

 PDF
PDF ePub
ePub Citation
Citation Print
Print


 , Suk Hee Heo, MD1, Sang Soo Shin, MD2, Yong Yeon Jeong, MD1
, Suk Hee Heo, MD1, Sang Soo Shin, MD2, Yong Yeon Jeong, MD1
Abstract
Figures and Tables
 | Fig. 1Contrast-enhanced CT images of Bosniak classification of cystic renal masses.
A. Class I simple cyst with homogeneous water attenuation density (0–20 Hounsfield unit) and no enhancement.
B. Class II cyst with few hairline thin septa (arrows).
C. Class IIF cystic mass with minimal smooth thickened septa and calcification (arrow).
D. Class III cystic mass with thickened irregular septa and nodular calcification.
E. Class IV cystic mass with mural enhancing soft tissue nodule (arrow).
|
 | Fig. 2Drawings of the Bosniak classification version 2019.
A. Class I. Well-defined cyst with thin (≤ 2 mm) smooth wall and homogeneous simple fluid (−9 to 20 HU on CT or SI similar to CSF); no septa or calcifications.
B. Class II. Cystic mass with thin (≤ 2 mm) or few (1–3) enhancing septa; may have calcifications (green color) of any type; or homogeneous mass markedly hyperintense at T2WI (similar to CSF) or markedly hyperintense at T1WI (approximately × 2.5 normal parenchymal SI) at noncontrast MRI.
C–E. Class IIF. Cystic masses with a smooth minimally thickened (3 mm) enhancing wall or smooth minimal thickening (3 mm) of one or more enhancing septa (C), or many (≥ 4) smooth thin (≤ 2 mm) enhancing septa (D) at CT or MRI; or heterogeneous hyperintensity at unenhanced fat-saturated T1WI (E).
F. Class III. Cystic masses with one or more enhancing thick (≥ 4 mm) or enhancing irregular (≤ 3 mm obtusely margined convex protrusion[s]; blue color) walls or septa.
G. Class IV. Cystic mass with one or more enhancing nodule(s) (≥ 4 mm convex protrusion with obtuse margins, or a convex protrusion of any size with acute margins; red color).
CSF = cerebrospinal fluid, HU = Hounsfield unit, SI = signal intensity, T1WI = T1-weighted image, T2WI = T2-weighted image
|
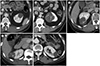
 | Fig. 3Cystic renal mass in a 44-year old man, which is initially classified Bosniak class IIF at CT and upgraded to Bosniak class III at MRI.
A. Contrast-enhanced CT image shows a 2.5 cm Bosniak IIF cystic mass with multiple minimally smooth thickened septa in the right kidney.
B, C. T2-weighted (B) and gadolinium-enhanced T1-weighted (C) MRI images show irregular thick septa (arrowheads) and some enhancing convex protrusions (arrows) within the cystic mass better than CT (A), being upgraded to Bosniak class III. The lesion was surgically resected and histopathological examination revealed multilocular cystic renal cell carcinoma.
|
 | Fig. 4Hemorrhagic cystic renal mass in a 58-year-old man.
A, B. A 2.5 cm heterogeneous hyperintense mass (asterisks) both at in-phase T1-weighted (A) and unenhanced fat-saturated T1-weighted MR image (B) is seen in the right kidney. The hyperintense component is consistent with hemorrhage.
C. Post-contrast subtraction image clearly shows the thick (≥ 4 mm) enhancing posterior wall (arrows) and thick (≥ 4 mm), irregular enhancing septum (arrowhead) of the mass, suggestive of Bosniak class III. The mass was resected and pathologically confirmed as a chromophobe renal cell carcinoma.
|
 | Fig. 5Bosniak IIF cystic mass in the left kidney in a 49-year old man.
A. Contrast-enhanced coronal CT image shows a 4 cm Bosniak IIF cystic mass in the upper pole of left kidney.
B. At 18-month follow-up, number and thickening of the septa (arrows) within the cystic mass are increased, morphologic changes concerning for RCC. The mass was resected and pathologically confirmed as multilocular cystic RCC.
RCC = renal cell carcinoma
|
 | Fig. 6Bosniak IIF cystic mass in the right kidney in a 55-year old woman.
A. A 3.5 cm cystic mass with multiple thin or minimal smooth thickened septa seen and considered to be Bosniak IIF.
B. At 15-month follow-up, CT shows interval growth of the cystic mass from 3.5 cm to 4.5 cm. The mass was resected and pathologically confirmed as a benign multilocular cyst. Growth of a cystic mass without morphologic change is not indicative of malignancy.
|
Table 1
Bosniak Classes and Management for Cystic Renal Masses

*The recommended interval for follow-up examinations is to obtain a CT scan or MRI at 6 and 12 months, followed by yearly examinations for a minimum of 5 years.
†Although Bosniak III or IV cystic masses generally require surgical intervention, the most recent American Urological Association guidelines propose active surveillance as an initial management option for Bosniak III and IV masses 2 cm or less in patients with limited life expectancy.
![]()


Acknowledgments
Notes
Author Contributions
Conceptualization, N.Y.K., H.S.H.
data curation, all authors.
formal analysis, all authors.
funding acquisition, H.S.H.
investigation, all authors.
methodology, N.Y.K., H.S.H.
project administration, H.S.H.
resources, N.Y.K., H.S.H.
supervision, H.S.H.
validation, all authors.
visualization, N.Y.K., H.S.H.
writing—original draft, N.Y.K., H.S.H.
writing—review & editing, all authors.
 XML Download
XML Download