

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Reconstruction of the distal ureter is performed for a variety of benign pathologies that include but are not limited to vesicoureteral reflux (VUR), megaureter or obstruction. Although obstruction due to stone disease is common, iatrogenic injury from radiation or various urologic [1], gynecologic (GYN) [2] and colorectal surgeries is commonly seen in developed countries. Iatrogenic injury most commonly present as symptomatic or asymptomatic obstruction and less commonly due to fistula formation. Ureteral obstruction due to stricture formation can lead to significant morbidity such as chronic pain, infection, hydronephrosis, and eventual irreversible renal injury [3] while posing a challenging disease entity for urologists due to wide spectrum of treatment modalities required. Although the initial management is often endoscopic with balloon dilation and stent placement, the long-term outcomes of these procedures are poor and not durable [4]. Definitive ureteral reconstruction has traditionally been performed using open laparotomy as the ‘gold standard’ for adequate exposure in the pelvis and retroperitoneal space [567]. Contemporary literature about laparoscopic ureteral reconstruction has suggested decreased blood loss, length of hospitalization stay and post-operative pain when compared to the open laparotomy approach [8].
The exposure needed to work in the pelvis to address distal ureteral obstructions makes the robot-assisted laparoscopic (RAL) approach an attractive option. The da Vinci Surgical System (Intuitive Surgical, Sunnyvale, CA, USA) obtained Food and Drug Administration clearance in the year 2000, and was introduced to the market with an initial 3 arm system which included a camera arm. The first RAL radical prostatectomy (RALP) was performed the same year [9]. With early adoption of RAL, urology has been in the forefront of its application for other procedures including pyeloplasty, partial nephrectomy, nephroureterectomy, radical cystectomy, adrenalectomy, and more recently ureteral reconstruction. Here, we focus on RAL reconstruction of distal ureter for benign pathologies given the limited body of literature in the field. We will discuss peri-operative and post-operative outcomes as well as some technical considerations in the current medical literature.
METHODS
We performed a literature review of the PubMed database on April 2019 with the following keywords: robotic distal ureter; distal; distales; distally; distals; ureters; ureteral; ureteric; ureteritis; robotically; robotized; robotics; robots; robot. We included publications in the English language reporting adult patients (>18 years old). We excluded studies reporting management of malignant pathology such as distal ureterectomy or nephroureterectomy. The articles included case reports, including video techniques, cases series, and comparative studies from single institution and multi-institution groups. Studies that met our inclusion criteria were reviewed by two of the co-authors (A.M.A & R.A.L).
PURE ROBOT-ASSISTED URETERAL REIMPLANT
Also referred to as ureteroneocystostomy, ureteral reimplantation is a time-tested urologic surgery, first attempted in 1876 by Nussbaum [10]. Over the next decades, the technique was advanced by experts in the field for both pediatric and adult indications such as VUR, megaureter, and distal ureteral obstruction. With the advent of laparoscopy and RAL, these techniques were adapted to be performed using a minimally invasive approach. The first reported case of RAL ureteral reimplantation was by Yohannes et al. [11] in 2003 in a 43 year old male with 2.5 cm distal ureteral stricture secondary to multiple ureteroscopies for urolithiasis. The surgery was completed in 210 minutes without any intra-operative or post-operative complications. Estimated blood loss (EBL) was noted to be <50 mL. A 6-month follow-up intravenous urogram (IVU) demonstrated a patent system without evidence of obstruction.
The following year, the first report of ureteral reimplantation secondary to iatrogenic injury during RALP was published [12]. Schimpf and Wagner [13] reported this group's experience with RAL distal ureteral reconstruction in eleven patients which included three with benign pathology. One patient underwent ureteral reimplantation alone for a Hutch diverticulum. The operation, which also included bladder diverticulectomy lasted 240 minutes with EBL of 25 mL. The patient had no complications and was discharged on post-operative day 2. After a 36-month follow-up period, no radiological evidence of obstruction was reported. With the rising utilization of robotic surgery, small cases series of rare benign pathologies, such as ureterovaginal fistulas (UVF) after hysterectomy have been published. In 2008, Laungani et al. [14] performed RAL ureteral reimplantation in 3 patients with continuous vaginal leaking and radiologic evidence of UVF. The operations, which lasted between 68 to 118 minutes in console time, yielded resolution of leakage without any complications [14].
Williams et al. [15] provided the first RAL ureteral reimplantation series solely for benign causes in 2009. Seven patients had various indications including impacted stone, iatrogenic injury during GYN surgery, and UVF. One patient had endometriosis resulting in bilateral obstruction. Of the total of eight ureteral units that were reimplanted, one had post-operative stricture recurrence requiring ureteral balloon dilation. However, after this endoscopic procedure, the patient remained recurrence free for remainder of the 17-month follow-up period. No complications were reported in this cohort. In a subsequent larger series in 2010, Hemal et al. [16] presented 13 patients requiring distal ureteral reconstruction with benign etiologies ranging from iatrogenic injury during prostatectomy to megaureter repair. Of these patients, twelve were performed with RAL ureteral reimplantation alone without the need for adjunct reconstructive techniques such as psoas hitch (PH) or Boari flap (BF). Mean operative time for this cohort was 153 minutes with EBL of 106 mL and length of stay (LOS) of 2.6 days. All patients with megaureters underwent ureteral tailoring prior to reimplantation and those with vesicovaginal fistulae had primary repair of the fistula.
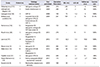
In the following years, a new case series of RAL distal ureteral reconstruction was published nearly annually. Table 1 lists operative data and outcomes of these series focusing on patients who underwent pure RAL ureteral reimplantation without PH or BF. Here, we will focus on any differentiating features such as new techniques or significant outcomes [5611131415161718192021]. Lee et al. [17] published our group's initial experience in RAL distal ureteral reconstruction in 2013. Four patients in this cohort had pure RAL reimplantation without evidence of failure at 20 months mean follow-up length. We presented both extravesical and intravesical refluxing and non-refluxing techniques. Slater et al. [18] later published the first series describing side-docking the robot in order to allow access to the genitalia, enabling cystoscopic ureteral stent placement while docked. In their cohort, 10 patients underwent RAL ureteral reimplantation for iatrogenic ureteral injury, megaureter, or VUR. Although sidedocking was done for ease of cystoscopic access, this cohort had a longer operative time compared to other series, at a mean operative time of 288 minutes. EBL was minimal (<50 mL) with no complications. Four patients in this cohort did not obtain post-operative imaging, however ultrasonography in the remaining patients showed no evidence of obstruction at mean follow-up time of 20.4 months.
Two of the most recent series focused on special cases. Abdul-Muhsin et al. [19] described distal ureteral strictures of transplanted kidneys in 3 patients with deteriorating renal function due to obstruction. Endoscopic management was initially attempted in these patients, but patency was not durable. RAL was then attempted with successful outcomes in the short follow-up period of up to 4 months. Kaouk et al. [6] presented the first series of distal ureteral reconstruction using the da Vinci SP Single Port Robotic System (Intuitive Surgical). Of the 3 patients in this cohort, one had bilateral ureteral strictures after neobladder creation following cystectomy. This patient had bilateral ureteral reimplantation without the need for an assistant port or additional incisions for the intra-abdominal drain. This was done in 180 minutes with EBL of 50 mL without any complications. Since this was a technical publication, no post-operative outcomes were provided.
ROBOT-ASSISTED URETERAL REIMPLANT WITH ADJUNCT PROCEDURES: PSOAS HITCH & BOARI FLAP
Ureteral reimplantation success is reliant on ensuring a tension-free anastomosis. In cases where this is not obtained with ureterolysis and mobilization, adjunct procedures such as a PH and/or a BF may be indicated. We will discuss both procedures in the current RAL literature. In 1896, Achille Boari, an Italian surgeon, described a tubularized flap of bladder that replaced the distal ureter in a dog [22]. However, it was not until 1939 and 1947 when Ockerblad [23] described this procedure in humans. The PH was first described in 1960 by Zimmerman et al. [24] for UVF repair by mobilizing the bladder and securing it to the psoas tendon. Using RAL, De Naeyer et al. [25] was the first to report the use of a PH for a 4 cm distal ureteral obstruction secondary to endometriosis in 2007. Operative time was 120 minutes with minimal blood loss. At 2 months follow-up, there was no evidence of obstruction or extravasation on excretory urography.
In 2008, Patil et al. [26] published the largest series of RAL ureteral reimplantation with PH for benign pathology. In this cohort of 12 patients, the most common etiology was stricture from stone disease. With a mean operating time of 208 minutes and EBL of 40 mL, this group reported 100% success based on lack of obstruction on post-operative MAG-3 renal scans or IVU. However, 2 patients were noted to have mild residual hydronephrosis with normal renal function. Multiple series mentioned in the prior section also described the use of adjunct procedures to obtain a tension-free anastomosis using PH and/or BF. Table 2 summarizes all contemporary studies reporting the use of PH and/or BF in RAL reconstruction of the distal ureter for benign pathologies [5613161718202125262728293031].
Additionally, in 2011, Yang et al. [28] published their single institution series which included one patient with endometriosis and another with ureteral transection during a GYN procedure. The authors discussed a novel technique for ureteral stent placement using a Council tip Foley catheter via the bladder and retrograde insertion into the ureter by the existing cystotomy. In 2016, Stolzenburg et al. [29] reported the largest series of RAL reimplantation with BF in 11 patients with benign ureteral strictures. The authors reported success in all patients at 15 months of follow-up. One patient was noted to have a urine leak requiring prolonged catheterization. Sagalovich et al. [27] were able to perform bilateral BFs in a patient with bilateral ureteral strictures secondary to pelvic radiation therapy. Post-operatively, the patient did not report any de novo lower urinary symptoms or need anticholinergic treatment. Finally, with the single port robotic system, Kaouk et al. [6] were the first to report use of PH in management of distal ureteral obstructions in two patients using a 3 cm incision and a multi-channel port.
ALTERNATIVE PROCEDURES
Although ureteral reimplantation with or without adjunct procedures is the most common procedure for distal ureteral reconstruction, there are few reports of alternative methods. In 2013, Lee et al. [32] published a case series from our group's experience with RAL ureteroureterostomy (UU). This cohort included 6 patients who had distal obstruction with benign etiologies such as UVF (2), iatrogenic strictures after GYN procedures (2), idiopathic stricture (1), and endometriosis (1). We reported a mean operative time of 175 minutes, EBL of 175 mL, LOS of 1 day, and no intra-operative or post-operative complications. After an average follow-up period of 11.5 months, all patients met both clinical and radiographic criteria for success. Most recently, Yang et al. [33] presented an abstract at the American Urological Association (AUA) 2019 national meeting focusing on RAL-UU for focal strictures in the distal ureter at our institution. Of the 20 patients presented with mean stricture length of 1.5 cm, 2 (10%) had recurrence during the 11.5-month follow-up period. Other groups have also reported cases of RAL-UU in their ureteral reconstruction series including Musch et al. [20] and Slater et al. [18]. Musch et al. [20] also reported a patient with endometriosis who underwent ureterolysis with omental wrapping of the ureter. This patient was free of obstruction at 30.5 months follow-up.
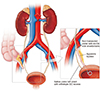
At AUA 2019, Patel et al. [34] presented a multi-institutional experience, including this article's authors, demonstrating side-to-side transection-free ureteral reimplantation. This technique, which aimed to minimize ureteral dissection and vascular compromise, entailed a ureterotomy proximal to the level of the obstruction and an anastomosis to the bladder at this level. In this series of 15 patients with 16 ureteral side-to-side reimplantations, all 16 units had radiographic evidence of success. One patient reported persistent pain from urinary reflux via the side-to-side anastomosis; thus, a transected, non-refluxing RAL ureteral reimplantation was performed thereafter. Most recently, we presented a patient with an 8 cm radiation-induced distal ureteral stricture with decreased bladder compliance and capacity [35]. In such patient who was not deemed to be a good candidate for reimplantation, the patient's appendix was used to bypass the stricture and divert urine into the bladder. Proximally, this involved an end-to-side anastomosis, which required a non-transecting longitudinal incision on healthy ureter above the level of the stricture and anastomosing the appendiceal end to the side of healthy ureter. Distally, the appendix was anastomosed to the bladder (Fig. 1) [35]. We reported an operative time of 337 minutes, EBL of 75 mL, and no intra-operative or post-operative complications. The patient had radiographic success at 3 months follow-up.
Finally, in management of complex ureteral strictures, buccal mucosal graft (BMG) has been utilized [363738], similar to its use in urethroplasty [39]. As a member of Collaborative of Reconstructive Robotic Ureteral Surgery (CORRUS), we have previously described our experience and techniques with promising outcomes [4041]. While majority of RAL-BMG ureteroplasties were performed for mid or proximal strictures, we have employed this technique in select cases of distal ureteral strictures. This was done in two young females who desired future pregnancy. Given the suggested increased risk of fetal loss, urinary tract infection due to the development of VUR, and ureteral obstruction in pregnant patients with a history of ureteral reimplantation [42], we opted to minimize alteration to pelvic anatomy and ureteral drainage. RAL ventral onlay BMG ureteroplasty allowed us to maintain the natural course of the ureter and native ureteral orifice. At median follow-up length of 13 months, both patients were symptom-free with brisk drainage on MAG-3 renal scans.
COMPARING OPEN VS. LAPAROSCOPY VS. ROBOT-ASSISTED LAPAROSCOPY
With the relative immaturity in robotic ureteral reconstruction literature, limited number of studies exist that directly compare RAL to open or pure laparoscopy. Although not a direct comparison, Patil et al. [26] was the first to compare their series with earlier publications of open vs. laparoscopic ureteral reimplantation. By outlining the findings from an open vs. laparoscopic series [43] with their RAL series, they described the difference in open, laparoscopic, and RAL operative time (187 vs. 228 vs. 208 minutes), EBL (610 vs. 370 vs. 48 mL), LOS (19.1 vs. 9.2 vs. 4.3 days), with clinical and radiographic success rate of 80% vs. 100% vs. 100% after a follow-up length of 65, 17, and 15.5 months, respectively.
Kozinn et al. [44] compared 10 open and 10 RAL distal ureteral reconstructions using ureteral reimplantation with or without PH and BF in benign distal ureteral stricture disease. In the open cohort, 6 patients underwent pure ureteral reimplantation, 3 needed a concurrent PH, and 1 patient underwent a BF. These were performed by multiple surgeons. The RAL arm had 4 pure reimplantations, 4 with PH, and 2 with BF performed by a single surgeon. No patient was converted to open in this arm. Notably, a reported exclusion criteria for the robotic approach was history of pelvic radiation or lower extremity bypass graft. The authors found statistically significant lower EBL (30.6 vs. 327.5 mL, p=0.001) and LOS (2.4 vs. 5.1 days, p=0.01) in RAL compared to open, respectively. The RAL arm reported decreased narcotics use for post-operative pain compared to open but this was not statistically significant (69 vs. 174.1 mg morphine respectively, p=0.22). Lastly, the authors noted no significant difference in operative time between open and RAL (306 vs. 270 minutes, p=0.316). Using clinical and radiographic studies such as MAG-3 renal scan, no patient had evidence of recurrence in either arm during the median follow-up length of 30 months (open) and 24 months (RAL).
Comparing 6 patients with pure laparoscopic vs. 13 patients with RAL ureteral reimplantation, Baldie et al. [45] reported their management of benign distal ureteral pathologies. The laparoscopic vs. RAL arms were similar in their mean operative time (266.7 vs. 276.5 minutes), EBL (150 vs. 182 mL), LOS (2.7 vs. 2.8 days). Two patients in the RAL arm and 1 in the laparoscopic group converted to open. Only one complication was reported, which was an unrecognized enterotomy in the RAL arm requiring surgical repair. Of note, one patient in the RAL arm had a mid-ureteral stricture treated with reimplantation. Additionally, patients who underwent RAL had a higher incidence of prior abdominal surgeries and prior open ureteral reconstruction attempts. Although no statistical analysis was done, their descriptive comparison helps differentiate the two minimally invasive approaches. Both techniques reported a 100% clinical and radiographic success rate during the 13.2 months (laparoscopy) and 4.4 months (RAL) follow-up period.
In the largest comparative study of RAL vs. open distal ureteral reimplantation for benign pathologies, Isac et al. [46] reported 25 cases of RAL cases vs. 41 open cases. Both arms had patients who required PH (4 in RAL, 14 in open) and BF (10 in RAL, 8 in open). They reported that patients who underwent RAL had longer operative times compared to the open approach (279 vs. 200 minutes respectively, p=0.0008), but significantly lower EBL (100 vs. 150 mL respectively, p=0.0008), LOS (3 vs. 5 days respectively, p=0.0004), and postoperative narcotic use (104.6 vs. 290 mg morphine respectively, p=0.0001). In the RAL arm, 2 patients had stricture recurrence and required open reconstructions with kidney autotransplantation and ileal interposition respectively. The open arm also included 2 stricture recurrences, which required a repeat open reimplantation and nephrectomy, respectively. Additionally, one patient, in the open, arm developed an enterocutaneous fistula that required surgical repair.
A comprehensive comparison of all three modalities was done by Elsamra et al. [47] who reported on 20 RAL, 85 laparoscopic, and 25 open ureteral reimplantation, some with adjunct procedures, between 2008–2013. Of note, this study included a variety of pathologies including 29 patients with malignancy, however since it was the only publication comparing all three modalities, it was included in this article. For RAL, laparoscopic, and open reconstruction, they reported no significant difference in operative time (236 vs. 235 vs. 257 minutes respectively, p=0.123) but significantly lower EBL in the RAL arm (100 vs. 150 vs. 300 mL respectively, p=0.001), and LOS (2 vs. 3 vs. 5 days respectively, p=0.01). There was no significant difference in failure rate among all arms. These studies shed light on emergence of minimal invasive approach for ureteral reconstruction by highlighting advantages of robotic ureteral reimplant with or without adjunct procedure and its feasibility in distal ureteral reconstruction.
TECHNICAL CONSIDERATIONS
Advancements in technology have provided improved visualization and dexterity during robotic surgery. However, ureteral reconstruction is unpredictable given the varying patient anatomy and the risk of devascularization during dissection. Because of this, patients should be counseled and consented for all possible repair options. In order to utilize all capabilities of the robotic platform, patient positioning and port placement are crucial and dependent on the accurate localization of the stricture with meticulous pre-operative planning.
Using the da Vinci Si surgical system, patients with distal ureteral pathology are placed in dorsal lithotomy and Trendelenburg position. A 12 mm camera port is first placed just cranial to the umbilicus followed by 8 mm right and left instrument ports placed 8 cm at both sides lateral to the umbilicus. An assistant port, 5 mm, is placed between the right arm instrument port and the camera port, but superior to the level of the umbilicus. A left-sided far lateral 8 mm instrument port for the 4th arm and a right-sided far lateral 12 mm assistant port are optional based on complexity of reconstruction and surgeon's expertise (Fig. 2) [32]. The majority of procedures were performed with the robot docked between the patient's legs after patient is placed in dorsal lithotomy. As previously mentioned, others have performed distal ureteral reconstructions with the robot docked at the patient's side to allow for easier genitalia access for manipulation of a Foley catheter and placement of ureteral stent (Fig. 3) [18]. Using the da Vinci Xi surgical system allows patient to remain supine Trendelenburg, without the use of stirrups and use of an 8 mm camera port.
Ureterolysis begins with mobilization of the colon and retroperitoneal exposure, allowing identification of healthy ureteral tissue. The ureter is dissected anteriorly with careful preservation of the posterolateral blood supply from the iliac vasculature and is continued towards the diseased segment distally. Chronic inflammation and/or disease processes distort tissue planes and may lead to fibrosis, thus increasing the difficulty of visualization and ureterolysis. Surgeons should use caution with ureteral manipulation and electrocautery to prevent devascularization.
Indocyanine green (ICG) is a chemical indicator dye visualized under near infrared fluorescence (NIF) that had reported use for cardiac, vascular, ophthalmic, and hepatic functional studies. Upon intravenous administration, ICG binds plasma proteins localizing the dye to the intravascular space. Although the compound is almost exclusively excreted by the liver and has poor renal uptake, the dye provides real-time perfusion imaging and identification under NIF [48]. Since NIF capabilities have become available on the da Vinci surgical system, our group have described its potential uses in several publications [49505152]. We now use ICG routinely in robotic reconstructive cases to assess for relevant ureteral blood supply when injected intravenously or in some cases, direct intraluminal injection to assist in difficult ureteral localization [49]. However, intraureteral and intravenous injection cannot be done simultaneously as one would obscure the other.
Once dissection is complete, the stricture length and location relative to the bladder is assessed to determine type of repair. Ureteral reimplantation can bridge gaps of 3 to 4 cm, or up to 15 cm when using adjunct procedures such as PF or BF [53]. However, UU has emerged as a viable option for short strictures noted to be at least >2 cm from the bladder [3233]. The diseased ureteral segment is then resected, and the residual gap is measured.
The final step of distal ureteral reconstruction is ureterovesical anastomosis and deployment of ureteral stent which is done using various techniques. Although guidewire and stent placement can be introduced from a laparoscopic port, we have found that the easiest and most reliable method to deliver a stent for ureteroneocystostomy is to deliver a guidewire via Foley catheter and place the stent up the ureter in a retrograde fashion [28]. Side-docking of the robot, was later described which allowed for placement of a guidewire and ureteral stent via cystoscopy with easy access to the genitalia (Fig. 3) [18].
CONCLUSIONS
Robot-assisted laparoscopy has improved urologic pelvic surgery with excellent visualization, improved dexterity, and appropriate learning curve. Patients have also benefited from this minimal invasive approach with decreased blood loss, hospital stay, and post-operative pain. In appropriately selected patients, robot-assisted laparoscopic reconstruction of the distal ureter has shown to be effective and feasible in a contemporary urology practice.



 XML Download
XML Download