

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Recently, there is an increase in the prevalence of food allergy worldwide. In Japan, the common foods responsible for allergy are egg, milk, and wheat, in that order from high to low. These are followed by fruits, which are the 5th most common food allergens. Even in new-onset food allergies by age, fruit ranks 5th among 0–3-year-olds, 1st among 4–6-year-olds, and 2nd among 7–19-year-olds, showing that it is an important cause of food allergies particularly from childhood onward [1].
In the recent 10 years, sensitization through eczema has been established in the onset of childhood food allergies. “Cutaneous sensitization” is considered an important route to confirm the onset of allergy following food ingestion [2]. Meanwhile, in the onset of fruit allergies, there is a reaction toward the fruit or vegetable containing the common antigen after pollen allergy occurs, which is followed by a cross-reaction where allergy is induced. This is the commonly known route. In the food allergy guidelines of Japan [3], this is commonly known as pollen-food allergy syndrome (PFAS). The most important common antigen is pathogenesis-related protein-10 (PR-10), and sensitization to Bet v1, which is present in pollen of birch, induces allergic symptoms from rose family fruits such as peach and apple. The next important antigen is profilin and is present in all eukaryotes; therefore, it is difficult to identify the source of sensitization. It induces allergy in various fruits and vegetables. These more rarely exhibit anaphylaxis compared to the immediate type, and heat-induced hypoallergenization is likely to be observed.
There is limited data on the prevalence of PFAS among children with fruit and vegetable allergy in Japan. On the other hand, the prevalence of pollen allergy other than that due to Japanese cedar has been reported as 0.6%, 8.3%, and 20% in children aged 0–4 years, 5–9 years, and 10–19 years, respectively, suggesting a low prevalence for children aged less than 10 years and an increasing prevalence with increasing age [4]. Therefore, it is possible that the proportion of young children with fruit and vegetable allergies who do not have PFAS is high. In the United Kingdom, the proportion of children with pollen allergy who were diagnosed with PFAS was reported as 17%, 50%, and 78% for those aged 0–5 years, 6–10 years, and 11–15 years, respectively [5].
This study aimed to examine the allergens in fruit and vegetable allergies in pediatric patients and the extent of sensitization to PR-10 and profilin.
MATERIALS AND METHODS
Study design and participants
This was a multicenter cross-sectional case series study that was conducted in a total of 6 institutions in a 1-year period from August 2016 to July 2017 with the Pediatric Department of Kindai University Hospital as the representative study site and the Pediatric Departments of 5 other institutions (Osaka Habikino Medical Center, Sumitomo Hospital, Osaka General Medical Center, Yao Municipal Hospital, and Higashiosaka City Medical Center) in Osaka Prefecture as cooperating study sites. The participants were patients aged 0–15 years who visited any of these institutions due to symptoms or chief complaints of itchiness in the mouth; strange feeling in the throat; skin, respiratory tract, or digestive tract allergies; and neurological symptoms after eating fruits and/or vegetables. The patients were recruited into this study if they met the inclusion criterion. We did not conduct skin prick tests to diagnose allergies in this study. Moreover, oral food challenge was not a prerequisite for diagnosis.
The inclusion criterion was the appearance of the final allergic symptom within 1 year. However, patients with the following characteristics were excluded in the study: patients whose specific antibody titer for the antigen did not increase (<0.35 UA/mL) in later blood tests and patients with allergic symptoms for allergens that cannot be measured using the Japanese medical insurance system.
Method
If the patient was 7 years old or older, in addition to the caregiver's informed consent, the patient provided informed assent. After obtaining consent to participate in the study, the test items were in the form of questionnaire administered by the attending physician, and blood tests were performed at the time of examination. The questionnaire consisted of questions on the following: (1) sex, age, medical history, siblings, history of raising a pet, smoking history of the parents, and breastfeeding or feeding the patient with cow's milk formula during patient's infancy; (2) history of allergy (atopic dermatitis, bronchial asthma, allergic rhinitis, and latex allergy) of the patient and history of allergy in the family; and (3) the fruits and vegetables that caused the onset of symptoms (multiple answers allowed), age at first appearance of allergic symptoms, reproducibility of allergic symptoms, types of allergic symptoms that have appeared and their severity, and history of anaphylaxis when eating fruits and vegetables. The blood tests consisted of the measurement of white blood cell count, eosinophil count, total immunoglobulin E (IgE), and specific antibody titer to the fruits and vegetables with the allergic symptoms. Additionally, 3 mL of blood, which was obtained in the representative site, was sent to Siemens Healthcare Diagnostics K. K. (Tokyo, Japan) where specific antibody titers of Dermatophagoides pteronyssinus (mite), Japanese cedar, birch, timothy grass, ragweed, and latex and Bet v1 and Bet v2, which are components of birch, were measured using the IMMULITE 2000 3gAllergy (Siemens Healthcare Diagnostics, Tokyo, Japan).
Outcomes
The primary outcome was the allergen of the participants. The secondary outcomes were the age distribution of each group, number of participants per allergen in each group, and association between Bet v1 and Bet v2 and various allergen-specific IgE antibodies.
Participants with a Bet v1 antibody titer ≥0.35 IUA/mL were diagnosed with PR-10 sensitization and were assigned into the “PR-10 group”; similarly, participants with a Bet v2 antibody titer ≥0.35 IUA/mL were assigned into the “profilin group,” and participants who were positive for both PR-10 and profilin were assigned into the “double positive group.” All the participants who belonged to any of these groups were diagnosed with PFAS. On the contrary, the group where neither PR-10 nor profilin was sensitized was assigned into the “double negative group.”
Statistical analysis
For the statistical analysis, we used GraphPad Prism ver. 7 (GraphPad Software Inc., La Jolla, CA, USA) and compared age by allergen using the Mann-Whitney U-test.
The protocol of this study was established based on the Declaration of Helsinki, and this study was approved by the Ethics Committee of Kindai University Faculty of Medicine (approval number: 28-051) and was conducted after an ethical review by all the institutions that participated in the study.
RESULTS
Participant characteristics
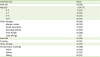
A total of 101 patients were registered from all sites. Three patients with flawed data and 1 patient who had developed allergy not from fruit as there was no increase in the fruit-specific antibody titer that was performed at the site were excluded. Hence, 97 patients were included in the analysis (Fig. 1). None of the participants exhibited allergic symptoms with allergens that could not be measured using the Japanese medical insurance system in top 20 allergens. Participants were predominantly composed of 56 males (58%), and the median age of the overall patients was 9 years. By age, 13 participants (13%) were 0–3 years, 18 (18%) were 4–7 years, 40 (41%) were 8–11 years, and 26 (27%) were 12–15 years. Of all the patients, 89 (92%) had, to some extent, allergic disease, with 68 (70%) having allergic rhinitis, which was the most common allergy (Table 1).

Table 1
Characteristic of the participants
![]()
Allergen of participants and results of the blood tests
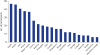
The most common allergen was apple followed by peach, kiwi, cantaloupe, and watermelon, in that order (Fig. 2).
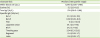
According to the results of the blood tests performed in the participants, the median values (up to 4 decimal places) for leukocytes, eosinophils, and total IgE were 6,540/µL (5,500–7,795/µL), 5.5% (3.0%–8.5%), and 574 IU/mL (218.5–1168 IU/mL), respectively. For the specific antibodies (IUA/mL), the values were 10.3 (0.09–119) for Bet v1 and 0.09 (0.09–8.9) for Bet v2 (Table 2). For antibodies against the pollen, the respective values were 54.1 (2.3–116) for Japanese cedar, 27.2 (1.1–132) for birch, 3.04 (0.3–23.2) for timothy grass, 0.4 (0.09–1.7) for ragweed, and 0.6 (0.09–1.7) for latex (Table 2).
Table 2
Results of the blood test
![]()
Age distribution of each group
The PR-10 group, profilin group, and double positive group consisted of 33 (34%), 12 (12%), and 29 participants (30%), respectively. Of these overall participants, 76% of the participants were diagnosed with PFAS. On the contrary, 23 participants (24%) who had no sensitization to either allergen were assigned into the double negative group. In the 0–3-year-old age group, 11 patients (85%) were assigned into the double negative group. On the contrary, in the 4–7-, 8–11-, and 12–15-year-old age groups, the double negative groups were 33%, 5%, and 15%, respectively. In the 3 groups of PFAS, the number of patients in the PR-10 group who were in the 4–7-, 8–11-, and 12–15-year-old age groups were 6 (33%), 20 (50%), and 7 (27%), respectively, which were the highest among all groups. Even in the double positive group, when combined with the PR-10 group, the number of patients by age group with allergy was 8 (44%), 35 (88%), and 19 (73%) in the 4–7-, 8–11-, and 12–15-year-old age groups, respectively. Compared to the PR-10 group, the profilin group had lower number of patients (2 patients [15%]) in the 0–3-year-old age group. When combined with the double positive group, the number of patients by age group were 6 (33%), 18 (46%), and 15 (58%) in the 4–7-, 8–11-, and 12–15-year-old age groups, respectively, showing a consistent increase with age (Table 3).

Allergen in each group
Regarding the allergen in each group, in the PR-10 group, apple, which was the most common allergen, was the allergen in 24 patients (72.7%), followed by peach in 14 (42.4%) and cherry in 13 patients (39.4%). In the profilin group, watermelon and cantaloupe, which were the most common allergens, were the allergens in 7 patients (58.3%), followed by kiwi and peach in 5 patients (41.7%). In the double negative group, the major allergen was kiwi (12 patients), followed by banana in 9 patients and cantaloupe in 8 patients (34.8%) (Fig. 3).

Association between Bet v1 and Bet v2 and various allergen-specific IgE antibodies
Bet v1 was significantly associated with birch titers (r = 0.99). However, Bet v2 was insignificantly associated with birch antibody titers (r = 0.29). The correlation coefficients of the association between timothy grass and ragweed were 0.4 and 0.57, respectively, which had no significant association. Latex had the strongest association with Bet v2 (r = 0.88) (Fig. 4).

DISCUSSION
In this study, allergens in 97 pediatric patients aged 0–15 years with fruit and vegetable allergies and living in Japan and the percentage accounted for by PFAS were examined. Apple, peach, and kiwi are the common allergens, and PFAS accounts for 76% of the overall cases. In fact, 70% of the participants had allergic rhinitis. Therefore, PFAS needs to be considered when examining Japanese pediatric patients with fruit and vegetable allergies specifically for children greater than 4 years old.
This is the first study in Japan to investigate the association between fruit and vegetable allergy and PFAS in childhood. In a similar case series conducted in Japan where the participants included 100 patients with fruit allergy with a mean age of 31.5 years (range, 3–74 years), the percentage of PFAS due to PR-10 and profilin was reported as 80% (80 patients) [6]. Our study participants were limited to children aged 0–15 years; however, the percentage of PFAS was the same.
Presently in Japan, Bet v1 cannot be measured using the medical insurance system; however, based on the results of this study, the specific antibody titer of birch is significantly associated with PR-10, suggesting that it is useful in the diagnosis of PR-10-related PFAS. Moreover, profilin (Bet v2) is significantly associated with latex-specific antibody titer, demonstrating that in the diagnosis of profilin-related PFAS, latex-specific antibody titer is significantly helpful. However, in this study, latex allergy was found in only 3 patients (3%), and the latex-specific antibody titer of patients with allergies by profilin increased because Hev b8, which is a profilin family and a component of latex, established sensitization as a cross-antigen. Even in the previous reports, a case series conducted in Spain where the participants were children reported that the antibody titer against the crude antigen of latex in children with profilin sensitization increased [7]. Additionally, sensitization toward profilin is established even in younger preschool children, and that percentage increases with increasing age. In older children, allergy induced by profilin is common. In a multicenter cohort study in Italy, it was reported that profilin sensitization begins in childhood and the percentage increases with increasing age, exceeding 20% by the age of 15 years [8]. The results of this study demonstrated that a similar condition is observed in Japan.
In this study, there were several younger patients in the double negative group with allergies to banana and kiwi. Therefore, we assumed that there is a group of fruit allergies unique to childhood. In western countries, lipid transfer protein (LTP) [910] and thaumatin-like protein (TLP) [1112] and, in Japan, gibberellin-regulated protein (GRP) [13] are known allergens of the double negative group fruit allergies and hence are reportedly important. Even in the Japanese case series mentioned previously, of the 20% of the double negative group patients, 65% (13 patients) and 5% (1 patient) had GRP and LTP allergies, respectively [7]. As LTP and GRP were not examined in this study, the incidence rates of patients with LTP and GRP allergies are unknown. Hence, it is important to study the sensitization of these allergens in Japanese pediatric patients with fruit allergies.
Worldwide, there are reports of banana allergy, and latex fruit syndrome has been reported in the past [14]. However, the percentage of patients with latex allergy among these participants was low, which could be a possible reason of the insignificant association between banana allergy and latex allergy. Therefore, the onset was assumed to be due to Mus a4 (TLP) present in the fruit flesh of banana. Interestingly, TLP is also present in kiwi as Act d2. These have been reported to cross-react [15]. This sensitization was likely established by this cross-reaction in patients with allergies to both banana and kiwi in the double negative group. Even among fruit allergies, banana and kiwi are allergens that induce serious allergic reactions in childhood; hence, a more detailed study in Japan is required.
This study has some limitations. First, the participants comprised only patient who wanted to participate in the study, which highly results in a selection bias. However, Bet v1 and Bet v2 could not be measured using the Japanese medical insurance system, hence probably reflecting the actual condition of patients who visited during the study. Second, the sample size was small. Additionally, self-reporting of the patients was the main form of obtaining the complaints of fruit and vegetable allergies; neither an oral food challenge test nor a skin prick test was performed, which likely weakened the precision of the diagnosis. Moreover, the diagnostic accuracy of PFAS may be low since in this study PFAS was diagnosed only by subjective symptoms and sensitization of Bet v1 and Bet v2. To address this problem, it will be necessary to confirm the order of sensitization and onset through longitudinal studies as well as add further immunological tests such as inhibition test. Furthermore, as mentioned previously, the involvement of LTP, TLP, and GRP has not been investigated at all. Hence, one cannot confirm that it is a study that covers all fruit allergies in childhood. In the future, a study that addresses these issues needs to be conducted with the aim of contributing to better treatment of pediatric patients with fruit and vegetable allergies.
In conclusion, the common allergens of Japanese fruit and vegetable were apple, peach, and kiwi. Moreover, when we examine patients with these allergies, we should first consider PFAS even in childhood specifically for children greater than 4 years old.
 XML Download
XML Download