

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
A variety of factors can contribute to gastric cancer carcinogenesis. Because Helicobacter pylori was a notable cause of gastric cancer development, it should be eradicated to prevent gastric cancer. However, eradication rate of H. pylori by proton pump inhibitor (PPI)-based standard triple therapy (STT) has been gradually decreasing in Korea.1 The main cause of declining eradication rate over time is increased antibiotic resistance rate and poor compliance. Therefore, alternative regimen was introduced for overcoming this problem. Results using these alternative regimens are being debated. Sequential therapy (ST) for 10 days was superior to 7-day STT in a Korean study.2 ST is superior to 7-day STT but not to STT with prolonged duration in meta-analysis in Korea.3
According to guidelines of the Korean society of gastroenterology, duration of first-line therapy (PPI based STT) and second-line therapy (bismuth-containing quadruple therapy) was 7–14 days.4 Recent studies revealed 14-day STT had significantly higher eradication rate by 5%–9% than 7-day STT.1 Based on the Cochrane database in 2013, increasing duration of STT increases H. pylori eradication rates.5 It is questionable that prolongation of the treatment period would be effective in increasing the eradication rate. As for second-line therapy, eradication rates revealed diverse results based on duration of bismuth-containing quadruple therapy as well. In meta-analysis of Korea, there was no significant difference between 7-day and 14-day PPI + bismuth + metronidazole + tetracycline (PBMT) on H. pylori eradication rate by intention-to-treat (ITT), however, 14-day PBMT increased eradication rates in per-protocol (PP) analysis.3
We compared eradication rates of 7-day STT and 14-day as first-line therapy, prospectively. In addition, eradication rates were compared between 7-day and 14-day bismuth-containing quadruple therapy as second-line therapy for those that failed first-line STT.
METHODS
Patients
This multicenter, randomized, open-label, and prospective study (clinical trial No. NCT02487511) was conducted at four medical centers (Bucheon St. Mary's Hospital, Seoul St. Mary's Hospital, Yeouido St. Mary's Hospital, and St. Paul's Hospital, Catholic Medical Center, Korea) May 2015–January 2017. This study was conducted in accordance with good clinical practice and the Declaration of Helsinki guidelines. Patients were eligible for inclusion if they were age 20–75, had H. pylori infection by endoscopy. H. pylori infection was diagnosed based on histologic evidence by silver staining, or positive rapid urease test. Criteria for exclusion included: previous H. pylori eradication therapy; ingestion of antibiotics or PPI within the prior 4 weeks; patients with previous gastric surgery; co-existence of serious concomitant illness (liver cirrhosis or chronic kidney disease); and pregnant or lactating women.
Intervention
Patients were randomly assigned into two groups based on duration of therapy either 7 days or 14 days in first-line therapy (https://www.random.org/). STT as first-line therapy comprised of standard-dose PPI (lansoprazole 30 mg, pantoprazole 40 mg, or rabeprazole 20 mg) plus amoxicillin (1,000 mg) and clarithromycin (500 mg) twice daily after meal. Patients that failed to first-line therapy were randomly assigned into two groups either 7 days or 14 days as second-line therapy. Bismuth-containing quadruple therapy as second-line therapy included standard-dose twice daily PPI, 120 mg bismuth 4 times a day, 500 mg metronidazole 3 times a day, and 500 mg tetracycline 4 times a day. Compliance was sufficient in case of taking medications over 85% for 7 days and 85% for 14 days. Eradication success was defined as a negative 13C-urea breath test, conducted at least 4 weeks after completion of eradication therapy. Breath samples before and 20 minutes after administration of 38 mg 13C-urea were collected6 measured by mass spectrometry (Heliview; MediChems, Seoul, Korea), and cutoff value was 2.0‰. This method is illustrated by flowchart (Fig. 1).

Endpoints
Primary endpoint was H. pylori eradication rate calculated by ITT and PP analysis after 4–6 weeks of treatment. Eradication rate of ITT was defined as percentage of subjects determined successful in eradication of all subjects that took the drug for the purpose of participating in the study including those that discontinued medication because of adverse events, or those that were not followed up. PP eradication rate was expressed as percentage of patients that completed the study. Secondary endpoints included compliance and adverse events.
Statistical analysis
Sample size for first-line therapy was according to the following: estimated proportion of successful eradication in both groups of 82.5%, non-inferiority delta (or epsilon) of 10%, one-sided alpha level of 0.05 and power of 80%. Considering a dropout rate of 10%, 199 patients were required in both groups. As for second-line therapy, estimated proportion of successful eradication in both groups of 86%, non-inferiority delta (or epsilon) of 20%, one-sided alpha level of 0.05 and power of 80%. Considering a dropout rate of 20%, 47 patients were required in both groups.
Patients' categorical data were presented as mean ± standard deviation. The χ2 test or Fisher's exact test were applied to compare characteristics of patients and results of the two groups. The t-test was used to evaluate continuous variables. Both univariate and multivariate analyses were conducted. A level of statistical significance was established at P < 0.05 for all analyses. Statistical analyses were conducted using SAS ver. 9.4 (SAS Institute Inc., NC, Cary, USA).
RESULTS
H. pylori eradication rates in first-line therapy
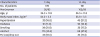
Baseline characteristics of patients in first-line therapy group are shown in Table 1. In total, 369 patients were included in this study. In 7-day group and 14-day group, proportion of men was 53.4% and 53.4%, respectively. Mean ages were 54.3 ± 11.8 and 54.5 ± 11.5, 21.8% and 17.3% were smokers and 40.5% and 47.8% were drinkers, respectively. Proportion of patients with diabetes was 11.0% and 10.9%, respectively. Proportion of patients with hypertension was 16.8% and 21.2%, respectively. Follow up losses were 33 (18.5%) and 33 (17.3%), respectively. There were two dropouts due to side effects of abdominal pain in the 7-day group.
Table 1
Baseline characteristics of first-line therapy with standard triple therapy
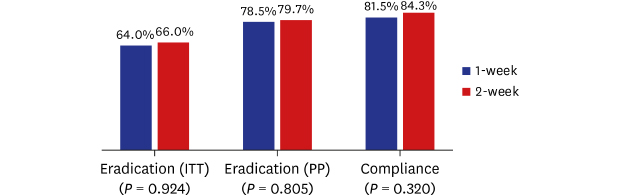
Results of eradication in first-line therapy group are shown in Fig. 2. Eradication rate was 78.5% (95% confidence interval [CI], 70.6%–85.1%; n = 106/135) and 79.7% (95% CI, 72.2%–86.0%; n = 114/143) in the 7-day and 14-day treatment in the PP analysis (P = 0.805). In ITT analysis, eradication rate was 64.0% (95% CI, 56.5%–71.1%; n = 114/178) and 66.0% (95% CI, 58.8%–72.7%; n = 126/191), respectively (P = 0.924). There was no significant difference in drug compliance (81.5% [n = 145/178] vs. 84.3% [n = 161/191]; P = 0.320).
Fig. 2
The results of standard triple therapy with PPI + amoxicillin + clarithromycin as first-line therapy. In ITT analysis, eradication rate was 64.0% and 66.0% respectively (P = 0.924). Eradication rate was 78.5% and 79.7% in the 7-day and 14-day treatment in the PP analysis (P = 0.805). There was no significant difference in drug compliance between both groups (P = 0.320).
PPI = proton pump inhibitor, ITT = intention-to-treat, PP = per-protocol.

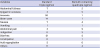
Adverse event rate was higher in the 14-day regimen (15.7% vs. 20.9%; P = 0.042). Interestingly, there were 5 patients in the 7-day group and no patients in the 14-day group who were uncomfortable to affect daily activities or discontinued H. pylori medications. Frequently reported adverse events were diarrhea, anorexia, and bitter taste. Abdominal fullness, epigastric soreness, nausea, abdominal pain, indigestion, general weakness, vomiting, dizziness, weight loss, dysuria, edema were also reported (Table 2).
Table 2
Adverse events during taking eradication medication
Presence or absence of diabetes (71.0% vs. 64.9%; P = 0.781) did not affect the eradication rate. Additionally, presence or absence of hypertension (68.5% vs. 64.8%; P = 0.571) also did not influence the eradication rate.
H. pylori eradication rates in second-line therapy
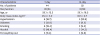
Baseline characteristics of patients in second-line therapy group are shown in Table 3. In total 96 patients were included in the second-line therapy group. In 7-day group and 14-day group, proportions of men were 45.5% and 44.2%, respectively. Follow-up losses was 4 in each group. There was one dropout in each group, due to drug failure because of nausea and vomiting.
Table 3
Baseline characteristics of second-line therapy with bismuth containing quadruple therapy
Results of eradication in second-line therapy group are shown in Fig. 3. Eradication success rates of second-line therapy were 79.6% (95% CI, 64.7%–90.2%; n = 35/44) in 7-day group and 90.4% (95% CI, 79.0%–96.8%; n = 47/52) in 14-day group (P = 0.080) in ITT analysis, 91.7% (95% CI, 77.5%–98.3%; n = 33/36) and 100% (n = 45/45) (P = 0.084) in PP analysis, respectively. Drug compliances were 95.5% (n = 42/44) and 98.1% (n = 51/52) (P = 0.728), adverse event rates were 20.5% and 9.6% (P > 0. 099), respectively. Frequently reported adverse events were abdominal fullness and nausea. Epigastric soreness, anorexia, bitter taste, vomiting, dizziness, abdominal pain, indigestion, diarrhea, constipation, myalgia, and skin rash were also reported (Table 2).
Fig. 3
The results of second-line therapy with PPI + bismuth + metronidazole + tetracycline. Eradication rate of second-line therapy was 79.6% and 90.4% in 7-day and 14-day treatment (P = 0.080) in ITT analysis. There was no difference between 7-day and 14-day treatment in PP analysis (91.7% vs. 100%, P = 0.084). Drug compliances were not significantly different in both groups (P = 0.728).
PPI = proton pump inhibitor, ITT = intention-to-treat, PP = per-protocol.

DISCUSSION
We demonstrated here that 14-day treatment for H. pylori eradication did not yield better results as compared to 7-day treatment. H. pylori eradication success rates were less than 80% for 7-day and 14-day treatment in ITT and PP analysis, indicating that both may be unsuitable for first-line therapy. Guidelines from the Korean Society of Gastroenterology suggest STT for 7–14 days as first-line therapy. Currently, most Korean doctors prefer 7-day, because 7-day treatment was not inferior to 14-day treatment.7 Recent studies revealed the eradication rate was 5%–9% improvement in 14-day treatment compared to 7-day during the past 10 years in Korea.1 However, this was not a prospective study. In systemic review of Korea, eradication rate of PPI-based triple therapy for 7 days (20 studies) was 71.1% for ITT and 78.5% for PP, while those for 14 days (5 studies) was 76.4% for ITT and 85.2% for PP.8 In the Cochrane study, the prolongation of duration of PPI-based triple therapy from 7 days to 14 days significantly increased eradication rate of H. pylori in the subgroup of STT in 34 studies (relative risk, 0.65; number needed to treat, 12), suggesting the ideal duration of STT would be at least 14 days.5 Another study conducted in Canada identified 14-day treatment as superior to 10-day treatment, the problem of which was the small number of subjects (n = 83).9 Several studies were conducted to substitute existing first-line treatment in Korea. As an alternative to STT, various therapies are presented and are constantly challenging. Among them, concomitant therapy (PPI + amoxicillin + metronidazole + clarithromycin), 10-day ST (PPI + amoxicillin for 5 days and PPI + clarithromycin + metronidazole/tinidazole in the following 5 days), 14 days of hybrid therapy (1-week dual treatment with PPI and amoxicillin followed by 1-week concomitant therapy), 10 or 14 days of levofloxacin based triple treatment was introduced. However, results were unsatisfactory. The new therapy is not a distinct effect than conventional therapy and it may be due to antibiotic resistance. That's why new treatments do not replace conventional therapy. In this study, STT did not reveal adequate results.
Clarithromycin resistance increased from 17% to 37% in Korea, and this high clarithromycin resistance rate is related to eradication failure.1011 In countries where antibiotic resistance is high, such as in Korea, bismuth treatment is the most preferred treatment. The American College of Gastroenterology Clinical Guidelines in 2017 suggest that STT consisting of PPI, clarithromycin, and amoxicillin for 14 days is the recommended treatment in areas wherein H. pylori clarithromycin resistance is less than 15%.12 The Maastricht V/Florence Consensus Report did not recommend ST. Fourteen-day bismuth quadruple therapy was recommended for high clarithromycin and metronidazole resistance (> 15%).13 Recent reviews suggest that therapy with PBMT is an alternative first-line therapy useful when resistance to clarithromycin and metronidazole is common.14 Although European guidelines recommend that an antibiotic resistance test be administered in case of failure in secondary eradication, it is troublesome and costly to test, and it cannot be conducted in all hospitals.15 However, currently used guidelines recommend standard triple regimen as first-line therapy, and patients receiving second-line therapy due to low eradication rate account for approximately 20%–30% of all patients. As a result, problems such as prolongation of treatment period, increased cost, side effects due to use of antibiotics, generation of resistant bacteria, etc. may occur. Additionally, it is unclear that the 14-day therapy is more effective than the 7-day therapy.716 It is time to re-evaluate the efficacy of STT as empirical first-line therapy and to re-establish a first-line treatment in Korea.
Therefore, new first-line therapy is needed. Which regimen to use as secondary treatment should be considered. Existing primary therapies must be customized through antibiotic resistance studies. It is initially costlier, but will be cost effective in the long term. Because it is difficult to determine new primary and secondary treatments, increasing the treatment period to 14-day therapy may be an option before a new treatment is established. Although not statistically significant, 14-day therapy increased the eradication rate. There was a study showing good eradication rates in Korea where antibiotic resistance rates were high.17
In terms of second-line therapy, there was a study that compared 10-day ST and 14-day PBMT therapy for patients with eradication failure. Eradication rates were similar in both groups (49% vs. 42.5%), however, better compliance and fewer side effects were revealed in patients with ST.18 In Korean studies, PBMT (7-day to 10-day) therapy revealed significantly higher eradication rate than 10-day ST (84.3% vs. 56.8%) despite higher side effects.19 It is recommended to administer second treatment from 7 to 14 days of bismuth-containing quadruple therapy in Korea. There were studies comparing treatment effects on 7- and 14-day PBMT treatments. Eradication success rate of treatment on the 14-day treatment was 82.6%–85.1% in ITT analysis, 93.6%–96.2% in PP analysis, higher than 7 days of treatment in two studies. Frequency of side effects was similar in both groups.2021 However, in another study, 7-day PBMT may be effective as 14-day PBMT (83.5% vs. 87.7% in ITT and 87.7% vs. 88.9% in PP analysis).22 In our study, there was no statistical significance, but success rates were high in the 14-day group. The problem with PBMT is the poor compliance due to side effects. In the present study, drug compliance rates were high, it is noteworthy that there were fewer drug adverse events than expected. Clinically, if there would be no major side effects after taking a 7-day second-line therapy, it may be recommended to take it 14 days. Another problem is that bismuth is not available globally. Therefore, other treatments are needed in areas where bismuth is not available. If bismuth would be available, PBMT can be recommended as empirical first-line therapy instead of STT in regions wherein antibiotic resistance to clarithromycin and metronidazole is higher than 30%.1123 It is also possible to use bismuth in Korea, in addition, the success rate of STT is gradually decreasing, so it should consider changing the first-line therapy as PBMT. Research is needed to determine if twice daily doses are equally effective as four times a day because patients have difficulty taking four times a day.
The advantage of our study is that it is a prospective study. Most existing Korean studies are based on retrospective studies. There was no head-to-head study comparing the 7- and 14-day treatment since 2008. Based on this study, it is time to change first-line treatment. Additionally, patients with compliance greater than 85% were included. However, there are several limitations to our study. The numbers of dropout and follow-up loss were high in patients with first-line therapy. Therefore, the number of patients receiving second-line therapy was small in our study. To overcome this, additional registrations (n = 33) were made. These were patients who were referred to the first-line therapy failure at a private clinic during the study period, which might act as a confounding factor. Secondly, the present study was conducted in and around Seoul, not across the country. Lastly, clarithromycin resistance was not checked. Considering that the Clarithromycin-resistance rate of H. pylori is high in Korea, the existence of antibiotic resistance is crucial. Tailored therapy by the result of clarithromycin resistance is likely to increase the success rate of H. pylori eradication, but these studies are needed because current practice often uses empirical treatment rather than tailored therapy.
In summary, success rates of H. pylori eradication with PPI-clarithromycin-amoxicillin triple therapy were less than 80% regardless of treatment duration, PPI-based STT for H. pylori was not efficient as a first-line therapy in Korea. Although bismuth-containing quadruple therapy for 14 days as a second line therapy tended to show higher eradication rate compared to 7-day therapy, this should be elucidated by further larger scaled studies.
 XML Download
XML Download