

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Soo Hyun Kim, MD , Kye jin Park, MD, Mi Hyun Kim, MD, Jeong Kon Kim, MD
, Kye jin Park, MD, Mi Hyun Kim, MD, Jeong Kon Kim, MD
, Kye jin Park, MD, Mi Hyun Kim, MD, Jeong Kon Kim, MD
Abstract
The diagnosis rates of small renal masses less than 4 cm in diameter are increasing with the increasing number of CT and MRI examinations. Since these small renal masses include a high proportion of benign tumors and low-malignant renal cell carcinomas, image-guided biopsy plays an important role in facilitating accurate diagnosis, low-invasive percutaneous radiofrequency- or cryo-ablation, and active surveillance for these masses. Therefore, the diagnostic accuracy and safety of image-guided biopsy for small renal masses, but awareness of the technical aspects of image-guided percutaneous ablation and an understanding of active surveillance are crucial in establishing an adequate treatment plan. The purpose of this review is to present the basic knowledge and clinical usefulness of the diagnosis trends for small renal masses, discuss the diagnostic accuracy of imaging-guided biopsy, and assess the use of low-invasive therapy with percutaneous ablation and active surveillance.
Figures and Tables
 | Fig. 1Suggested algorithm for the management of SRMs. RMB depicts the clinical scenarios in which RMB can be considered.
*When technically feasible.
†Benign pathology, chromophobe, papillary type 1, or Fuhrman grade 1 to 2 mRCC.
AS = active surveillance, CCI = Charlson Comorbidity Index, mRCC = metastatic renal cell carcinoma, PN = partial nephrectomy, QOL = quality of life, R.E.N.A.L. = Radius, Exophytic/endophytic properties, Nearness of tumor to the collecting system or sinus in millimeters, Anterior/posterior Location relative to polar lines, RMB = renal mass biopsy, SRMs = small renal masses, TA = thermal ablation
|
 | Fig. 2A case of successful radiofrequency ablation for renal cell carcinoma in a 70-year-old female patient.
A. MRI shows a contrast-enhancing mass in the left kidney.
B. The mass closely abuts the descending colon in the prone position.
C. Hydrodissection ensured sufficient space between the mass and the descending colon.
D. Radiofrequency ablation was performed for the renal mass.
E. The CT image obtained immediately after ablation shows no residual contrast enhancement in the renal mass.
F. The CT image obtained 24 hours after ablation shows a completely ablated mass without complication.
|
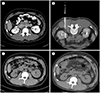 | Fig. 3A case of bowel perforation after radiofrequency ablation for renal cell carcinoma in a 57-year-old male patient.
A. CT image shows a 2-cm recurrent mass in the left kidney after right partial nephrectomy for renal cell carcinoma.
B. Radiofrequency ablation was performed for the recurrent tumor in left kidney.
C. Immediately after the ablation, there was no ablation-related complication on CT images.
D. At 24 h after ablation, the patients complained of persistent abdominal pain. CT images obtained 24 h after the procedure show pneumoperitoneum (arrows) caused by perforation of the ileal loop.
|


Table 3
Summary of the Published Guideline Criteria and Follow-Up for AS of SRMs

*Depending on the patient's comorbidities and life expectancy.
AML = angiomyolipoma, AS = active surveillance, ASCO = American Society of Clinical Oncology, AUA = American Urological Association, CXR = chest X-ray, EAU = European Association of Urology, ESRD = end-stage renal disease, NCCN = National Comprehensive Cancer Network, RCC = renal cell carcinoma, RMB = renal mass biopsy, SRM = small renal mass, US = ultrasound
![]()
Acknowledgments
This work was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (2017R1A2B3007567).
References
1. Welch HG, Skinner JS, Schroeck FR, Zhou W, Black WC. Regional variation of computed tomographic imaging in the United States and the risk of nephrectomy. JAMA Intern Med. 2018; 178:221–227.
2. Bhindi B, Lohse CM, Mason RJ, Westerman ME, Cheville JC, Tollefson MK, et al. Are we using the best tumor size cut-points for renal cell carcinoma staging? Urology. 2017; 109:121–126.
3. Finelli A, Ismaila N, Bro B, Durack J, Eggener S, Evans A, et al. Management of small renal masses: American Society of Clinical Oncology clinical practice guideline. J Clin Oncol. 2017; 35:668–680.
4. Sanchez A, Feldman AS, Hakimi AA. Current management of small renal masses, including patient selection, renal tumor biopsy, active surveillance, and thermal ablation. J Clin Oncol. 2018; JCO2018792341.
5. Campbell S, Uzzo RG, Allaf ME, Bass EB, Cadeddu JA, Chang A, et al. Renal mass and localized renal cancer: AUA guideline. J Urol. 2017; 198:520–529.
6. Pierorazio PM, Johnson MH, Patel HD, Sozio SM, Sharma R, Iyoha E, et al. AHRQ comparative effectiveness reviews. In : Rockville MD, editor. Management of renal masses and localized renal cancer. Rockville: Agency for Healthcare Research and Quality;2016.
7. Patel HD, Johnson MH, Pierorazio PM, Sozio SM, Sharma R, Iyoha E, et al. Diagnostic accuracy and risks of biopsy in the diagnosis of a renal mass suspicious for localized renal cell carcinoma: systematic review of the literature. J Urol. 2016; 195:1340–1347.
8. Marconi L, Dabestani S, Lam TB, Hofmann F, Stewart F, Norrie J, et al. Systematic review and meta-analysis of diagnostic accuracy of percutaneous renal tumour biopsy. Eur Urol. 2016; 69:660–673.
9. Harisinghani MG, Maher MM, Gervais DA, McGovern F, Hahn P, Jhaveri K, et al. Incidence of malignancy in complex cystic renal masses (Bosniak category III): should imaging-guided biopsy precede surgery? AJR Am J Roentgenol. 2003; 180:755–758.
10. Lang EK, Macchia RJ, Gayle B, Richter F, Watson RA, Thomas R, et al. CT-guided biopsy of indeterminate renal cystic masses (Bosniak 3 and 2F): accuracy and impact on clinical management. Eur Radiol. 2002; 12:2518–2524.
11. Bosniak MA. Should we biopsy complex cystic renal masses (Bosniak category III)? AJR Am J Roentgenol. 2003; 181:1425–1426.
12. Herts BR, Baker ME. The current role of percutaneous biopsy in the evaluation of renal masses. Semin Urol Oncol. 1995; 13:254–261.
13. Hong K, Georgiades C. Radiofrequency ablation: mechanism of action and devices. J Vasc Interv Radiol. 2010; 21:S179–S186.
14. Goldberg SN, Gazelle GS, Solbiati L, Rittman WJ, Mueller PR. Radiofrequency tissue ablation: increased lesion diameter with a perfusion electrode. Acad Radiol. 1996; 3:636–644.
15. Baust JG, Gage AA, Bjerklund Johansen TE, Baust JM. Mechanisms of cryoablation: clinical consequences on malignant tumors. Cryobiology. 2014; 68:1–11.
16. Kavoussi N, Canvasser N, Caddedu J. Ablative therapies for the treatment of small renal masses: a review of different modalities and outcomes. Curr Urol Rep. 2016; 17:59.
17. Klossner DP, Robilotto AT, Clarke DM, VanBuskirk RG, Baust JM, Gage AA, et al. Cryosurgical technique: assessment of the fundamental variables using human prostate cancer model systems. Cryobiology. 2007; 55:189–199.
18. Ge BH, Guzzo TJ, Nadolski GJ, Soulen MC, Clark TW, Malkowicz SB, et al. Percutaneous renal cryoablation: short-axis ice-ball margin as a predictor of outcome. J Vasc Interv Radiol. 2016; 27:403–409.
19. Ali O, Fishman EK, Kawamoto S. Recurrent renal cell carcinoma following nephrectomy and ablation therapy: radiology perspective. Eur J Radiol. 2018; 107:134–142.
20. Thompson RH, Atwell T, Schmit G, Lohse CM, Kurup AN, Weisbrod A, et al. Comparison of partial nephrectomy and percutaneous ablation for cT1 renal masses. Eur Urol. 2015; 67:252–259.
21. Bhindi B, Mason RJ, Haddad MM, Boorjian SA, Leibovich BC, Atwell TD, et al. Outcomes after cryoablation versus partial nephrectomy for sporadic renal tumors in a solitary kidney: a propensity score analysis. Eur Urol. 2018; 73:254–259.
22. Andrews JR, Atwell T, Schmit G, Lohse CM, Kurup AN, Weisbrod A, et al. Oncologic outcomes following partial nephrectomy and percutaneous ablation for cT1 renal masses. Eur Urol. 2019; 76:244–251.
23. Lay AH, Faddegon S, Olweny EO, Morgan M, Lorber G, Trimmer C, et al. Oncologic efficacy of radio frequency ablation for small renal masses: clear cell vs papillary subtype. J Urol. 2015; 194:653–657.
24. Best SL, Park SK, Youssef RF, Olweny EO, Tan YK, Trimmer C, et al. Long-term outcomes of renal tumor radio frequency ablation stratified by tumor diameter: size matters. J Urol. 2012; 187:1183–1189.
25. Lay AH, Stewart J, Canvasser NE, Cadeddu JA, Gahan JC. Likelihood of incomplete kidney tumor ablation with radio frequency energy: degree of enhancement matters. J Urol. 2016; 196:41–45.
26. Hudspeth TN, Abdelsalam ME, Sabir SH, Kusin SB, Matin SF, Wood CG, et al. Minimally invasive image guided thermal ablation for recurrent renal cell carcinoma (RCC) after ipsilateral partial nephrectomy. J Clin Oncol. 2018; 36:e16557–e16557.
27. Rivero JR, De La Cerda J 3rd, Wang H, Liss MA, Farrell AM, Rodriguez R, et al. Partial nephrectomy versus thermal ablation for clinical stage T1 renal masses: systematic review and meta-analysis of more than 3900 patients. J Vasc Interv Radiol. 2018; 29:18–29.
28. Reyes J, Canter D, Putnam S, Simhan J, Smaldone MC, Kutikov A, et al. Thermal ablation of the small renal mass: case selection using the R.E.N.A.L.-Nephrometry Score. Urol Oncol. 2013; 31:1292–1297.
29. Kurup AN. Percutaneous ablation for small renal masses-complications. Semin Intervent Radiol. 2014; 31:42–49.
30. Mitchell CR, Atwell TD, Weisbrod AJ, Lohse CM, Boorjian SA, Leibovich BC, et al. Renal function outcomes in patients treated with partial nephrectomy versus percutaneous ablation for renal tumors in a solitary kidney. J Urol. 2011; 186:1786–1790.
31. McIntosh AG, Ristau BT, Ruth K, Jennings R, Ross E, Smaldone MC, et al. Active surveillance for localized renal masses: tumor growth, delayed intervention rates, and >5-yr clinical outcomes. Eur Urol. 2018; 74:157–164.
32. Motzer RJ, Jonasch E, Agarwal N, Bhayani S, Bro WP, Chang SS, et al. Kidney cancer, version 2.2017, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2017; 15:804–883.
33. Ljungberg B, Bensalah K, Canfield S, Dabestani S, Hofmann F, Hora M, et al. EAU guidelines on renal cell carcinoma: 2014 update. Eur Urol. 2015; 67:913–924.
 XML Download
XML Download