

 PDF
PDF ePub
ePub Citation
Citation Print
Print



서론
수술 전 액와림프절 전이가 의심되는 경우, 유방암 환자의 예후 예측과 수술 전 신보강화학요법 시행 여부 결정을 위해 미세침흡인세포검사를 시행한다. 그러나 초음파 유도 미세침흡인세포검사의 민감도 범위(21~86%)와 음성예측도 범위(60~90%)가 보고에 따라 다양하다(1234567). 이전부터 초음파 유도 미세침흡인세포검사를 이용한 진단을 보완하고자 미세침흡인액으로부터 암배아항원(carcinoembryonic antigen), 암항원(cancer antigen), cytokeratin fragment 21-1 (이하 CYFRA 21-1)과 같은 종양표지자를 측정하는 방법들을 연구해왔다(8910). 더불어 최근 연구들에서는 미세침흡인액 CYFRA 21-1이 Cytokeratin 19의 fragment로서 림프절 전이에 우수한 진단능을 가지고 있으며(9), 초음파 유도 미세침흡인세포검사와 비교하였을 때 진단적 정확도가 같음을 보여주었다(10). 그러나 수술 후 국소 림프절 재발을 평가하는데 있어서 CYFRA 21-1의 진단적 유용성에 대해서는 연구된 바가 없다. 본 연구는 유방암으로 수술을 받은 환자의 액와부 국소 림프절 재발을 평가하는데 있어 CYFRA 21-1의 적절한 역치값과 진단수행도(diagnostic performance)를 구하는 것을 목표로 한다.
대상과 방법
연구 대상
2009년 1월부터 2014년 1월까지 유방암 수술 후 액와림프절 재발 여부를 평가하기 위해 미세침흡인세포검사 및 CYFRA 21-1 농도를 측정한 88명의 의학적 기록을 후향적으로 검토하였다(Severance Hospital; IRB No. 4-2018-0427). 이 중 이전 유방암 수술 관련 정보가 없던 19명과 충분한 추적검사가 시행되지 않았던 5명을 제외하였으며, 최종적으로 64명의 환자를 대상으로 연구를 진행하였다. 초음파 검사상에서 액와림프절 전이가 의심된 64개의 림프절에서 초음파 유도 미세침흡인세포검사와 함께 동시에 미세침세척액 CYFRA 21-1 검사를 시행하였다. 초음파 유도 미세침흡인세포검사를 시행하기 전에 액와 전체에 대한 초음파 검사를 시행하였고, 재발이 의심되는 액와림프절의 크기를 측정하였다. 초음파 및 초음파 유도 미세침흡인세포검사는 경험이 많은 유방영상전문의 4명 중 1명에 의해 시행되었으며(E.K.K, M.J.K, H.J.M, J.H.Y; 3~17년), 5~12 MHz(HDI 500; Philips-ATL, Bothell, WA, USA) 또는 5~12 MHz (iU22; Philips Medical System, Bothell, WA, USA) 선형 탐촉자(linear array transducer)를 이용하여 시행하였다. 의심스러운 초음파 소견으로는 림프절문이 소실되거나 림프절이 둥근 모양 또는 불규칙한 모양을 보이는 경우, 치우친 피질 비후소견(eccentric cortical thickening, > 3 mm), 피질이 지나치게 저에코를 보이는 경우, 도플러 검사상에서 현저한 주변부의 혈류 증가 소견들이 있다. 이중 한 가지 이상의 소견을 보일 경우 재발이 의심되는 림프절로 간주하였으며 미세침흡인세포검사가 진행되었다. 크기는 종단 또는 횡단 스캔에서의 최대 직경으로 측정하였다. 초음파 유도 미세침흡인세포검사는 초음파 유도하에 23 게이지 바늘과 연결된 2 cc 주사기를 이용하여 프리 핸드 기법으로 시행하였다. 각 림프절은 두 차례 흡인되었다. 채취한 흡인액을 슬라이드에 뿌리고 도말하여 세포검사를 위한 검체를 얻었다. 모든 도말한 검체들은 바로 papanicolaou 염색을 위해 95% 알코올에 넣었다. 그리고 바늘과 주사기에 남은 흡인액은 1 cc 식염수로 세척하였다. 이 세척액으로부터 CYFRA 21-1의 농도를 측정하였다.
CYFRA 21-1 분석
미세침세척액의 CYFRA 21-1 농도는 자동화된 화학발광 면역 분석법과 함께 하는 면역분석시스템(E411; Roche Diagnostics, Mannheim, Germany)으로 측정되었다. CYFRA 21-1에 대한 단클론항체를 포함하는 비경쟁적 immunometric assay (sandwich format)가 면역분석 시약과 함께 이용되었다.
병리 분석
5명의 병리학 전문의들이 액와림프절에 대해 시행한 미세침흡인세포검사의 병리 결과를 해석하였다. 세포검사 결과는 유방암으로부터의 전이성 림프절(metastasis from breast cancer) 또는 비정형 세포(atypical cell)인 경우에는 재발 림프절로 분류하였으며 반응성 과형성(reactive hyperplasia) 또는 전이에 대한 음성(negative for malignancy)인 경우에는 양성 림프절로 분류하였다. 그 외에 불충분세포(paucecellular)로 인해 비진단적인 경우는 12예가 있었으며 이 경우는 제외하거나 양성 림프절로 간주하였다. 최종 진단은 수술 및 조직학적 진단, 그리고 적어도 2년 이상의 추적검사를 기준으로 했다.
통계 분석
임상병리적 정보는 의무기록을 조사하여 얻었다. 임상병리적 정보에는 미세침흡인세포검사 당시 림프절의 크기, 원발성 유방암의 병리학 타입(pathologic type), 수술 종류, 수술 날짜, 미세침흡인세포검사 날짜와 CYFRA 21-1 농도를 포함하였다. 총 64명의 환자에서 미세침흡인세포검사 당시 흡인액으로부터 CYFRA 21-1 농도 결과를 얻었다. 림프절의 크기는 종단 또는 횡단 스캔상에서 최장 직경으로 측정하였다. 세포검사상에서 판단된 양성 림프절과 재발 림프절 군 간에 림프절 크기를 비교하기 위해서 Student's t-test를 시행하였다. 두 그룹 간에 병리학 타입, 수술 종류 비교를 위해서 카이제곱검정 또는 Fisher 정확 검정을 시행하였다. 양성 림프절과 재발 림프절 그룹 간의 CYFRA 21-1 농도를 비교하기 위해서 Mann-Whitney U test를 시행하였다. 최종 진단에 대한 CYFRA 21-1 농도의 수신기작동특성곡선(receiver operating characteristics curve; 이하 ROC 곡선)을 확인하였다. 면적하곡선(area under the curve; 이하 AUC)을 확인하였으며, 민감도와 특이도가 최대인 좌상단으로 역치값을 결정하였다. 또한 위양성(positive predictive value), 위음성(negative predictive value) 및 정확도(accuracy)를 구하였다. 세포검사의 불충분세포를 양성으로 간주하여 혹은 제외하여 각각 분석하였다.
결과
총 64명 환자의 원발성 유방암 병리학 타입은 침윤성 유관암(invasive ductal carcinoma, n = 54), 유관상피내암(ductal carcinoma in situ, n = 2), 유두암종(papillary carcinoma, n = 3), 점액암종(mucinous carcinoma, n = 2), 관암종(tubular carcinoma, n = 1), mixed ductal and lobular carcinoma (n = 1)이었다(Table 1). 액와림프절에 대한 미세침흡인세포검사를 통해 총 64명의 환자 중 11명이 재발 림프절, 41명에서 양성 림프절로 진단되었으며 12명은 불충분세포로 세포검사에서 비진단적 결과가 나왔다. 이 중 2명은 다시 시행한 미세침흡인생검, 1명은 절제 생검에서 양성 림프절임이 판단되었으며 나머지 9명은 추적검사(4~8년)에서 변화 없이 관찰되어 임상적으로 양성 림프절로 판단하였다.
불충분세포검사 결과를 비전이로 간주한 분석
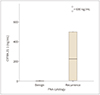
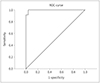
재발 액와림프절(19.8 ± 7.9)의 크기는 통계적으로 유의미하게 양성 액와림프절(9.8 ± 5.3) 보다 크게 나타났다(p < 0.001) (Table 1). 그러나 액와림프절 그룹에 따른 원발 유방암의 병리적 타입 및 수술 종류는 통계적으로 유의미한 차이가 없었다(p = 1.000, p = 0.159). CYFRA 21-1의 중간값은 재발 액와림프절 그룹(225.8 ng/mL, 사분위수 3.5~501.0 ng/mL)이 양성 액와림프절 그룹(0.6 ng/mL, 사분위수 0.5~0.8 ng/mL)에 비해 통계적으로 유의미하게 높았다(p < 0.001) (Fig. 1). 11개의 재발된 림프절에서 얻은 미세침세척액 CYFRA 21-1의 범위는 1.1~4923.0 ng/mL이었으며, 중간값은 225.8 ng/mL였다. 세포검사에서 양성으로 판정된 53개의 림프절에서 얻은 미세침세척액 CYFRA 21-1의 범위는 0.2~1.5 ng/mL였으며 중간값은 0.6 ng/mL였다. 최종 진단에 대한 CYFRA 21-1의 농도에 대한 ROC 곡선을 이용하여 분석한 결과 적절한 진단 기준은 1.6 ng/mL였다(Fig. 2). 이 기준을 적용하였을 때 미세침흡인세포검사에서 재발 림프절로 진단된 11개의 재발 림프절 중 10개에서 CYFRA 21-1 검사에서 양성(positive) 소견을 보였으며 단 1개에서만 음성(negative) 소견이 나왔다(Table 2). 세포검사에서 양성 림프절로 진단된 53개의 림프절 중 53개에서 모두 CYFRA 21-1 검사에서 음성(negative) 소견을 보였다. AUC는 0.997이었다. 민감도는 90.9%, 특이도는 100.0%, 양성예측도는 100.0%, 음성예측도는 98.1%, 정확도는 98.4%였다. 위양성은 0.0%이고 위음성은 1.9%였다(Table 3). 액와림프절 재발이 의심되어 시행한 미세침흡인세포검사에서 불충분세포로 나와 비진단적이었던 12 케이스의 CYFRA 21-1의 농도 범위는 0.4~0.9 ng/mL였다.
불충분세포검사 결과를 제외한 분석
재발 액와림프절(19.8 ± 7.9)의 크기는 통계적으로 유의미하게 양성 액와림프절(10.5 ± 5.6) 보다 크게 나타났다(p < 0.001) (Table 1). CYFRA 21-1의 중간값은 재발 액와림프절 그룹(225.8 ng/mL, 사분위수 3.5~501.0 ng/mL)이 양성 액와림프절 그룹(0.6 ng/mL, 사분위수 0.5~0.8 ng/mL)에 비해 통계적으로 유의미하게 높았다(p < 0.001). 11개의 재발된 림프절에서 얻은 미세침세척액 CYFRA 21-1의 범위는 1.1~4923.0 ng/mL이었으며, 중간값은 225.8 ng/mL였다. 세포검사에서 양성으로 판정된 41개의 림프절에서 얻은 미세침세척액으로 CYFRA 21-1의 범위는 0.2~1.5 ng/mL였으며 중간값은 0.6 ng/mL였다. 최종 진단에 대한 CYFRA 21-1의 농도에 대한 ROC 곡선을 이용하여 분석한 결과 적절한 진단 기준은 마찬가지로 1.6 ng/mL였다(Fig. 2). AUC는 0.996이었다. 민감도는 90.9%, 특이도는 100.0%, 양성예측도는 100.0%, 음성예측도는 97.6%, 정확도는 98.1%였다. 위양성은 0.0%이고 위음성은 2.4%였다(Table 3).
고찰
CYFRA 21-1은 CK19의 녹는 절편이고, 상피세포의 안정성에 기여하는 단백질로서 폐암 및 유방암 환자에서 높은 발현을 보이기 때문에 유용한 종양표지자 중 하나이다(111213.)
최근 유방암의 국소적 재발의 조기 발견은 환자의 생존율을 향상시켰다(14). 국소적 림프절 전이가 흔하지는 않으나 초기 stage의 유방암에서는 1~3%(1516171819), stage에 관계없이는 1.7~15.9%로 보고되었다(2021). 유방암 수술 후 추적관찰 하는 환자에서 이러한 국소적 림프절 전이를 조기에 발견하여 적절한 치료 계획을 세우는 것이 필요하다. 이전 연구에서는 유방암 환자에서 추적관찰 시, 재발이 의심되는 림프절에 대한 평가를 위한 미세침흡인세포검사가 수술 전 액와림프절 평가와 마찬가지로 우수한 진단수행도를 보였으며 신뢰할 만한 평가방법임을 보여주었다(22). 본 연구에서는 수술 후 추적검사에서 재발이 의심스러운 액와림프절에 대한 미세침세척액 CYFRA 21-1 검사가 1.6 ng/mL를 진단 기준으로 하였을 때 우수한 진단수행도를 보였다. 이는 불충분세포로 미세침흡인세포검사에서 비진단적으로 나왔던 환자를 포함하는 여부에 관계없이 같은 값으로 나왔다. 1.6 ng/mL를 진단 기준으로 하였을 때, 실제로 재발 림프절이 아닌데 CYFRA 21-1이 증가하여 재발 림프절로 평가되는 경우인 위양성과 실제로 재발 림프절인데 CYFRA 21-1이 올라가지 않아 양성 림프절로 평가되는 위음성도 매우 낮은 결과를 보였다. 유방암 중 유두암종과 후형질 아형유방암은 CK19 양성률이 낮은 것으로 보고되고 있어 이들에 대한 전이림프절의 진단에선 CYFRA 21-1 값이 높지 않을 가능성 있으나(23) 일반적으로 림프절 전이를 평가함에 있어 같은 CK19를 이용한 one-step nucleic acid amplification (OSNA)에서 위음성이 매우 낮았으며, 유방암의 조직학적 유형에 관계없이 미세전이를 발견함에 있어 낮은 위음성, 위양성률을 보였다(1123). CYFRA 21-1은 종양표지자로 비세포성 폐암을 비롯한 다양한 암 환자의 혈장에서 높은 농도로 측정되어(24) 이전 연구에서 수술 전 환자에서 미세침흡인세포검사의 진단수행도를 개선하는데 도움이 됨을 보였으며(9), 본 연구에서도 수술 후 환자에서도 유용할 수 있다는 결과를 보였다고 할 수 있다. 미세침흡인세포검사와 비교 했을 때 여러 가지 장점이 있다. 첫 번째로 세포검사의 결과는 병리 의사에 의해 판단되는 것이기 때문에 다소 주관적일 수 있으며, 병리 의사들 간에도 의견의 차이가 있을 수 있다. 반면에 미세침세척액 CYFRA 21-1 농도 측정은 객관적인 기준으로 결과가 결정된다는 점에서 장점이 있다. 두 번째로 미세침흡인세포검사의 경우는 종종 불충분세포 등의 이유로 비진단적인 결과가 나오는 경우가 있어서 미세침세포검사를 다시 시행하거나 수술적인 생검 등을 다시 검사를 해야 하는 경우가 있다. 이러한 경우 비용과 시간이 소요될 뿐만 아니라 환자에게도 불편함을 줄 수 있다. 그러나 CYFRA 21-1 농도 측정은 세포불충분으로 결과를 얻지 못할 가능성이 없으며 소량의 흡인액으로도 측정이 가능하기 때문에 비진단적인 결과가 나올 가능성이 적다는 점에서 장점이 될 수 있다. 실제로 우리 연구에서는 64명의 환자 중 12명의 환자가 첫 번째 미세침흡인세포검사에서 불충분세포로 인하여 비진단적인 결과를 얻었었다. 이 12명의 환자들에서 CYFRA 21-1의 농도는 0.4~0.9 ng/mL의 범위에 포함되어 있었으며 모두 진단 기준 1.6 ng/mL보다 낮은 농도로 음성 결과에 해당하였으며, 이 환자들은 재검사 또는 추적관찰 하였을 때, 최종적으로 양성 림프절로 판정되었다. 세 번째로 세포검사의 경우는 병리 의사에 의해 해석이 되어야 하기 때문에 결과를 얻기까지 필요한 시간이 CYFRA 21-1 농도 측정에 비해 길다.
우리 연구의 한계로는 첫 번째로, 액와림프절에 대한 최종 진단이 수술을 통한 병리적 확진 결과가 아니라는 점이다. 수술 전 병기 결정을 위한 액와림프절 평가의 경우는 수술 시 감시림프절생검 또는 액와림프절 절제술을 통해 병리적 확진이 이루어지지만 수술 후 추적관찰에서 액와림프절의 재발이 의심되는 경우에는 수술적 치료 외에 항암 치료를 하는 경우가 많기 때문이기도 하다. 본 연구에서도 전이성 림프절을 진단받은 11명의 환자 중 5명은 원거리 전이가 있어 항암치료를 진행하였으며, 5명은 림프절 전이 또는 림프절 전이 및 흉벽 재발이 있는 환자였으며 항암치료를 진행하였다. 그 외 한 명은 진단 후 추적관찰이 이루어지지 않았다. 두 번째로는 추적관찰 시에 재발 림프절을 평가함에 있어서는 미세침세척액 CYFRA21-1이 도움을 줄 수 있으나 재발이 확진된 이후 치료법을 결정하기 위해서 추가적으로 필요할 수 있는 핵생검술 또는 절제 생검을 궁극적으로 대체할 수는 없다는 한계점이 있다. 그러나 핵생검술 혹은 절제 생검 등의 적극적인 확인이 필요할지 여부를 가늠하는데는 도움이 되겠다. 세 번째로는 비교적 적은 수의 액와림프절로 연구가 이루어졌다는 점이다. 추후 좀 더 많은 수의 림프절을 대상으로 연구가 필요할 것으로 생각된다. 네 번째로는 본 연구는 유방암이 진단된 환자들만을 대상으로 연구가 이루어졌으며 대조군에 대한 연구는 이루어지지 않았다. 그러나 최근 연구에서 양성 림프절로 확진된 림프절에서 시행한 미세침세척액으로부터 CYFRA 21-1 농도를 측정하였을 때 0.02~1.9 ng/mL 임을 보여주었으며 이 결과를 우리 연구의 대조군으로 참조할 수 있을 것으로 생각된다(25).
결론적으로, 유방암 수술 후 액와림프절 재발이 의심되는 환자에서, 미세침세척액 CYFRA 21-1 농도 측정은 역치값을 1.6으로 하였을 때 우수한 진단수행도를 보여준다. 이 결과는 미세침세척액 CYFRA 21-1 농도 측정이 유방암 수술 환자에서 액와림프절 재발을 진단하는데 있어 유용함을 보여준다.



 XML Download
XML Download