

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Seung-seob Kim, MD , Jin-Young Choi, MD, Hyungjin Rhee, MD
, Jin-Young Choi, MD, Hyungjin Rhee, MD
, Jin-Young Choi, MD, Hyungjin Rhee, MD
Abstract
In patients at high risk of hepatocellular carcinoma (HCC), such as those with chronic hepatitis or cirrhosis, the confirmative diagnosis of HCC can be made solely from characteristic imaging findings on contrast-enhanced CT or MR scans. However, in daily practice, HCCs showing atypical imaging features are frequently encountered. Since the criteria for diagnosis of HCC is based on dynamic contrast enhancement patterns, it is essential to thoroughly understand these patterns. In this article, we aim to use gadoxetate-enhanced MRI to comprehensively review the HCC enhancement patterns and the associated histopathologic findings with their prognostic factors.
Figures and Tables
Fig. 1
Hepatocellular carcinoma without “washout” enhancement patterns, but showing transitional hypointensity. Hepatocellular carcinoma with Edmonson-Steiner grade I–II was confirmed via surgery.
A, B. A 57-year-old male patient with non-alcoholic fatty liver disease underwent MRI using the extracellular contrast agent (gadoterate meglumine; Dotarem, Guerbet, France). The signal intensity of the focal hepatic lesion in the left lateral section is more than that of the adjacent liver parenchyma in both the portal (A, arrow) and the delayed phases (B, arrow). The lesion showed nonrim hyperenhancement in the late arterial phase (not shown).
C, D. After 21 days, the same patient underwent MRI using the hepatocyte-specific contrast agent (gadoxetate; Primovist, Bayer Healthcare, Berlin, Germany). The signal intensity of the focal hepatic lesion in the left lateral section is similar to that of the adjacent liver parenchyma in the portal phase (C, arrow). However, in the transitional phase (D, arrow), the signal intensity of the lesion is less than that of the adjacent liver parenchyma. The lesion showed nonrim hyperenhancement in the late arterial phase (not shown).

Fig. 2
Early hepatocellular carcinoma without arterial hyperenhancement, but showing hypointensity in the hepatobiliary phase. A 57-year-old male patient with liver cirrhosis underwent MRI using the hepatocyte-specific contrast agent (gadoxetate). Early hepatocellular carcinoma was confirmed via surgery.
A. The focal hepatic lesion in the right hemiliver is not clearly delineated due to the absence of arterial hyperenhancement in the late arterial phase (arrow).
B. In the portal phase, the signal intensity of the lesion is less than that of the adjacent liver parenchyma (arrow).
C. In the hepatobiliary phase, the lesion shows hypointensity (arrow).

Fig. 3
Dysplastic nodule showing hypointensity in the hepatobiliary phase. A 61-year-old male patient with hepatitis B-related cirrhosis underwent MRI using the hepatocyte-specific contrast agent (gadoxetate). The high-grade dysplastic nodule was confirmed via surgery.
A. In the precontrast T1-weighted image, the focal hepatic lesion in the right hemiliver shows hyperintensity (arrow).
B. In the arterial phase with the subtraction technique, the lesion shows no arterial hyperenhancement (arrow).
C. In the portal phase, the lesion shows isointensity with the adjacent liver parenchyma (arrow).
D. In the hepatobiliary phase, the lesion shows hypointensity (arrow).

Fig. 4
Poorly differentiated hepatocellular carcinoma without arterial hyperenhancement. A 61-year-old female patient with hepatitis B-related cirrhosis underwent MRI using the hepatocyte-specific contrast agent (gadoxetate). The poorly differentiated hepatocellular carcinoma was confirmed through surgery. The hematoxylin-eosin staining slide displayed a large area of central necrosis (not shown).
A. The focal hepatic lesion in the left lateral section shows no arterial hyperenhancement in the late arterial phase.
B. In the portal phase, the signal intensity of the lesion is less than that of the adjacent liver parenchyma. The central portion of the lesion showed no contrast enhancement throughout the entirety of the dynamic sequences (not shown).
C. In the hepatobiliary phase, the lesion shows hypointensity.

Fig. 5
Scirrhous hepatocellular carcinoma without “washout” enhancement patterns. A 47-year-old male patient with hepatitis B-related cirrhosis underwent MRI using the hepatocyte-specific contrast agent (gadoxetate). Scirrhous hepatocellular carcinoma was confirmed via surgery.
A. The focal hepatic lesion in the right hemiliver shows arterial hyperenhancement in the late arterial phase (arrow).
B, C. In the portal (B, arrow) and transitional (C, arrow) phases, contrast enhancement is persistent without “washout.”
D. In the hepatobiliary phase, the lesion shows a targetoid appearance from the contrast retention at the central area (arrow).

Fig. 6
Hepatocellular carcinoma showing irregular rim enhancement. A 61-year-old male patient with chronic B-viral hepatitis underwent MRI using the hepatocyte-specific contrast agent (gadoxetate). Hepatocellular carcinoma was confirmed via surgery. The hematoxylin-eosin staining slide displayed a large area of central necrosis (not shown).
A. The focal hepatic lesion in the right hemiliver shows irregular rim enhancement in the late arterial phase (arrow).
B. In the transitional phase, the lesion shows persistent irregular rim enhancement (arrow). The central portion of the lesion showed no contrast enhancement throughout the entirety of the dynamic sequences (not shown).
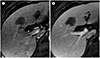
Fig. 7
Hepatocellular carcinoma with microvascular invasion. A 58-year-old male patient with chronic B-viral hepatitis underwent MRI using the hepatocyte-specific contrast agent (gadoxetate). Hepatocellular carcinoma with microvascular invasion and infiltrative tumor margin was confirmed via surgery.
A. The focal hepatic lesion is seen in the left medial section. In the late arterial phase, the lesion shows nonrim arterial hyperenhancement. Irregular enhancement is also seen in the peritumoral liver parenchyma.
B. In the hepatobiliary phase, the lesion shows hypointensity and a non-smooth margin. The peritumoral liver parenchyma also shows hypointensity.
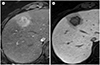
Fig. 8
Hepatocellular carcinoma showing intratumoral vessels with aneurysmal change. A 47-year-old male patient with chronic B-viral hepatitis underwent MRI using the hepatocyte-specific contrast agent (gadoxetate). A large mass is seen in the right hemiliver. Strongly enhancing vessels are seen inside the tumor in the late arterial phase, some of which accompany aneurysmal change (arrow). Poorly differentiated hepatocellular carcinoma was confirmed via surgery. The hematoxylin-eosin staining slide demonstrated a large area of central necrosis and multiple intratumoral vessels with a pseudoaneurysmal change (not shown).

Fig. 9
Hepatocellular carcinoma showing hyperintensity in the hepatobiliary phase. A 73-year-old male patient with chronic B-viral hepatitis underwent MRI using the hepatocyte-specific contrast agent (gadoxetate). The focal hepatic lesion in the left lateral section shows homogeneous hyperintensity in the hepatobiliary phase (arrow). The lesion showed arterial hyperenhancement and no “washout” or transitional hypointensity in the dynamic sequences (not shown). Moderately differentiated hepatocellular carcinoma was confirmed via surgery. Expression level of the organic anion transporting polypeptide 8 was higher in the tumor than in the adjacent liver parenchyma (not shown). The tumor did not recur for over five years after the surgery.


References
1. Xiao YD, Paudel R, Liu J, Ma C, Zhang ZS, Zhou SK. MRI contrast agents: classification and application (review). Int J Mol Med. 2016; 38:1319–1326.
2. Gandhi SN, Brown MA, Wong JG, Aguirre DA, Sirlin CB. MR contrast agents for liver imaging: what, when, how. Radiographics. 2006; 26:1621–1636.
3. Choi JY, Lee JM, Sirlin CB. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: part II. Extracellular agents, hepatobiliary agents, and ancillary imaging features. Radiology. 2014; 273:30–35.
4. Reimer P, Schneider G, Schima W. Hepatobiliary contrast agents for contrast-enhanced MRI of the liver: properties, clinical development and applications. Eur Radiol. 2004; 14:559–578.
5. Ahn SS, Kim MJ, Lim JS, Hong HS, Chung YE, Choi JY. Added value of gadoxetic acid-enhanced hepatobiliary phase MR imaging in the diagnosis of hepatocellular carcinoma. Radiology. 2010; 255:459–466.
6. Lee YJ, Lee JM, Lee JS, Lee HY, Park BH, Kim YH, et al. Hepatocellular carcinoma: diagnostic performance of multidetector CT and MR imaging-a systematic review and meta-analysis. Radiology. 2015; 275:97–109.
7. Yoon JH, Lee JM, Lee YJ, Lee KB, Han JK. Added value of sequentially performed gadoxetic acid-enhanced liver MRI for the diagnosis of small (10–19 mm) or atypical hepatic observations at contrast-enhanced CT: a prospective comparison. J Magn Reson Imaging. 2019; 49:574–587.
8. An C, Kim MJ. Imaging features related with prognosis of hepatocellular carcinoma. Abdom Radiol (NY). 2019; 44:509–551.
9. Roberts LR, Sirlin CB, Zaiem F, Almasri J, Prokop LJ, Heimbach JK, et al. Imaging for the diagnosis of hepatocellular carcinoma: a systematic review and meta-analysis. Hepatology. 2018; 67:401–421.
10. European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018; 69:182–236.
11. Tang A, Bashir MR, Corwin MT, Cruite I, Dietrich CF, Do RKG, et al. Evidence supporting LI-RADS major features for CT- and MR imaging-based diagnosis of hepatocellular carcinoma: a systematic review. Radiology. 2018; 286:29–48.
12. Kitao A, Zen Y, Matsui O, Gabata T, Kobayashi S, Koda W, et al. Hepatocellular carcinoma: signal intensity at gadoxetic acid-enhanced MR Imaging--correlation with molecular transporters and histopathologic features. Radiology. 2010; 256:817–826.
13. Kitao A, Matsui O, Yoneda N, Kozaka K, Shinmura R, Koda W, et al. The uptake transporter OATP8 expression decreases during multistep hepatocarcinogenesis: correlation with gadoxetic acid enhanced MR imaging. Eur Radiol. 2011; 21:2056–2066.
14. Choi JY, Lee JM, Sirlin CB. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: part I. Development, growth, and spread: key pathologic and imaging aspects. Radiology. 2014; 272:635–665.
15. Ringe KI, Husarik DB, Sirlin CB, Merkle EM. Gadoxetate disodium-enhanced MRI of the liver: part 1, protocol optimization and lesion appearance in the noncirrhotic liver. AJR Am J Roentgenol. 2010; 195:13–28.
16. Higaki A, Tamada T, Sone T, Kanki A, Sato T, Tanimoto D, et al. Potential clinical factors affecting hepatobiliary enhancement at Gd-EOB-DTPA-enhanced MR imaging. Magn Reson Imaging. 2012; 30:689–693.
17. Nassif A, Jia J, Keiser M, Oswald S, Modess C, Nagel S, et al. Visualization of hepatic uptake transporter function in healthy subjects by using gadoxetic acid-enhanced MR imaging. Radiology. 2012; 264:741–750.
18. Rimola J, Davenport MS, Liu PS, Brown T, Marrero JA, McKenna BJ, et al. Diagnostic accuracy of MRI with extracellular vs hepatobiliary contrast material for detection of residual hepatocellular carcinoma after locoregional treatment. Abdom Radiol (NY). 2019; 44:549–555.
19. Asayama Y, Nishie A, Ishigami K, Ushijima Y, Takayama Y, Okamoto D, et al. Histogram analysis of noncancerous liver parenchyma on gadoxetic acid-enhanced MRI: predictive value for liver function and pathology. Abdom Radiol (NY). 2016; 41:1751–1175.
20. Jin YJ, Lee SH, Cho SG, Kim JH, Lee JW, Lee KY, et al. Prediction of postoperative liver failure using gadoxetic acid-enhanced magnetic resonance imaging in patients with hepatocellular carcinoma. J Gastroenterol Hepatol. 2016; 31:1349–1356.
21. Joo I, Lee JM, Lee DH, Jeon JH, Han JK, Choi BI. Noninvasive diagnosis of hepatocellular carcinoma on gadoxetic acid-enhanced MRI: can hypointensity on the hepatobiliary phase be used as an alternative to washout? Eur Radiol. 2015; 25:2859–2868.
22. Chernyak V, Fowler KJ, Kamaya A, Kielar AZ, Elsayes KM, Bashir MR, et al. Liver Imaging Reporting and Data System (LI-RADS) version 2018: imaging of hepatocellular carcinoma in at-risk patients. Radiology. 2018; 289:816–830.
23. Kim YN, Song JS, Moon WS, Hwang HP, Kim YK. Intra-individual comparison of hepatocellular carcinoma imaging features on contrast-enhanced computed tomography, gadopentetate dimeglumine-enhanced MRI, and gadoxetic acid-enhanced MRI. Acta Radiol. 2018; 59:639–648.
24. Motosugi U, Ichikawa T, Sano K, Sou H, Onohara K, Muhi A, et al. Double-dose gadoxetic acid-enhanced magnetic resonance imaging in patients with chronic liver disease. Invest Radiol. 2011; 46:141–145.
25. Davenport MS, Bashir MR, Pietryga JA, Weber JT, Khalatbari S, Hussain HK. Dose-toxicity relationship of gadoxetate disodium and transient severe respiratory motion artifact. AJR Am J Roentgenol. 2014; 203:796–802.
26. Pietryga JA, Burke LM, Marin D, Jaffe TA, Bashir MR. Respiratory motion artifact affecting hepatic arterial phase imaging with gadoxetate disodium: examination recovery with a multiple arterial phase acquisition. Radiology. 2014; 271:426–434.
27. Kambadakone AR, Fung A, Gupta RT, Hope TA, Fowler KJ, Lyshchik A, et al. LI-RADS technical requirements for CT, MRI, and contrast-enhanced ultrasound. Abdom Radiol (NY). 2018; 43:56–74.
28. Narita M, Hatano E, Arizono S, Miyagawa-Hayashino A, Isoda H, Kitamura K, et al. Expression of OATP1B3 determines uptake of Gd-EOB-DTPA in hepatocellular carcinoma. J Gastroenterol. 2009; 44:793–798.
29. Jin YJ, Cho SG, Lee KY, Kim JM, Lee JW. Association between relative liver enhancement on gadoxetic acid enhanced magnetic resonance images and histologic grade of hepatocellular carcinoma. Medicine (Baltimore). 2017; 96:e7580.
30. Bartolozzi C, Battaglia V, Bargellini I, Bozzi E, Campani D, Pollina LE, et al. Contrast-enhanced magnetic resonance imaging of 102 nodules in cirrhosis: correlation with histological findings on explanted livers. Abdom Imaging. 2013; 38:290–296.
31. Golfieri R, Renzulli M, Lucidi V, Corcioni B, Trevisani F, Bolondi L. Contribution of the hepatobiliary phase of Gd-EOB-DTPA-enhanced MRI to dynamic MRI in the detection of hypovascular small (≤ 2 cm) HCC in cirrhosis. Eur Radiol. 2011; 21:1233–1242.
32. Suh CH, Kim KW, Pyo J, Lee J, Kim SY, Park SH. Hypervascular transformation of hypovascular hypointense nodules in the hepatobiliary phase of gadoxetic acid-enhanced MRI: a systematic review and meta-analysis. AJR Am J Roentgenol. 2017; 209:781–789.
33. Lee DH, Lee JM, Lee JY, Kim SH, Kim JH, Yoon JH, et al. Non-hypervascular hepatobiliary phase hypointense nodules on gadoxetic acid-enhanced MRI: risk of HCC recurrence after radiofrequency ablation. J Hepatol. 2015; 62:1122–1130.
34. Lee DH, Lee JM, Yu MH, Hur BY, Yi NJ, Lee KW, et al. Non-hypervascular hepatobiliary phase hypointense nodules on gadoxetic acid-enhanced MR can help determine the treatment method for HCC. Eur Radiol. 2019; 29:3122–3131.
35. Motosugi U, Ichikawa T, Sou H, Sano K, Tominaga L, Muhi A, et al. Distinguishing hypervascular pseudolesions of the liver from hypervascular hepatocellular carcinomas with gadoxetic acid-enhanced MR imaging. Radiology. 2010; 256:151–158.
36. Zech CJ, Grazioli L, Breuer J, Reiser MF, Schoenberg SO. Diagnostic performance and description of morphological features of focal nodular hyperplasia in Gd-EOB-DTPA-enhanced liver magnetic resonance imaging: results of a multicenter trial. Invest Radiol. 2008; 43:504–511.
37. Choi JY, Lee HC, Yim JH, Shim JH, Lim YS, Shin YM, et al. Focal nodular hyperplasia or focal nodular hyperplasia-like lesions of the liver: a special emphasis on diagnosis. J Gastroenterol Hepatol. 2011; 26:1004–1009.
38. Choi YS, Rhee H, Choi JY, Chung YE, Park YN, Kim KW, et al. Histological characteristics of small hepatocellular carcinomas showing atypical enhancement patterns on gadoxetic acid-enhanced MR imaging. J Magn Reson Imaging. 2013; 37:1384–1391.
39. Asayama Y, Yoshimitsu K, Irie H, Nishihara Y, Aishima S, Tajima T, et al. Poorly versus moderately differentiated hepatocellular carcinoma: vascularity assessment by computed tomographic hepatic angiography in correlation with histologically counted number of unpaired arteries. J Comput Assist Tomogr. 2007; 31:188–192.
40. Nakachi K, Tamai H, Mori Y, Shingaki N, Moribata K, Deguchi H, et al. Prediction of poorly differentiated hepatocellular carcinoma using contrast computed tomography. Cancer Imaging. 2014; 14:7.
41. Asayama Y, Yoshimitsu K, Nishihara Y, Irie H, Aishima S, Taketomi A, et al. Arterial blood supply of hepatocellular carcinoma and histologic grading: radiologic-pathologic correlation. AJR Am J Roentgenol. 2008; 190:W28–W34.
42. Tanaka S, Sugimachi K, Yamashita Yi Y, Ohga T, Shirabe K, Shimada M, et al. Tie2 vascular endothelial receptor expression and function in hepatocellular carcinoma. Hepatology. 2002; 35:861–867.
43. Jain RK. Determinants of tumor blood flow: a review. Cancer Res. 1988; 48:2641–2658.
44. Le Moigne F, Durieux M, Bancel B, Boublay N, Boussel L, Ducerf C, et al. Impact of diffusion-weighted MR imaging on the characterization of small hepatocellular carcinoma in the cirrhotic liver. Magn Reson Imaging. 2012; 30:656–665.
45. Okamoto D, Yoshimitsu K, Nishie A, Tajima T, Asayama Y, Ishigami K, et al. Enhancement pattern analysis of hypervascular hepatocellular carcinoma on dynamic MR imaging with histopathological correlation: validity of portal phase imaging for predicting tumor grade. Eur J Radiol. 2012; 81:1116–1121.
46. Min JH, Kim YK, Choi SY, Jeong WK, Lee WJ, Ha SY, et al. Differentiation between cholangiocarcinoma and hepatocellular carcinoma with target sign on diffusion-weighted imaging and hepatobiliary phase gadoxetic acid-enhanced MR imaging: classification tree analysis applying capsule and septum. Eur J Radiol. 2017; 92:1–10.
47. Kudo M, Matsui O, Izumi N, Iijima H, Kadoya M, Imai Y, et al. JSH consensus-based clinical practice guidelines for the management of hepatocellular carcinoma: 2014 update by the liver cancer study group of Japan. Liver Cancer. 2014; 3:458–468.
48. Korean Liver Cancer Association. National Cancer Center. Practice guidelines for management of hepatocellular carcinoma 2018. Seoul, Goyang: KLCA, NCC;2018.
49. Kim YY, An C, Kim S, Kim MJ. Diagnostic accuracy of prospective application of the Liver Imaging Reporting and Data System (LI-RADS) in gadoxetate-enhanced MRI. Eur Radiol. 2018; 28:2038–2046.
50. Kim YY, Kim MJ, Kim EH, Roh YH, An C. Hepatocellular carcinoma versus other hepatic malignancy in cirrhosis: performance of LI-RADS version 2018. Radiology. 2019; 291:72–80.
51. An C, Park S, Chung YE, Kim DY, Kim SS, Kim MJ, et al. Curative resection of single primary hepatic malignancy: Liver Imaging Reporting and Data System category LR-M portends a worse prognosis. AJR Am J Roentgenol. 2017; 209:576–583.
52. Choi SY, Kim SH, Park CK, Min JH, Lee JE, Choi YH, et al. Imaging features of gadoxetic acid-enhanced and diffusion-weighted MR imaging for identifying cytokeratin 19-positive hepatocellular carcinoma: a retrospective observational study. Radiology. 2018; 286:897–908.
53. Chernyak V, Tang A, Flusberg M, Papadatos D, Bijan B, Kono Y, et al. LI-RADS® ancillary features on CT and MRI. Abdom Radiol (NY). 2018; 43:82–100.
54. Kim H, Park MS, Choi JY, Park YN, Kim MJ, Kim KS, et al. Can microvessel invasion of hepatocellular carcinoma be predicted by pre-operative MRI. Eur Radiol. 2009; 19:1744–1751.
55. Nino-Murcia M, Olcott EW, Jeffrey RB Jr, Lamm RL, Beaulieu CF, Jain KA. Focal liver lesions: pattern-based classification scheme for enhancement at arterial phase CT. Radiology. 2000; 215:746–751.
56. Lee JH, Lee JM, Kim SJ, Baek JH, Yun SH, Kim KW, et al. Enhancement patterns of hepatocellular carcinomas on multiphasicmultidetector row CT: comparison with pathological differentiation. Br J Radiol. 2012; 85:e573–e583.
57. Tsunematsu S, Chuma M, Kamiyama T, Miyamoto N, Yabusaki S, Hatanaka K, et al. Intratumoral artery on contrast-enhanced computed tomography imaging: differentiating intrahepatic cholangiocarcinoma from poorly differentiated hepatocellular carcinoma. Abdom Imaging. 2015; 40:1492–1499.
58. Suh YJ, Kim MJ, Choi JY, Park YN, Park MS, Kim KW. Differentiation of hepatic hyperintense lesions seen on gadoxetic acid-enhanced hepatobiliary phase MRI. AJR Am J Roentgenol. 2011; 197:W44–W52.
59. Kitao A, Matsui O, Yoneda N, Kozaka K, Kobayashi S, Koda W, et al. Hypervascular hepatocellular carcinoma: correlation between biologic features and signal intensity on gadoxetic acid-enhanced MR images. Radiology. 2012; 265:780–789.
60. Erra P, Puglia M, Ragozzino A, Maurea S, Liuzzi R, Sabino G, et al. Appearance of hepatocellular carcinoma on gadoxetic acid-enhanced hepato-biliary phase MR imaging: a systematic review. Radiol Med. 2015; 120:1002–1011.
61. Ueno A, Masugi Y, Yamazaki K, Komuta M, Effendi K, Tanami Y, et al. OATP1B3 expression is strongly associated with Wnt/β-catenin signalling and represents the transporter of gadoxetic acid in hepatocellular carcinoma. J Hepatol. 2014; 61:1080–1087.
62. Yamashita T, Kitao A, Matsui O, Hayashi T, Nio K, Kondo M, et al. Gd-EOB-DTPA-enhanced magnetic resonance imaging and alpha-fetoprotein predict prognosis of early-stage hepatocellular carcinoma. Hepatology. 2014; 60:1674–1685.
63. Kim JW, Lee CH, Kim SB, Park BN, Park YS, Lee J, et al. Washout appearance in Gd-EOB-DTPA-enhanced MR imaging: a differentiating feature between hepatocellular carcinoma with paradoxical uptake on the hepatobiliary phase and focal nodular hyperplasia-like nodules. J Magn Reson Imaging. 2017; 45:1599–1608.
64. Guo Y, Li W, Cai W, Zhang Y, Fang Y, Hong G. Diagnostic value of gadoxetic acid-enhanced MR imaging to distinguish HCA and its subtype from FNH: a systematic review. Int J Med Sci. 2017; 14:668–674.
65. Kim R, Lee JM, Shin CI, Lee ES, Yoon JH, Joo I, et al. Differentiation of intrahepatic mass-forming cholangiocarcinoma from hepatocellular carcinoma on gadoxetic acid-enhanced liver MR imaging. Eur Radiol. 2016; 26:1808–1817.
66. Hwang J, Kim YK, Park MJ, Lee MH, Kim SH, Lee WJ, et al. Differentiating combined hepatocellular and cholangiocarcinoma from mass-forming intrahepatic cholangiocarcinoma using gadoxetic acid-enhanced MRI. J Magn Reson Imaging. 2012; 36:881–889.
67. Choi JY, Kim MJ, Park YN, Lee JM, Yoo SK, Rha SY, et al. Gadoxetate disodium-enhanced hepatobiliary phase MRI of hepatocellular carcinoma: correlation with histological characteristics. AJR Am J Roentgenol. 2011; 197:399–405.
68. Jeong HT, Kim MJ, Kim YE, Park YN, Choi GH, Choi JS. MRI features of hepatocellular carcinoma expressing progenitor cell markers. Liver Int. 2012; 32:430–440.
69. Shin SK, Kim YS, Shim YS, Choi SJ, Park SH, Jung DH, et al. Peritumoral decreased uptake area of gadoxetic acid enhanced magnetic resonance imaging and tumor recurrence after surgical resection in hepatocellular carcinoma: a STROBE-compliant article. Medicine (Baltimore). 2017; 96:e7761.
70. Ishigami K, Yoshimitsu K, Nishihara Y, Irie H, Asayama Y, Tajima T, et al. Hepatocellular carcinoma with a pseudocapsule on gadolinium-enhanced MR images: correlation with histopathologic findings. Radiology. 2009; 250:435–443.
71. An C, Rhee H, Han K, Choi JY, Park YN, Park MS, et al. Added value of smooth hypointense rim in the hepatobiliary phase of gadoxetic acid-enhanced MRI in identifying tumour capsule and diagnosing hepatocellular carcinoma. Eur Radiol. 2017; 27:2610–2618.
72. Kim B, Lee JH, Kim JK, Kim HJ, Kim YB, Lee D. The capsule appearance of hepatocellular carcinoma in gadoxetic acid-enhanced MR imaging: correlation with pathology and dynamic CT. Medicine (Baltimore). 2018; 97:e11142.
 XML Download
XML Download