBS. Patients with an early hydrogen increase tended to show positive results for an early methane increase. In addition, both hydrogen producing microbiota and methanogenic microbiota might have colonized simultaneously, or that more pathogenic microbiota can produce both hydrogen and methane.
This study had some limitations, such as a retrospective study performed in a single center. Nevertheless, the data were acquired consecutively and collected prospectively using the same standard method.
In conclusion, women were associated with high rates of positive lactulose breath-test results. In addition, methane production was correlated with hydrogen production. Future studies will be needed to evaluate the influence of sex on the gut microbiota composition associated with breath-test results and the treatment response according to the pattern of breath-test results.



 XML Download
XML Download