

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Stress urinary incontinence (SUI) and pelvic organ prolapse (POP) are common pelvic floor disorders affecting women of all ages. Approximately 11% of women will seek surgical correction of their incontinence and/or prolapse in their lifetime [1]. Polypropylene mesh mid-urethral slings (MUS) were approved by the U. S. Food and Drug Administration (FDA) in 1998. These thin strips of mesh revolutionized treatment of SUI for women by providing a minimally invasive, durable, effective surgical treatment for SUI [23].
In the mid-2000s, polypropylene mesh began to be used for vaginal POP surgery, to augment transvaginal repairs in a manner similar to inguinal herniorrhaphy. Sheets of mesh have also been utilized abdominally for sacrocolpopexy for POP since well before MUS surgery developed wide acceptance. However, complication rates of POP repairs with transvaginal mesh (TVM) were higher than expected, prompting the FDA to issue a public health notification in 2008 and an update in 2011 [45]. The FDA emphasized the need for a more rigorous informed consent process to educate and inform patients of the full range of potential and serious complications associated with the surgical use of polypropylene mesh in this setting, including erosion, pain, infection, bleeding, organ perforation, dyspareunia and urinary issues [456]. Complications after MUS have also been identified and include vaginal mesh exposure, mesh erosion into the bladder or urethra, pelvic pain, groin pain, and dyspareunia [78]. Mesh complications after sacrocolpopexy have also been reported, including mesh erosion into the bladder, bowel, or vagina, dyspareunia, and pelvic pain [9101112].
There is limited literature on preoperative factors which may predispose patients to mesh complications specifically, as opposed to complications from surgery in general [7]. Similarly, there are limited data regarding the outcomes of women undergoing mesh explant due to mesh complications [13]. Here, we present data from our tertiary referral center experience of pelvic floor mesh explant surgery for symptomatic mesh complications. The primary goal of this study was to characterize the clinical and demographic features of patients in our clinical population with symptomatic mesh complications and secondarily, to describe outcomes after mesh removal in this population.
MATERIALS AND METHODS
This is an institutional review board (IRB)-approved, retrospective case series of consecutive female patients undergoing partial or complete removal of synthetic mesh graft for POP and/or SUI for the treatment of symptomatic, mesh-related complications, performed at a single-site tertiary referral center by 3 fellowship-trained female pelvic medicine and reconstructive surgery (FPMRS) urologists (Benaroya Research Institute at Virginia Mason IRB, approval number: 3011200). Informed consent was waived for this study. Mesh explant surgeries were performed between January 2011 and December 2016 and were identified by Current Procedural Terminology (CPT) codes 57287 (removal or revision of sling for stress incontinence), 57295 (removal or revision of vaginal mesh, vaginal approach) and 57296 (removal or revision of prosthetic vaginal graft, abdominal approach). The decision for partial versus complete mesh graft removal was discretional based on both surgical and patient considerations, and detailed pre-operative counseling between the surgeon and patient. Patients with mesh complications who were asymptomatic and managed conservatively without surgical excision were not included in the study.
Index surgeries included MUS for anti-incontinence, TVM and/or sacrocolpopexy for POP repair, and included any combination of these surgeries. MUS type was further defined as retropubic, transobturator, single-incision, or bone anchored. Index surgeries were not required to be performed at the study institution. Original operative notes were obtained whenever possible. Patient demographics, comorbidities, presenting symptoms, exam findings, mesh characteristics, and surgical factors were obtained via chart review of the electronic medical record, and primary care and specialty clinic records were reviewed when possible to confirm diagnoses. Comorbidities were defined as conditions determined to be present prior to placement of mesh. Psychiatric comorbidities included depression, anxiety and/or bipolar disorder. Chronic pain conditions preexisting prior to mesh placement were recorded, including chronic neck and/or back pain, migraines, chronic pelvic pain, fibromyalgia, and endometriosis. Chronic obstructive pulmonary disease, diabetes, and rheumatologic/autoimmune diseases were identified. When available, pre-operative visual analogue scale (VAS) for pain (0–10) was collected prior to explant surgery. The International Urogynecological Association (IUGA) Complication grades were determined pre-operatively from review of the medical record for all patients reporting pain related to their mesh [14].
Patient-reported outcome measures including the Patient Global Impression of Improvement (PGI-I) and Likert satisfaction scale (0–10), were collected postoperatively via questionnaires mailed 6 and 12 months after surgery and annually thereafter. When more than 1 questionnaire was returned, the first questionnaire returned was included in the analysis. Measures were summarized using means and frequencies, and 95% confidence intervals (CIs) where appropriate. Descriptive statistics were performed using R version 3.5.1 (https://www.R-project.org).
RESULTS
A total of 156 women underwent surgical removal of mesh graft for treatment of symptomatic complications during the 5 year study period. All initial mesh implants were placed between 1990 and 2015. Table 1 summarizes the preoperative comorbidities of this cohort at time of the initial surgery. Psychiatric diagnoses were prevalent 85 (54.5%) patients, depression and anxiety co-occurred in 21 (13.5%), depression alone was recorded in 42 (26.9%), and anxiety alone in 17 (10.9%). Bipolar disorder was observed in 3 patients. Chronic pain conditions were observed in 53 (34.0%) patients, though no patient had chronic pelvic pain prior to the mesh implant surgery. Autoimmune and rheumatologic disorders were seen in 23 (14.7%) patients and included diagnoses of rheumatoid arthritis, systemic lupus erythematosus, psoriasis, Sjogren's syndrome, Raynaud's disease and/or thyroiditis.
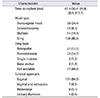
Demographic characteristics and patients' presenting symptoms at the time of mesh removal are shown in Table 2. The primary indication for removal of mesh was pain, reported in 127 women (81.4%) and 92 (59.0%) women with pain described 2 or more sites/sources of pain. The severity of pain measured by the IUGA/International Continence Society (ICS) Grades of Pain Subclassification Scale ranged from “provoked pain only (during vaginal exam)” to “spontaneous pain”, Fig. 1. A total of 78 (50.0%) women presented with a vaginal mesh exposure and 31 (19.9%) presented with mesh erosion into the bladder, urethra, and/or bowel. Three women presented with concomitant visceral erosion and vaginal exposure. There were 2 cases of erosion of mesh into both the bladder and urethra and 1 case of mesh erosion into bowel. Pain co-occurred with a mesh exposure or erosion 64.7% of the time (101/156). Thirty-five percent (54/156) of women presented with pain localized to their mesh implant and no evidence of exposed mesh in the vagina and no erosion within the bladder or urethra. De novo urinary tract infections (defined as 2 or more annual infections beginning after placement of mesh) occurred as a presenting symptom for 44 (28.2%) of women.
Patient mesh implant characteristics and the surgical approaches utilized for removal are presented in Table 3. Median time from index surgery to mesh explant was 63.5 months (interquartile range [IQR], 30.4–89.8 months). One patient ultimately required urinary diversion for obliteration of the bladder outlet and persistent ureterovaginal fistula, having failed prior conservative surgical management of her MUS complication.
Median preoperative VAS pain score was available for 123 patients (78.8%) and was 5/10 (IQR, 0–7). Forty-two percent of patients returned at least 1 post-surgery questionnaire, with a mean follow-up of 14 months. For these patients, the mean Likert satisfaction score after mesh removal was 7.4/10±3.0. Responses to the PGI-I showed that 68% of these patients reported feeling a little better, better, or very much better after surgery (mean, 2.9±1.68).
DISCUSSION
Developing a deeper understanding of why mesh complications occur in some women but not in others is a critical issue for female pelvic medicine. Risk factors associated with complications are challenging to study, in part because the development of mesh complications in women is multifactorial. The heterogeneity of patient characteristics and surgical factors, limited sample sizes, as well as the lack of a matched control group of women without mesh complications are challenges that occur with research in this area. Additionally, assessment of risk factors for mesh implant complications can be challenging due to the relatively low frequency of mesh complications and the variable length of time to presentation of these issues. In this study, we identified several demographic and clinical characteristics and comorbidities in a tertiary patient population undergoing mesh explant surgery for symptomatic mesh complications. These included psychiatric comorbidities, chronic pain, rheumatologic or autoimmune disease, diabetes, irritable bowel syndrome, tobacco use, and having a prior revision.
Previous research has suggested possible risk factors for mesh complications, including hypertension, diabetes, fibromyalgia, tobacco use, and concomitant hysterectomy [151617]. One study investigating common comorbidities among urogynecologic patients showed a high prevalence of obesity, hypertension, coronary artery disease, and diabetes mellitus, conditions which may increase overall risk of adverse surgical outcomes [18]. Similar to our findings, Danford et al. [16] identified tobacco use as frequently present in patients who undergo surgical excision for mesh complications. Another study showed that tobacco use was associated with a three-fold increase in the risk of developing a vaginal erosion after TVM repair of POP [19].
The American Urological Association (AUA) 2017 guidelines on the surgical management of SUI address some of the potential risk factors associated with mesh sling surgery, specifically in Guidelines 19 and 22 which discuss special populations and circumstances [20]. Guideline 19 indicates that chronic states such as systemic autoimmune disorders may lead to impaired wound healing and thereby increase the risk for mesh complications. Guideline 22 notes that diabetic, obese, and/or geriatric patients should be counseled regarding a higher risk of mesh erosion and potential for reduced clinical effectiveness, compared with patients without these conditions. Our results support the importance of these recommendations, as our cohort included 40 patients (25.6%) with rheumatologic and autoimmune disorders and/or diabetes. Our results also raise questions about whether women with immunosuppressive and chronic inflammatory disorders may be at greater risk for complications from mesh implants.
Chronic neck or back pain and migraines predating their mesh surgery were present in 34% of our cohort. Evidence that chronic pain disorders may contribute to mesh-related complications in POP surgery is increasing, although differences in definitions of chronic pain make direct comparisons between studies challenging [2122]. Another observation was that 53% of the patients in this study had a history of psychiatric disorders prior to their initial surgery, including depression, anxiety, and/or bipolar disorder. Previous literature has thoroughly examined the complex relationship between depression and pain [2324]. Other evidence supports an association between psychiatric disorders, such as depression and anxiety, and post-operative complications [252627]. Currently, the association of mental health conditions with symptomatology related to pelvic floor surgeries is not well understood. Depression has been associated with pelvic floor disorders in women, however as Larouche et al. [28] note, study methodologies and prevalence reported vary considerably. A recent report identified an increased risk of depression for women younger than 46 years after receiving a mesh surgical revision compared with women not requiring a revision, although women with a previous history of depression were excluded from these analyses [29]. To the best of our knowledge, our observation of increased prevalence of anxiety, depression, and/or bipolar disorder prior to index surgery in women who undergo mesh explant for symptomatic relief has not been previously reported. A deeper understanding of the interplay of mental health conditions such as anxiety, depression, and bipolar disorder with pain in pelvic floor disorders is needed.
A secondary goal of our study was to describe patient-reported outcomes associated with mesh removal in symptomatic patients. Most women undergoing mesh removal in this cohort presented with pain. However, it is important to note that 35% of women in this cohort experienced pain in the absence of mesh exposure or erosion. This may be explained by the histopathologic findings and inflammatory response that have been observed with the use of transvaginal polypropylene mesh, which may invoke pain without clinical evidence of obstruction or erosion [303132]. Prior studies have shown that 60% to 80% of women have relief of pain after mesh removal (TVM and/or sling mesh) [1522], and our results are consistent with these reports. Rogo-Gupta et al. [33] examined a cohort of 179 of 306 women who underwent removal of TVM and completed a follow-up questionnaire. Of 81 women providing PGI-I scores, 64 patients (78%) reported that their symptoms were improved overall reiterating the role for surgical excision in properly identified and counseled patients.
This retrospective study has several limitations. The patient cohort represents a single-institution and practice patterns may vary across different institutions and regions of the U.S and internationally. Surgeries were performed by 3 fellowship-trained FPMRS urologic surgeons located at a tertiary referral center. This referral pattern may impact the characteristics and/or complexity of patients who presented. Original operative notes for index mesh implant surgeries were obtained whenever possible, but were not always available. Pre-operative VAS pain scores were obtained as available, and post-operative VAS pain scores were not collected. The post-operative outcome data was patient-reported, and subjective in nature. Additionally, the patient population was heterogeneous and all types of mesh excision surgeries were included in this series (i.e., sling, TVM, and abdominal/robotic sacrocolpopexy). We acknowledge that correlations or associations cannot be established from this descriptive, clinically-based case series, but these observations may provide data for further hypothesis-driven investigation.
This study examines complications related to the use of polypropylene mesh in female pelvic floor surgery which is a timely and critically important issue. Information on mesh-related complications is important to further our understanding, to potentially identify risk factors, and to prevent future complications that are specific to the use of mesh in pelvic floor reconstruction. This study has several strengths, including the large, consecutive series of patients at a tertiary referral center. Post-operative outcomes described in this study are consistent with prior series examining surgically managed mesh complications. Further, this study examines the impact and site(s) of patients' pain with the IUGA/ICS Grades of Pain Subclassification Scale. Finally, this study provides real-world clinical data reflecting patient and surgical characteristics, including pre-operative patient-specific comorbidities and presenting symptoms together with follow-up data following mesh removal.
CONCLUSIONS
The use of polypropylene mesh for SUI and/or POP is associated with potential complications ranging in severity from minor to devastating. This research identified tobacco use, and psychiatric, immunosuppressive, and chronic pain conditions as prevalent in this cohort of patients undergoing mesh removal. Surgical removal can improve presenting symptoms, including for patients with pain in the absence of other indications, underlining the importance of counseling patients with symptomatic complications about this option.



 XML Download
XML Download