

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Injuries to the posterolateral corner (PLC) of the knee occur in 16% of knee injuries.1) These injuries are commonly associated with motor vehicle trauma, athletic trauma, and falls. And the PLC is frequently injured in tibial plateau fractures. But it is more commonly injured in conjunction with the posterior cruciate ligament or multiple ligamentous injuries. Isolated PLC injuries are very rare, especially in particular in conjunction with Schatzker type 2 tibial plateau fractures. This type of injuries may easily be missed during the initial assessment of a patient. If these injuries were left untreated, it can cause chronic pain, residual instability, and osteoarthritis. We present a case of a Schatzker type 2 tibial plateau fracture with associated isolated PLC injury and literature's review.
Case Report
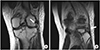
A 28-year-old male who was motor vehicle driver was injured after collision accident. The patient presented to the emergency department and was evaluated by the orthopedic surgery and the general surgery trauma service. He was found to have a fracture of multiple ribs and an injury to left knee. Plain radiographs and computed tomography (CT) scans of the knee showed a lateral split depression type fracture of the tibial plateau (Schatzker type 2), mostly in the anterolateral portion of tibial plateau and a avulsion fragment on a fibular tip (Fig. 1). A detailed ligamentous examination in the acute stage was deferred due to the patient's pain and discomfort. Magnetic resonance imaging (MRI) conformed no injury to the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), or meniscal injury. We performed operation open reduction and internal fixation for the fracture (Fig. 2). Postoperatively, splint immobilization was applied for 2 weeks and constant active quadriceps strengthening exercise was performed. After then, cast immobilization was done for 6 weeks. And then, patient applied MCL brace and started passive range of motion (ROM) exercise. At 3 months later after surgery, patient had full range of motion and walked well without pain or instability. But, at 6 months later, he complained of knee instability especially downing the stairs without minor trauma or accident. On physical examination, patient was shown positive findings on the dial test and the posterolateral rotatory stress test. And the results of the initial MRI were reviewed, we missed a concomitant injury to the structure of the PLC. Injured structures were included biceps femoris and popliteus tendon (Fig. 3). At 11 months later after initial operation, we planned the second operation for stabilizing the PLC and removing plate and screws. We reconstructed the PLC using fibular sling technique (Fig. 4).2) After surgery, splint immobilization was applied for 2 weeks. After then, bracing was performed for 6 weeks, and passive ROM exercise with a continuous passive machine was started. And full weightbearing was allowed 8 weeks later after surgery. At 6 months later after second operation, patient had normal range of motion and no instability and discomfort during walking or stepping (Fig. 5).
Discussion
The PLC of the knee consists of several static and dynamic restraints. Static restraints include the lateral collateral ligament, arcuate ligament, fabellofibular ligament, popliteofibular ligament, joint capsule, and coronary ligaments. Dynamic restraints include the biceps femoris and popliteus muscle tendon units.34) Although the importance of preliminary assessment of these structures is known, they till under-reported and reported 5% to 9% of total knee injuries.5)
The reason for this is that highly specific physical examination and definite evaluation tools for the PLC injury are not accurate. But MRI has proven to be a useful tool in recognition of these soft tissue injuries.6) Especially, in case of injury with intra-articular fracture, combined soft tissue injury was very common. Therefore, MRI examination may be prerequisite for evaluation of this type injuries.
In addition, the PLC injury associated with the proximal tibia fracture is common, but is more commonly associated with posterior cruciate ligament or multiple ligament injuries. It is rare to cause injury to only the posterolateral structures with proximal tibia fracture, especially with Schatzker type 2 fractures. It is uncommon injury to have severe damage to the ipsilateral soft tissue in the presence of damage to the bony structure. Thus, these impairments are often missed and lead to posterolateral instability, chronic pain, and post-traumatic arthritis. Therefore, early recognition and repair should be performed to obtain better clinical results.
In this case, Schatzker type 2 injury was confirmed initially. And whether there was any involvement of the medial soft tissue complex, anterior cruciate ligament, and posterior cruciate ligament or not. Treatment plan was made to focus on restoration of the bony structure and range of motion respectively. During the follow-up, the patient complained of instability, and careful physical examination and MRI revealed that the posterolateral structures were injured.
Zelle et al.7) reported the similar case with the fracture of anterolateral portion of tibia and PLC injury. They treated bony structure and posterolateral structure simultaneously. Maheshwari et al.8) reported that anterior tibial plateau fracture was easily missed fracture type. All three reports including the present report showed that main injured bony structures were anterior tibial plateau.
This trend showed posterior soft tissue lesion was usually concomitant to tibia plateau fracture involving mainly anterior portion.
Classically, we thought that there are two-dimensional mechanisms of injury to tibial plateau. First, there was varus force of the knee. In case of varus force of knee, a compressive lesion was present in the medial compartment and avulsive lesions were present in the lateral compartment.9) Second, there was valgus force of the knee. In contrast, in case of valgus force of knee, a compressive lesion was present in the lateral compartment and avulsive lesions were present in the medial compartment.
In the described case, initially we thought that mechanism of injury was valgus force. Because it had lateral plateau bony fracture, medial soft tissue injury was important for this type injury. We carelessly evaluated posterior and posterolateral soft tissue structures. Therefore, it is necessary to consider that the damage can be varied through three-dimensional analysis according to the position of the knee at the time of injury and the direction of injured force.
As mentioned above, in case of tibia plateau fracture involving the anterior portion, an assessment of soft tissue injury to the posterior portion is considered necessary. In the described case, anterior portion of lateral tibia plateau fracture can be led to posterolateral soft tissue injury. Therefore, we had to check the injury on posterolateral soft tissue structure. More cases can be defined this tendency.
In case of tibia plateau fracture, the most important thing to build the treatment plan was to identify bony fracture type including soft tissue injury through the third dimension.




 XML Download
XML Download