

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Antiphospholipid syndrome (APS) is a systemic autoimmune disorder characterized by arterial and venous thrombosis or pregnancy morbidity in patients with persistent antiphospholipid antibodies, such as anticardiolipin antibodies, lupus anticoagulant, and/or anti-ß2 glycoprotein-I antibodies.1 APS can be suspected if any of the following occurs: fetal death at > 10 weeks, frequent miscarriages, severe preeclampsia, or a disease caused by an unknown origin of thrombus.2 Nonthrombotic manifestations include thrombocytopenia, hemolytic anemia, cardiac valvular disease, livedo reticularis, and cognitive dysfunction.3 The association of autoimmune disease with APS is well known, with systemic lupus erythematosus (SLE) being the most frequent disease associated with APS.4
Meaningful results regarding the pathogenesis, clinical manifestations, treatment, and prevention of APS have been reported.356 In 1990, the incidence and prevalence of APS were estimated approximately five new cases per 105 persons-years and 40–50 cases per 105 people, respectively.7 Antiphospholipid antibodies have been also widely studied. Approximately 5% of the general population is expected to be positive for antiphospholipid antibodies; among healthy blood donors, 10% are positive for anticardiolipin antibody and 1% are positive for lupus anticoagulant.89 Recently, a population-based research of 144,248 participants showed that during a 16-year study period, 33 incident cases were recorded and the annual incidence and estimated prevalence of APS were approximately two persons per 105 person-years and 50 per 105 people, respectively.10 However, APS is a rare disease and needs to be studied in a large population. Till date, nationwide population-based epidemiology studies regarding APS are unavailable.
This research aims to conduct the first nationwide population-based study of prevalence, incidence, and related complications of APS based on the database of the National Health Insurance (NHI), which is a nationwide mandatory insurance scheme provided by the Korean government and covering more than 52 million Koreans.
METHODS
Data source
Claims data extracted from the Health Insurance and Review Agency (HIRA) between January 1, 2008, and December 31, 2017, were analyzed. The NHI covers 97% of the Korean population, and the remaining 3% are covered by the Medical Assistance Program and the Medical Care for Patriots and Veterans Affair Scheme. HIRA is also a system operated by the Korea government, which stores the information of the three abovementioned insurance schemes electronically. All medical institutions in Korea send a claims database to HIRA, which includes demographics, inpatient and outpatient visits, diagnostic codes, tests and surgical codes, and prescription drug codes. Detailed structures of the HIRA and related research results are described elsewhere.111213 This research conducted an APS epidemiologic study based on the information identified in the HIRA claims database. To identify APS in HIRA system, we used diagnosis codes from the Korean Classification of Disease, 7th edition (KCD-7), which is a modification of the International Classification of Disease, 10th revision (ICD-10), and a rare intractable disease (RID) registration program. Korean government runs a RID program for 167 rare diseases and offers up to 90% copayment reduction for those who can meet the diagnostic criteria with physician certification. Considering this financial support, claims made by unreliable diagnoses can be rejected by the NHI; thus, all medical institutions review the accuracy of the diagnosis before submitting to the NHI.
Diagnosis of APS
The diagnostic code of APS was confirmed using V253 (APS) of RID and D68.6 (other thrombophilia) of KCD-7, which corresponds to D68.6 (other thrombophilia) of ICD-10 (Supplementary Table 1). The V253 can be used as a single disease code for APS. However, the D68.6 has three sub-diagnostic diseases, namely, anticardiolipin syndrome, APS, and presence of the lupus anticoagulant, which cannot be used alone for APS diagnosis. Hence, additional operational definitions were made. According to the revised Sapporo criteria, patients with APS should undergo an antiphospholipid antibody test at least 12 weeks apart, and only if the same antigenicity is verified twice, the persistence of antiphospholipid antibodies can be confirmed.1 Required minimum laboratory test was based on the case wherein the same antibody test code was identified at least twice (Supplementary Table 1). However, considering that the test results are unknown, and the anticoagulant is not prescribed for a long time with the diagnosis of the anticardiolipin syndrome or the presence of the lupus anticoagulant, only those who prescribed anticoagulants (warfarin, enoxaparin, heparin, antiplatelet, rivaroxaban, apixaban, dabigatran, and edoxaban) more than 180 days and satisfied the laboratory test conditions were defined as APS.
Primary and secondary APS
The APS is classified as primary APS in the absence of systemic autoimmune disease and secondary APS in the presence of SLE or other systemic autoimmune disease. To investigate the association of APS to a systemic autoimmune disease, we identified six disease codes (SLE, rheumatoid arthritis [RA], Sjogren syndrome, vasculitis, dermatomyositis, systemic sclerosis) for 1 year before and after the new diagnosis of APS.
Obstetrical APS
The association between APS and obstetrical disorder was investigated. When APS was newly diagnosed among women up to 49 years old, codes for abortion, stillbirth, eclampsia, and preeclampsia were identified.
Catastrophic APS (CAPS) and major clinical manifestation of APS
Patients with APS that presented life-threatening thrombotic events involving multiple organs over a short period are classified as CAPS.141516 Generally, CAPS is treated with a combination of anticoagulants, glucocorticoids, intravenous immune globulin, and plasma exchange. Acute renal failure, adrenal hemorrhage, encephalopathy, respiratory distress syndrome, and diffuse alveolar hemorrhage are common in CAPS.31718 Therefore, CAPS was defined as a case in which at least two codes among the abovementioned treatments were identified in newly diagnosed patients with APS during admission; at the same time, one or more of the five disease codes were confirmed together. The identified major clinical manifestations of APS included codes of pulmonary thromboembolism (PTE), deep vein thrombosis (DVT), cerebral infarction, and transient ischemic attacks in newly diagnosed patients with APS.
Statistical analysis
The entire Korean population (n = 52,272,755) covered by HIRA in 2016 was obtained from the Korean Statistical Information Service (http://kosis.kr). For the incidence estimates, the data of the earliest claim of APS according to our operational definition were defined as the index data, which were also considered as the incident time. On the basis of the incident time, the corresponding patient was defined as the incident case in that year. For the accuracy of the analysis, a clearance period was set by excluding cases identified in the first year (2008) to remove any potential pre-existing cases of APS. In addition, cases confirmed in the last year (2017) were excluded because of insufficient 1-year follow-up data. Newly diagnosed patients with APS from January 1, 2008, to December 31, 2016, were defined as incident cases. Among them, those with claims data generated by visiting the medical institution at least once in 2016 were divided into the total Korean population covered by HIRA in the same year to calculate the 1-year period prevalence. Then, the 95% confidence interval (CI) of the prevalence and incidence rates was estimated by applying Poisson distribution. From 2009 to 2016, the annual incidence rate was calculated as the number of incidence cases in a corresponding year divided by the Korean population covered by HIRA in that year. To compare the annual incidence to reflect the changes in the demographic structure over 8 years, we set the standardized incidence for the Korean population in 2016 as the reference. We evaluated the trends in the incidence of age group by gender. In the incidence cases, the χ2 or Fishers' exact test was used to compare the presence of autoimmune diseases according to gender. All statistical analyses were performed using the SAS Enterprise Guide software version 6.1 (SAS Institute, Inc., Cary, NC, USA).
RESULTS
Incidence
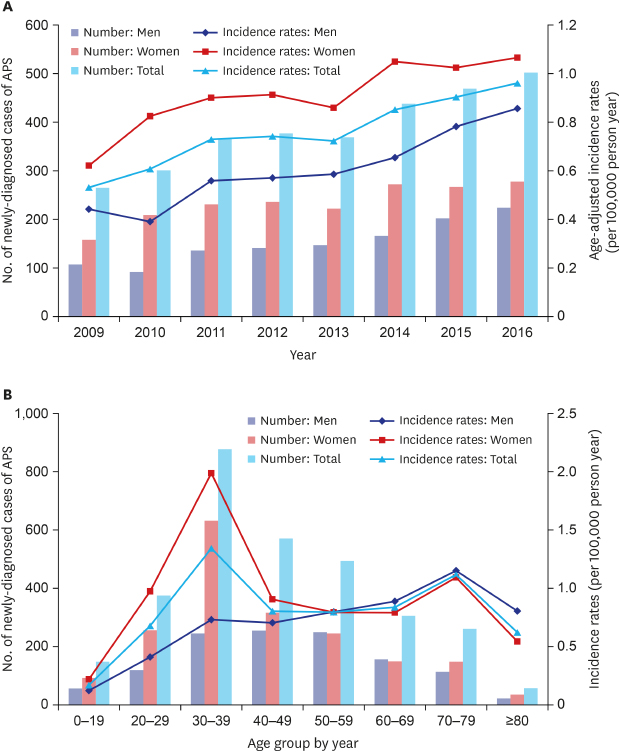
From 2009 to 2016, we identified 3,088 incident cases, comprising 1,215 men and 1,873 women (Fig. 1). The mean age was 44.6 ± 16.6 years, with men at 47.4 ± 16.3 years and women at 42.8 ± 16.6 years (median 42 total years; men, 47 years; women, 39 years). During the study period, the incidence rate was 0.75 per 105 person-year (95% CI, 0.73–0.78), with men and women at 0.59 (95% CI, 0.56–0.62) and 0.91 per 105 person-year (95% CI, 0.87–0.96), respectively. The highest incidence rates were observed at the age range of 30–39 years in the whole population (1.34 per 105 person-year; 95% CI, 1.26–1.43) and women (1.99 per 105 person-year; 95% CI, 1.84–2.15), whereas that in men was at 70–79 years (1.12 per 105 person-year; 95% CI, 0.99–1.26). The annual incidence of age and gender adjustment in the APS had increased by 1.81 times since 2009 (0.53 per 105 person-year; 95% CI, 0.47–0.60) to 2016 (0.96 per 105 person-year; 95% CI, 0.88–1.05) (Supplementary Table 2 and Fig. 2).
Fig. 1
Identification of antiphospholipid syndrome cases in the Health Insurance Review and Assessment Service databases.
APS = antiphospholipid syndrome.

Fig. 2
The incidence of APS. (A) Number of newly diagnosed cases of antiphospholipid syndrome and age-adjusted incidence between 2009 and 2016 (the standardized incidence for the Korean population in 2016 as the reference), (B) and by age groups during the study period. Rates are per 105 person-years.
APS = antiphospholipid syndrome.

Prevalence
Among the patients newly diagnosed with APS during a 9-year (2008–2016) study period, 3,235 had at least one medical checkup in 2016; it included 1,246 men and 1,989 women. The mean age of the prevalent cases was 43.7 ± 16.4 years, with men at 46.5 ± 16.1 years and women at 42.0 ± 16.3 years (median, 41 total years; men, 46 years; women, 38 years). The prevalence during the 1-year period of 2016 was 6.19 per 105 people (95% CI, 5.98–6.41), with men and women at 4.76 (95% CI, 4.50–5.03) and 7.62 per 105 people (95% CI, 7.29–7.96), respectively. The peak prevalence of the total population was at the age range of 30–39 years, with 12.11 per 105 people (95% CI, 11.35–12.91). When stratified by gender, the highest prevalence in men was at the age range of 70–79 years, with 7.44 per 105 people (95% CI, 6.08–9.02), whereas that in women was at the age range of 30–39 years, with 18.05 per 105 people (95% CI, 16.72–19.46) (Supplementary Table 3 and Fig. 3).

Primary and secondary APS
Of the total cases, 1,766 (57%, 810 men and 956 women) were primary APS, 1,322 (43%, 405 men and 917 women) were secondary APS, and 845 (27%, 216 men and 629 women) were associated with SLE. Primary APS in men was twice as high as secondary APS and 1.2 fold in women. The most common autoimmune diseases in secondary APS were SLE (844 cases, 64%) and RA (809 cases, 61%), with the remaining diseases accounted for less than 8%. In addition, patients included in each autoimmune disease were not mutually exclusive. For women, 68% of SLE and 59% of RA were identified, whereas 66% of RA and 53% of SLE for men. The most common autoimmune diseases were different according to gender (Supplementary Fig. 1).
Obstetric APS
For 1 year before and after the new diagnosis of APS, 1,204 women with APS aged between 20 and 49 years. Additionally, abortion and stillbirth codes were identified in 437 (36.30%), and preeclampsia and eclampsia codes were confirmed in 36 (2.99%) patients. The abovementioned codes have not been identified in patients under 19 years old and those at 50 years old or older.
CAPS and major clinical manifestation of APS
During the study, 94 (3.04%) cases of newly diagnosed patients with APS were identified as CAPS at the first diagnosis, with 40 (3.30%) cases for men and 54 (2.88%) cases for women. The DVT code was found in 619 cases (20.0%), the PTE code in 540 cases (17.5%), and the cerebral infarction and transient ischemic attack codes in 862 cases (27.9%). Patients included in each clinical manifestation were not mutually exclusive.
DISCUSSION
This is the first nationwide population-based study of the incidence, prevalence, and related complications of APS based on HIRA data, which is a nationwide mandatory insurance scheme provided by the Korean government. Unlike a previous population-based study, our research showed that the incidence rate of APS differed according to gender and age groups. In secondary APS analysis, SLE was identified as the most relevant autoimmune disease, which was previously identified; however, it was observed that RA was also highly associated with secondary APS, particularly in men patients.
The Euro cohort (Euro-Phospholipid Project) and the Northwest Italian cohort (APS Piedmont Cohort) consisted of 1,000 and 274 diagnosed patients, respectively. They revealed various important clinical information through findings during the observation period along and past medical history. However, the cohort configuration itself had limitations in which selection biases are inevitable. Additionally, the Euro cohort, which is the largest cohort study, had diagnostic criteria as of 1999,19 and 41.9% of patients were lost to follow-up, whereas the Italian cohort with 274 patients has yet to report further findings.42021 These cohorts did not show general epidemiology on prevalence and incidence. Recently, a population-based study (Olmsted County study) of 144,248 participants showed that during the 16-year study period, 33 incident cases were recorded, and the annual incidence of APS was around two persons per 105 person-years, with an estimated prevalence of 50 per 105 people. However, patients with APS diagnoses were only few, and a specific area of the population was insufficient to analyze the overall epidemiology.10 We analyzed the data of 3088 newly diagnosed patients with APS through the HIRA databases, which cover more than 52 million of Korean population, during the 9-year study period and showed the incidence and prevalence rates with other related clinical features (Table 1).
Table 1
General characteristics and clinical manifestations in the Korean HIRA study in comparison with previous research
| Characteristics | Cohort study | Population-based study | |||
|---|---|---|---|---|---|
| Euro-phospholipid project | APS piedmont cohort | Olmsted county study | Korea HIRA study | ||
| No. of patients with APS | 1,000 | 217 | 33 | 3,088 | |
| Study population | - | - | 1.4 × 105 | 522.7 × 105 | |
| Classification criteria | Wilson et al.19 | Miyakis et al.1 | Miyakis et al.1 | Miyakis et al.1 | |
| Study period | 1999–2009 | 2012–present | 2000–2015 | 2008–2017 | |
| Mean age at diagnosis | 34 ± 13a | 43.7 ± 15.3 | 54.2 ± 18.5 | 44.6 ± 16.6 | |
| Women | 820 (82) | 162 (74.7) | 18 (55) | 1,873 (60.7) | |
| Primary APS | 531 (53.1) | 115 (52.9) | - | 1,766 (57) | |
| SLE-related APS | 362 (36.2) | 60 (27.6) | 6 (18) | 845 (27) | |
| Clinical manifestations | |||||
| Fetal lossb | 83 (10.1) | 38 (23.5) | 3 (16.7) | 437 (23.3) | |
| DVT | 317 (31.7) | 81 (31.3) | 14 (42) | 619 (20.0) | |
| PTE | 90 (9.0) | 26 (12.0) | 13 (39) | 540 (17.5) | |
| Stroke | 131 (13.1) | 53 (24.4) | 11 (33) | 862 (27.9) | |
| TIA | 70 (7.0) | - | 4 (12) | ||
| Catastrophic APS | 9 (0.9)c | 3 (1.3) | - | 94 (3.0) | |
Data are presented as mean ± standard deviation or number (%).
In Euro-Phospholipid Project, data were used at the time of the disease onset.
HIRA = Health Insurance and Review Agency, APS = antiphospholipid syndrome, DVT = deep vein thrombosis, PTE = pulmonary thromboembolism, TIA = transient ischemic attack.
aAs there were no studies reporting mean age at diagnosis, age at the onset of symptoms attributable to the disease was used; bFetal loss compared to women population; cIncidence case during the 10-year follow-up.
The mean age at diagnosis was 44.6 ± 16.6 years, with 47.4 years for men and 42.8 years for women. The average age of diagnosis was lower than that in the Olmsted County study (54.2 vs. 44.6, respectively). The ratios of women in the two cohorts, namely, the Euro-Phospholipid Project and the APS Piedmont Cohort, were 82% and 74.7%, respectively. Meanwhile, such ratio in the population-based studies was relatively low in the Korean HIRA study (60.5%) and the Olmsted County study (55%). Therefore, selection biases were in cohort composition and indicated that more attention should be paid in men patients with APS.
In the Olmsted County study, no difference in APS incidence rates by gender and no evidence of a differential age effect in men vs. women were found. However, in the current research, the incidence rates between men and women showed different patterns. Men showed peak incidence rates at 70–79 years old, while women revealed incidence peak at 30–39 years and at 70–79 years old. In men, the primary APS, secondary APS, and SLE-related APS incidence rates all showed a peak at 70–79 years old. In women, the primary APS incidence rate showed peaks at 30–39 years and at 70–79 years old, but both the secondary APS and SLE-related APS incidence rates showed a peak only at 30–39 years old. Unlike women, the incidence rate in men tended to increase with age at overall (P trend < 0.001), primary APS (P trend < 0.001), and secondary APS (P trend < 0.001) (Supplementary Tables 4, 5 and Fig. 4). Considering that SLE was the most frequent autoimmune disease in secondary APS, the age group for both the peak incidences of SLE and secondary APS is the same.22 In the epidemiology study of SLE in Korea, women demonstrated that the peak age of SLE incidence was at 30–39 years of age, which showed the same result in the current study; thus, the increase in SLE may be related to the increase in secondary APS in women.23
Fig. 4
Age- and gender-adjusted incidence rate of primary, secondary, and systemic lupus erythematosus-related APS (per 105 person-year) by age group in Korean population during 2009–2016.
APS = antiphospholipid syndrome.

The incidence by year was 0.53 per 105 person-year in 2009 and increased to 0.97 per 105 person-year in 2016. However, the diagnosis rate increased rather than the number of patients. In 2008, 3,322 antiphospholipid antibody tests were performed, but in 2017, it increased annually to 17,341, which is more than fivefold (Supplementary Fig. 2). Thus, physician's awareness and diagnostic efforts for APS have increased. The incidence rate in previous studies was relatively higher than that in the current study (Olmsted County study, 2 per 105 person-years vs. Korean HIRA study 0.75 per 105 person-year). However, studies investigating the actual incidence and prevalence of large populations, such as our research, are still unavailable. Another large-scale population-based study involving different ethnic group and regions is necessary.
The ratio of primary APS to secondary APS in men was approximately 2:1, but in women, it was 1:1.2; thus, secondary APS in women was higher than in men. In the secondary APS analysis, all autoimmune diseases were not mutually exclusive. SLE was the most common, but RA also showed a higher portion and was more in men than SLE. Other autoimmune diseases, except SLE and RA, were less than 8%. Among the autoimmune diseases, SLE (P < 0.001), RA (P = 0.026), Sjogren syndrome (P = 0.002) and vasculitis (P = 0.006) showed statistically different distribution according to gender. The prevalence of SLE and Sjogren syndrome higher in women, while that of RA and vasculitis was higher in men. DM and systemic sclerosis showed no statistically significant difference between men and women. RA can be overdiagnosed by physicians. In fact, increased cases of DVT and PTE in patients with RA were reported,24 and only few studies regarding the association of RA with APS are available.25 The reported prevalence of antiphospholipid antibodies in RA ranges from 5% to 75%, with a mean value of 28% and a median of 22%.26 Therefore, apart from SLE, RA may be another major disease involved in the occurrence of APS.
For 1 year before and after the new diagnosis of APS, among 1,209 women with APS aged between 20 and 49 years, abortion and stillbirth codes were found in 437, with a fetal mortality rate of 14.2% (437/3088), which was higher than that in the Olmsted County study (9.1%). Fetal mortality relative to childbearing age in the women population was 36.1% (437/1209), but the definite fetal mortality may be higher because not all childbearing women are pregnant. In the Euro-Phospholipid Project, 1,580 cases of pregnancy in a total of 590 women had been recorded from symptoms onset until entry into the enrollment, of which 827 fetal deaths were reported, showing a high fetal mortality rate of 52.3%. In the case of preeclampsia and eclampsia, 82 out of 590 pregnant women were identified in the Euro-Phospholipid Project (8.2%); in the current study, 36 out of 1,209 childbearing-age women were found (1.2%), showing a relatively low rate. However, as with fetal mortality, the high actual incidence is expected. Such cases of high pregnancy morbidity and fetal loss emphasize the importance of early diagnosis and management of APS.
The Euro-Phospholipid Project reported that the incidence of newly identified CAPS during the 10-year observation period was approximately 1%,4 but it was higher in our study (3%). In the Euro-Phospholipid Project, the patients died with CAPS who could not be registered, and 41.9% of the patients were lost to follow-up. Given that patients maintain regular medical follow-ups with preventive anticoagulants (77%) after the diagnosis, the incidence may lower than it actually is. In this study, thrombotic manifestations, namely, DVT and PTE, were 20% and 17.4%, respectively. Furthermore, all three studies have various differences. Stroke and TIA were identified in 28% of patients, and the highest incidence rate was reported in the Olmsted County study with the highest average diagnostic age.
The study has the strength of being the first nationwide population-based study with more than 52 million people, but some limitations were noted. First, the diagnostic codes, which were assigned by the health care providers, might not be entirely accurate. The results of antiphospholipid antibody test, imaging, and clinical manifestations were not available to the researchers. However, we used RID registration program with strict diagnostic conditions, and also attempted to overcome these limitations through the operational definition of at least two identical APS antibody tests and the use of anticoagulants for a long period of time. Second, the incidence of APS can differ according to the incidence of autoimmune diseases by region or ethnic groups. Especially, SLE is common in APS, and it showed various incidence rates across the world (0.3–23.2 per 105 person-years).27 Therefore, the results of this study may not generalize all population groups.
Unlike a previous population-based study, the incidence of APS differed according to age groups and gender. The incidence of primary APS was higher than that of secondary APS in both gender. Furthermore, as already reported, secondary APS is highly associated with SLE; however, we observed that RA is also highly related. The findings of this study may help physicians understand the nature of epidemiology and the burden of APS.
 XML Download
XML Download