

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
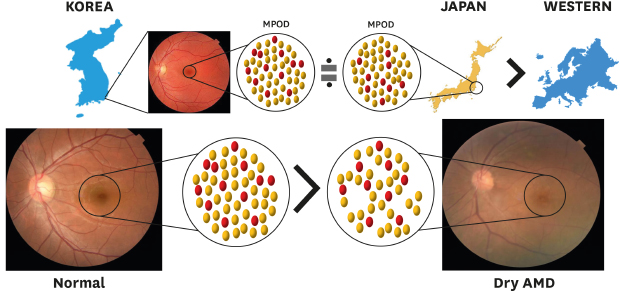
Age-related macular degeneration (AMD) is a leading cause of legal blindness among elderly individuals in industrialized countries.1 Although the pathogenesis of AMD remains poorly understood, the mechanisms believed to be causative include genetic factors, cumulative light damage, free radical injury, and hemodynamic processes.234 At least in part, the putative role of all of these processes can be attributed to oxidative retinal injury.5 The macular pigment (MP) is composed of the hydroxy-carotenoids lutein, zeaxanthin, and meso-zeaxanthin; it is concentrated at the center of the retina and decreases rapidly with increasing eccentricity.3 MP is thought to protect the retinal photoreceptors and retinal pigment epithelium primarily via its antioxidant properties and role as a filter for short wavelength blue light; and is believed to play a beneficial role in visual performance.678910 Therefore, it has been demonstrated that healthy individuals with higher MPs experience less disability glare and demonstrate better photo-stress recovery times.89
Currently, MP is studied mainly because of the proposed link between low levels of macular pigment optical density (MPOD) and an increased risk of developing AMD.311 MP protects against AMD,12 and the Eye Disease Case-Control Study (EDCC) reported that a high dietary intake and high serum levels of lutein and zeaxanthin were associated with a reduced risk of developing AMD.13 Furthermore, reduced concentrations of lutein and zeaxanthin have been demonstrated in the macula and whole retina of human donor eyes with early AMD compared with control subjects.14 Previous reports have described that dietary supplementation of carotenoids can increase MPOD,15 which has been shown to be positively correlated with MPOD in healthy subjects and also increase MPOD in AMD patients. Thereby, they elicit an improvement in visual function including visual acuity, contrast sensitivity, and subject glare recovery.1617 Thus, measurements of MPOD may be beneficial in evaluating the risk of AMD and the treatment effects of oral supplementation of carotenoids.
The macular pigment screener II (MPSII®; Elektron Eye Technology, Cambridge, UK), which is based on heterochromatic flicker photometry (HFP), is now commercially available. In this method, the difference in the intensities of blue (absorbed by the MP) and green (not absorbed by the MP) wavelengths of flickering light, which can be recognized in the fovea (where MPs accumulate) and para-fovea (where MPs are more scarce), are measured to estimate the level of macular pigment that blocks the blue wavelength of light and increases the threshold to recognize blue light by photoreceptor cells. Subtraction of the para-foveal threshold from the foveal threshold is performed to approximate MPOD.
Previous studies have reported that the estimated MPOD value obtained by MPSII® is applicable to not only healthy individuals but also subjects with AMD.18 Ozawa et al.18 reported that measurements of MPOD using MPSII® may be crucial to better understand the role of MP in the pathogenesis of AMD.
However, to the best of our knowledge, changes in MPOD using MPSII® according to age have not yet been investigated, and there have been no reports on the differences in MPOD obtained by MPSII® according to the presence and absence of AMD in the Korean population. In the present study, we analyzed the changes in MPOD measured by MPSII® according to age, and analyzed the differences in MPODs according to the presence or absence of AMD in the Korean population.
METHODS
Subjects
The retrospective review of medical records was performed in the Department of Ophthalmology of Busan Paik Hospital (Busan, Korea) with data collected from November 2018 to January 2019. The subjects were not included if they had a history of glaucoma, uveitis, diabetic retinopathy (diabetic patients without diabetic retinopathy were included), or neovascular AMD. Other exclusion criteria were the presence of media opacity or vitreous opacity that would prevent the examination of the retina and optical coherence tomography (OCT) imaging, and a history of prior laser treatment or vitrectomy surgery. We excluded the subjects who underwent cataract surgery within a year. The eyes with high myopia (> −6.00 diopter or an axial length over 26 mm) were also excluded.
We randomly selected a single eye from the subjects who did not meet the exclusion criteria. And then, the subjects were divided into four groups according to age: Group 1, 30–39 years; Group 2, 40–49 years; Group 3, 50–59 years; and Group 4, 60–79 years. In addition, subjects aged > 50 years were further divided into two subgroups according to the presence of dry AMD (early or intermediate AMD).19 Each group was further used for statistical analysis.
A detailed ophthalmologic examination, which included a measurement of the best-corrected visual acuity (BCVA), slit-lamp examination, and fundus examination, was performed. All subjects underwent additional examinations using a retinal camera (Topcon TRC 50DX, Topcon Corporation, Tokyo, Japan), Optos California® (Optos PLC, Dunfermline, Scotland, UK), and OCT using a Zeiss OCT system (Cirrus HD-OCT 5000, Carl Zeiss Meditec Inc., Dublin, CA, USA) to evaluate their retinal status.
The estimated values of MPOD were measured using the MPSII® macular densitometer, which uses an HFP technique. The mechanism of estimating MPOD with MPSII® has been addressed elsewhere.2021 The stimulus consists of blue light wavelength (465 nm) and green light wavelength (530 nm). The light target has a circular aperture with 1° in diameter; then, we can obtain MPOD with this instrument from the 0.5° (ca 150 μm) around foveal center.20 The subjects were asked to focus on a light target and to respond to the flickering by pushing a button on the machine immediately. The measurement was performed before pupil dilation, and when measurement errors were obtained twice, the result was recorded as non-measurable and subsequently the subjects were excluded. Before the measurement, information of the phakic eye or pseudophakic eye was entered, and the year of the cataract surgery was entered for subjects with pseudophakic eyes.
Statistical analysis
The data were analyzed using SPSS ver. 21.0 (IBM Corp., Armonk, NY, USA), and all results were expressed as the mean ± standard deviation. Spearman's correlation test was used to evaluate the correlations between the MPOD and age. A simple linear regression analysis was performed to determine the association between MPOD and age. The post hoc analysis with Bonferroni correction was used to compare MPODs among the four groups, and the Mann-Whitney U test was utilized to compare MPODs between the dry AMD group and the elderly controls. Moreover, the effects of diabetes mellitus, hypertension, dyslipidemia, and smoking on MPOD were analyzed using a logistic regression analysis. A P value of < 0.05 was accepted as statistically significant.
Ethics statement
Approval for data collection and analysis was obtained from the Institutional Review Board at Busan Paik Hospital, Inje University (approval No. 19-0024), and the requirement for individual consent was waived due to retrospective study. This study was performed in adherence with the tenets of the Declaration of Helsinki.
RESULTS
A total of 126 eyes of 126 individuals (51 men, 75 women; aged 30–79 years; mean age, 56.15 ± 12.33 years) were included. Among the subjects, 19 eyes (15%) were included in Group 1 (30–39 years of age), 17 eyes (13%) were included in Group 2 (40–49 years of age), 41 eyes (33%) were included in Group 3 (50–59 years of age), and 49 eyes (39%) were included in Group 4 (60–79 years of age). There were no statistically significant differences in the mean BCVA among the groups (P = 0.032). The baseline characteristics of the individuals are summarized in Table 1.
Table 1
Baseline characteristics of all subjects

The mean estimated MPOD values measured by MPSII® of all subjects was 0.59 ± 0.20, 0.72 ± 0.08 in Group 1, 0.70 ± 0.09 in Group 2, 0.60 ± 0.17 in Group 3, and 0.57 ± 0.23 in Group 4. Groups 1 and 2 exhibited higher estimated MPOD values compared to Groups 3 and 4 (Bonferroni correction). There were no significant differences between Groups 1 and 2 (Mann-Whitney U test, P = 0.528), or between Groups 3 and 4 (Mann-Whitney U test, P = 0.641). The details of each group are described in Tables 2, 3, and Fig. 1. According to Spearman's correlation analysis, the MPOD significantly decreased with increasing age (Spearman's correlation coefficient, −0.239; P = 0.008). In the simple regression analysis, a statistically significant linear regression was observed, and the estimated values of MPOD decreased by 0.005 as the age increased by 1 year (P = 0.001, estimated MPOD value = 0.884 − 0.005 × age) (Figs. 2 and 3).
Table 2
The differences of the estimated values of the MPOD

| Variables | Group 1 | Group 2 | Group 3 | Group 4 |
|---|---|---|---|---|
| Estimated MPOD values | 0.72 ± 0.08 | 0.70 ± 0.09 | 0.60 ± 0.17 | 0.57 ± 0.23 |
Table 3
Statistical comparisons by Bonferroni correction were described for each group
Fig. 1
Groups 1 and 2 exhibited higher estimated MPOD values compared to Groups 3 and 4 (Bonferroni correction). Group 1, 30–39 years of age; Group 2, 40–49 years of age; Group 3, 50–59 years of age; Group 4, 60–79 years of age.
MPOD = macular pigment optical density.
Fig. 2
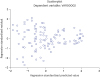
In the simple regression analysis, a statistically significant linear regression was observed, and the estimated values of MPOD decreased by 0.005 as the age increased by 1 year (P = 0.001, estimated MPOD value = 0.884 − 0.005 × age).
MPOD = macular pigment optical density.

Fig. 3
Scatterplot showing the correlation between the expected changes in MPOD and the age by simple regression analysis.
MPOD = macular pigment optical density.
After confirming that the MPOD was significantly decreased in subjects over 50 years of age, the changes in MPOD according to age were analyzed again, except for patients over 50 years of age with dry AMD who had drusen on the macula. After that, the Groups 3 and 4 were renamed "healthy Group 3” and “healthy Group 4,” respectively. Subsequently, 14 eyes (34%) of Group 3 and 26 eyes (53%) of Group 4 had drusen, and 27 eyes (66%) of Group 3 were included in healthy Group 3, and 23 eyes (47%) of Group 4 were included in healthy Group 4. In Groups 1 and 2, there was no significant lesion of the macula. The estimated values of MPOD then exhibited a decreasing trend with increasing age, but there were no statistically significant differences among the four groups (Tables 4 and 5). An analysis using Spearman's correlation test and simple regression analysis was also performed. As a result of Spearman's correlation analysis in healthy subjects, there was no statistically significant correlation between MPOD and age (P = 0.201).
Table 4
The differences of the estimated values of the MPOD in the Groups 1, 2, Healthy groups 3 and 4

| Variables | Group 1 | Group 2 | Healthy group 3 | Healthy group 4 |
|---|---|---|---|---|
| Estimated value of the MPOD | 0.72 ± 0.08 | 0.70 ± 0.09 | 0.64 ± 0.16 | 0.61 ± 0.25 |
Table 5
Statistical comparisons by Mann-Whitney U test were described for each group

| Intergroup differences | Group 1 | Group 2 | Healthy group 3 | Healthy group 4 |
|---|---|---|---|---|
| Group 1 | N/A | 0.528 | 0.083 | 0.298 |
| Group 2 | 0.528 | N/A | 0.195 | 0.412 |
| Group 3 | 0.083 | 0.195 | N/A | 0.738 |
| Group 4 | 0.298 | 0.412 | 0.738 | N/A |
To compare the MPOD in patients with dry AMD and in healthy controls, subjects aged > 50 years were categorized as patients with dry AMD and healthy controls. The mean estimated MPOD values that were measured by MPSII® were 0.69 ± 0.18 in the healthy controls and 0.55 ± 0.17 in patients with dry AMD. The estimated MPOD values in the patients with dry AMD were significantly lower than those in the healthy controls (Mann-Whitney U test, P = 0.001).
Additionally, a logistic regression analysis was performed to evaluate the effect of diabetes mellitus, hypertension, dyslipidemia, and smoking on the reduction of MPOD and the occurrence of dry AMD. A logistic regression analysis was performed to identify significant predictors of dry AMD or reduction in MPOD in the presence of hypertension (odds ratio [OR], 1.42; 95% confidence interval [CI], 0.67–1.70], dyslipidemia (OR, 2.01; 95% CI, 1.10–1.84), and smoking history (OR, 2.74; 95% CI, 1.91–3.91). However, diabetes mellitus showed no statistically significant association with decreases in MPOD or occurrence of dry AMD (Table 6). Because the present study included diabetic patients whose glucose level had been well controlled (hemoglobin A1c [HbA1c] < 7.5), no significant correlation was also found between HbA1c and MPOD (Spearman's correlation analysis, P = 0.351).
Table 6
OR (95% CI) for predictors of reduction of MPOD and occurrence of dry AMD among subjects older than 50 years old

| Variables | Dry AMD patients | ||
|---|---|---|---|
| Adjusted OR | 95% CI | P value | |
| Diabetes mellitus | 1.07 | 0.67–1.70 | 0.743 |
| Hypertension | 1.42 | 1.10–1.84 | 0.047a |
| Dyslipidemia | 2.01 | 1.61–2.51 | 0.021a |
| Smoking | 2.74 | 1.91–3.91 | 0.008a |
DISCUSSION
MP may protect against AMD because of its capability to absorb blue light and scavenge free radicals.22 Because the MP is entirely of dietary origin, a protective effect would have important health care implications.23 A preventive approach involving micronutrient supplementation based on the results from large clinical studies, including the Age-related Eye Disease Study (AREDS) and AREDS2, is currently attracting attention.2425 Measuring MP to diagnose subjects who need nutritional supplements may be important in preventing AMD.
There are several methods to measure MPOD including fundus reflectance spectroscopy, scanning laser ophthalmoscope, and HFP, all of which have been demonstrated to have significant bivariate correlation coefficients.22 Among these methods, HFP is the most widely used method of assessing MPOD.22 A small visual stimulus emits alternating light of two different wavelengths, blue light that is absorbed by the MP, and green light which is not absorbed by the MP in the retina.2627 MP has its peak at fovea and decreases with eccentricity, and flicker-based techniques typically use a central and peripheral measurement point. The peripheral measurement is used as a reference point for the central measurement and is assumed to be zero.
In the era of MPSII®, the reliability of MPSII® as well as the correlation between the absolute value and the estimated value of MPSII® have been reported. Obana et al.21 demonstrated that using MPSII®, intraclass correlation coefficients (ICC) of the estimated and absolute values were almost perfect (ICC: 0.75, 0.80). The mean estimated and absolute MPODs did not differ significantly (P = 0.427, paired t-test) and the Pearson correlation coefficient between the estimated and absolute MPODs were significant (P < 0.001). Additionally, Ozawa et al.18 reported that there were significant correlations between both values in all subjects: young healthy subjects, aged healthy subjects, AMD-fellow and AMD subjects. Furthermore, both values were measurable in 100% of the eyes in young healthy patients; however, in the aged groups, absolute MPOD values were measurable in only 56.7% of patients, while estimated values were measurable in 88.3% of patients in their study. In contrast, estimated values of MPOD using MPSII®, for which the influence of cataract and statue of intraocular lens was mitigated, may be more useful for evaluating MPOD over all ages with or without AMD. Additionally, MPSII® was previously validated mainly in a white population20 and in an Asian population with pigmented skin, especially in Japan.21
In the present study, we also studied MPS, which can be used to measure MPOD regardless of age or AMD. We demonstrated the changes in MPOD according to age from 30 to 79 years and the difference in MPOD according to the presence of dry AMD in subjects over 50 years of age.
Previously, the mean absolute MPOD of more than 5,000 participants was reported to be 0.33 ± 0.19 in patients aged 20 to 60 years, most of whom appeared to be Caucasians from the Netherlands.20 Abell et al.28 reported that the mean absolute MPOD in an Australian population was 0.41 ± 0.20. The mean estimated MPODs with MPSII® in our study subjects was 0.59 ± 0.20, which was higher than those of previous studies. However, unlike the Western reports, MPOD studies on Asian populations have demonstrated that Asians tend to have higher MPODs than Caucasian populations.29 MPOD measurements in the Japanese population showed high values both in absolute MPOD (0.63 ± 0.18) and estimated MPOD (0.64 ± 0.17) compared to a previous study with Caucasian populations. These results suggest that the differences in MPOD were influenced by the ethnic differences. Our MPOD measurement of the Korean population was also similar to the estimated values of Asian populations, supporting our assumption that MPOD differs according to race. However, there has been no inter-racial study comparing MPODs, and a large-scaled study including different races is warranted to confirm the differences of MPODs between the ethnicities.
We found that significantly lower MPODs were observed in the population aged ≥ 50 years of age than in the population aged < 50 years of age, and a negative correlation was indicated by Spearman's correlation analysis. However, there was no significant decrease in MPOD with age among healthy subjects after excluding AMD patients. To analyze the correlation between AMD and MPOD in patients older than 50 years, the MPOD was significantly lower in the subjects with AMD compared to the subjects without AMD.
In 2000, Hammond and Caruso–Avery reported a statistically significant inverse relationship between the optical density of MP and age.30 However, most other studies that used HFP found no age effect.313233 Ciulla and Hammond34 have reported that MPOD decreases with age, even in subjects with cataracts and AMD. In a recent study, Ozawa et al.18 demonstrated that there was no significant change in MPOD with age in healthy subjects, and there was a significantly lower MPOD in the eyes with AMD and AMD-fellow eyes compared with aged healthy eyes. In the current study, the reason for the significant decrease in MPOD in patients older than 50 years was thought to be the inclusion of patients with AMD. Except for AMD patients, there was no significant difference in MPOD with age, consistent with most previous studies. Among the subjects aged 50 years or older, patients with AMD showed significantly lower MPODs compared to heathy controls, which was also consistent with other previous reports.
Recently, there is a growing interest in the potential role of MP including lutein and zeaxanthin. MP protects the macula from photooxidation via its light-screening capacity and antioxidant activity35 to help prevent the development and progression of AMD. And, based on the results of this study, patients with dry AMD showed a significant lower MPOD, which meant that the patients lost the protective ability of MP, thereby lower MPOD may be the risk in the development of AMD. Many studies including EDCC have demonstrated that low MP is a risk factor for developing dry AMD, and dietary supplements with lutein and zeaxanthin have been recommended for decreasing the risk of dry AMD. Because the foveal MPOD is increased by dietary supplementation of lutein, zeaxanthin, and docosahexaenoic acid,36 a sufficient intake of these supplements is important, especially for patients with AMD. Risk factors for dry AMD include age, smoking, cardiorespiratory disease, diet, dyslipidemia, exposure to ultraviolet rays, race, and decreased MP.37383940 Similar to the previous study, hypertension, dyslipidemia, and smoking were risk factors for dry AMD or reduction of MPOD in AMD patients in the present study. Among these, MPOD is one of the modifiable factors and can be calculated. Measurement of MPOD using MPS II is expected to increase the macular protective effect by allowing subjects with low MPOD to take supplements.
Our study has some limitations. First, the study sample was relatively small, and further research with a larger sample is required. Second, because the focus was exclusively on AMD, the applicability of this technique to other diseases remains unclear. Third, analyses of the relationship between serum or dietary carotenoid levels and MPOD were not conducted. Finally, we haven't revealed a significant correlation between MPOD reduction and the occurrence of AMD. However, to the best of our knowledge, this study was the first to demonstrate the changes in MPOD according to age and difference in MPOD with and without AMD in Korean populations. Additionally, estimated values using MPSII® were measurable in all ages, especially old patients who might have dry AMD. The results of this study may lead to an increased use of MPSII® in practice and to identify the need of dietary supplementation in patients with lower MPOD. Future studies are needed to evaluate the effect of MPOD on the pathogenesis of AMD and MPOD levels in other diseases. Further information regarding the MPOD changes according to the amount of dietary supplementation would contribute to patient care.
In conclusion, the MPOD measured with MPSII® reflects the MP density in healthy individuals and in patients with dry AMD. Our results showed that aging was not significantly associated with low MPOD, but the presence of dry AMD was significantly associated with low MPOD. Therefore, we hypothesized that low MPOD may be a risk factor for developing dry AMD, and thus dietary supplementation of lutein and zeaxanthin is important in patients with lower MPOD. Furthermore, routine screening with MPS II® for ages 50 and older is thought to help detect early low MPOD and identify individuals who should take supplements.
 XML Download
XML Download