

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Alzheimer's disease (AD) is a neurodegenerative disorder that is associated with accumulations of amyloid and tau deposits in the brain.1 Autopsy studies found that while AD pathology was present in 65% of subjects at autopsy, only 43% of them had received clinical diagnoses of AD during their lifetimes.23 Other longitudinal studies have also found that substantial proportions of patients with positive amyloid scans show no cognitive decline during follow-up.4 These findings suggest that biomarkers additional to the amyloid β (Aβ) burden are needed to identify individuals who may experience cognitive decline.
Cerebral microbleeds (CMBs) are small, round, hypointense lesions that are detected using gradient-echo (GRE) T2*-weighted or susceptibility-weighted imaging (SWI) in magnetic resonance imaging (MRI) sequences, and are characterized histologically by the presence of hemosiderin deposits around small blood vessels.5 CMBs are classified into two types of vascular pathological change according to their location: 1) deep and infratentorial CMBs are possibly caused by hypertensive vasculopathy, while 2) lobar CMBs are possibly caused by cerebral amyloid angiopathy (CAA), which is characterized by the deposition of Aβ peptides in the media and adventitia of small leptomeningeal and cortical vessels.56 The vast majority of CMBs in AD show lobar predominance, representative of possible CAA pathology.7 Recent pathological studies have demonstrated that CAA is associated with cognitive impairment, even after adjusting for other age-related pathologies including vascular and AD pathology.89 These findings suggest that CMBs in AD contribute to the clinical onset and progression of the disease independently and/or simultaneously with Aβ and tau pathologies.
The developments in brain MRI have made it possible to easily detect CMBs in patients with AD. The prevalence of CMBs in subjects with AD has varied widely across studies, from 16% to 32%,10 possibly due to the inclusion of different populations. Most previous research on CMBs in AD has involved patients who were diagnosed based solely on clinical criteria, rather than using methods that can confirm amyloid pathology such as amyloid PET (positron-emission tomography) or cerebrospinal fluid (CSF) investigations. Clinical diagnoses of AD are often inaccurate and often show mismatches with biomarker-based diagnoses of AD.11
In this context, we evaluated the presence of CMBs in patients who were confirmed to have amyloid pathology using standardized 18F-florbetaben PET. We then analyzed how the clinical parameters and neuropsychological profiles varied according to the patterns of coexistence of CMBs and amyloid pathology. Finally, we evaluated the relationship between the presence and topographical location of CMBs and amyloid pathology.
METHODS
Participants
We retrospectively enrolled subjects who visited the Department of Neurology at Seoul St. Mary's Hospital with memory complaints and underwent 18F-florbetaben PET and MRI from October 2015 to May 2018. All of the participants received a medical history interview, physical and neurological examinations, screening laboratory tests including of vitamin B12, folate levels, and syphilis serology, and thyroid function tests. Information about the apolipoprotein E (APOE) genotype was available for 173 patients.
Clinical parameters such as age, sex, and vascular risk factors (hypertension, diabetes, hyperlipidemia, cardiovascular disease, and previous stroke history) were obtained by reviewing the medical records. Participants were excluded if they underwent MRI scans without SWI or showed large territorial infarcts on MRI, had a history of diseases other than mild cognitive impairment (MCI) or AD that may cause cognitive disorders, or had major psychiatric disease.
We used Petersen's criteria to diagnose MCI as follows: patients with objective memory impairment of less than 1.5 SDs from the norm in at least one memory test, but ability to perform the normal activities of daily living.12 Patients with probable AD were those who fulfilled the criteria proposed by the NINCDS-ADRDA (National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association).13 Subjective cognitive impairment (SCD) was diagnosed when patients reported complaints of memory decline but no objective cognitive decline greater than 1.5 SDs above the norm in any domain of neuropsychological tests.14 Diagnoses of possible or probable CAA were made according to the modified Boston criteria based on the presence of cortical superficial siderosis and/or lobar CMBs.15
The present study protocol was reviewed and approved by the Institutional Review Board of Seoul St. Mary's Hospital, The Catholic University of Korea (approval no: KC19RESI0799). The board exempted informed consent due to retrospective study.
Assessment of cognitive function
All of the participants underwent neuropsychological assessments using the Korean version of the Mini Mental State Examination (K-MMSE) and the Seoul Neuropsychological Screening Battery (SNSB). The SNSB consists of a digit-span task (forward and backward), the Korean version of the Boston Naming Test (K-BNT), the Rey-Osterrieth Complex Figure Test (comprising copying, immediate and 20-min-delayed recall, and recognition), the Seoul Verbal Learning Test (with 3 learning-free recall trials involving 12 words, a 20-min-delayed recall trial of these 12 items, and a recognition test), the phonemic Controlled Oral Word Association Test (COWAT), and the Stroop test (word and color reading of 112 items over a 2-min period). Functional performance was assessed using the Clinical Dementia Rating Sum of Boxes. Scores on the Geriatric Depression Scale were also obtained.
Acquisition of PET and MRI images
All PET images were acquired using combined PET/computed tomography (CT) in-line systems (Biograph TruePoint; Siemens Medical Solutions, Erlangen, Germany or Discovery 710D; GE Healthcare, Chicago, IL, USA). An average of 296 MBq 18F-florbetaben was injected intravenously, and the scan was initiated 90 minutes later. A low-dose CT scan was performed for attenuation correction and was immediately followed by PET in three-dimensional mode for 20 minutes. The subject's head was fixed using a head holder in order to minimize motion artifacts. The standard ordered subset expectation maximization algorithm (21 subsets with 3 iterations or 16 subsets with 4 iterations) was utilized for the reconstruction of PET images. All PET images were reviewed by nuclear medicine physicians who were blinded to the results of neuropsychological testing and successfully completed the electronic training program provided by the manufacturer. The result was dichotomized into amyloid positivity or negativity using visual assessments. The participants also underwent scanning on a 3.0-Tesla MRI device (Signa Excite 11.0, GE Medical Systems, Milwaukee, WI, USA) consisting of SWI and/or GRE T2-weighted imaging, as well as conventional T1-weighted, T2-weighted, and fluid-attenuated inversion recovery (FLAIR) sequences.
Image analysis
CMBs were defined as hypointense lesions within the brain parenchyma that were smaller than 10 mm in SWI images. CMBs mimic other features such as calcifications, cerebral venules, and blood vessels. Cavernous malformations were not counted as CMBs. The locations of microbleeds were subdivided into the following three categories: deep, if located in the basal ganglia, thalami, brain stem, or cerebellum; lobar, if located in one of the four cerebral lobes (frontal, parietal, occipital, or temporal); and mixed, for microbleeds distributed in both lobar and nonlobar locations.16 White-matter hyperintensities (WMHs) were rated visually on axial FLAIR images using the Fazekas scale.17 Periventricular hyperintensities were graded as 0 (no lesions), 1 (caps or a thin line), 2 (smooth halo), or 3 (extension into the white matter). Deep WMHs were graded as 0 (no lesions), 1 (punctate foci), 2 (beginning confluence of foci), or 3 (large confluent areas). Lacunar infarcts were defined as lesions <15 mm in diameter with low and high signals on T1- and T2-weighted images, respectively, and a perilesional halo on FLAIR images,18 and the number of lacunar infarcts was counted. The interrater agreement was excellent for all markers, with weighted kappa and intraclass correlation coefficient values of >0.90.
Statistical analysis
To compare the baseline demographic characteristics and neuropsychological variables according to the existence of CMB markers and amyloid positivity, we first used Kolmogorov-Smirnov tests to determine the pattern distribution of the data. Data that conformed to a normal distribution were analyzed using t-tests and chi-square tests, while the Mann-Whitney and Fisher's exact tests were used for continuous and categorical variables, respectively, that were not normally distributed.
We used multivariate logistic regression models to determine the value of CMBs for predicting amyloid pathology in patients with cognitive decline. Univariate regression models were used to determine how the amyloid status was affected by age, sex, education level, APOE ε4 genotype (carrier or noncarrier), history of hypertension, K-MMSE scores, and presence of lobar CMBs and deep CMBs. We used a multivariate logistic regression model to determine the relation between the presence of lobar CMBs and amyloid positivity (Model 1). We then classified lobar CMBs according to the topographical distribution, then reanalyzed their associations with amyloid positivity (Model 2). These regression models were adjusted for age and APOE ε4 genotype.
All statistical analyses were performed using SPSS (version 18, SPSS Inc., Chicago, IL, USA), and p values below 0.05 were considered statistically significant.
RESULTS
Amyloid PET scanning and brain MRI with SWI were applied to 227 patients. Fifteen patients were excluded because they were diagnosed with other degenerative diseases such as Parkinson's disease, Huntington disease, amyotrophic lateral sclerosis, or a brain tumor, while another 12 patients were excluded due to insufficiency of their neuropsychological test results. These exclusions resulted in 200 patients (124 females, 62%) being finally included in this study, comprising 108 patients with MCI, 83 patients with probable AD, and 9 patients with SCD.
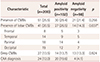
Among these 200 patients, 102 (51%) had positive amyloid PET scans and 51 (25.5%) had CMBs. The prevalence of CMBs did not differ with amyloid positivity [n=30 (29.4%) vs. n=21 (21.4%), p=0.256], but the distribution of CMBs did. CMBs in patients with positive amyloid scans were predominantly located in lobar areas [strictly lobar in 16 (53.3%) and strictly deep in 3 (1.0%) of the 30 patients], whereas CMBs in patients with negative amyloid scans were located evenly in lobar and deep areas [strictly lobar in 8 (38.0%) and strictly deep in 7 (33%) of the 21 patients]. Twenty (67%) of the 30 patients with CMBs and positive amyloid scans were eligible for a CAA diagnosis (Table 1).
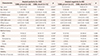
The demographic characteristics according to the presence of CMBs and amyloid positivity are presented in Table 2. Patients with positive amyloid scans who had CMBs were older than those without CMBs [79.47±5.62 vs. 73.89±8.44 (mean±SD, years), p<0.001]. The prevalence of hypertension was also higher in patients with CMBs [n=19 (63.3%) vs. n=30 (41.7%), p=0.046]. It was particularly interesting that the APOE ε4 allele was more common in patients without CMBs than in patients with CMBs [9 of 27 (33.3%) vs. 41 of 67 (61.19%), p=0.022]. Among patients with negative amyloid scans, the mean age and prevalence of hypertension did not differ with the presence of CMBs. The prevalence of the APOE ε2 allele was higher in patients with CMBs than in patients without CMBs [6 of 20 (30.0%) vs. 4 of 59 (6.8%), p=0.007].
In patients with positive amyloid scans, a higher WMH burden was more strongly correlated with the presence of CMBs than the absence of CMBs [2.00 (1.00–3.00) vs. 1.00 (1.00–2.00), median (interquartile range); p<0.001]. The prevalence of lacunar infarcts did not differ with the presence of CMBs in patients with positive amyloid scans. In contrast, the prevalence of CMBs were correlated with the presence of lacunar infarcts than the presence of WMHs [1.00 (0.00–1.00) vs. 0.00 (0.00–0.00), p<0.001] among patients with negative amyloid scans.
The neuropsychological test results are presented in Table 3. Patients with positive amyloid scans who had CMBs performed worse on the K-BNT (14.00±23.76 vs. 31.88±34.68, p=0.02) and phonemic COWAT (20.35±23.25 vs. 31.92±30.20, p=0.04) than did those without CMBs. In contrast, the cognitive function of patients with negative amyloid scans did not differ with the existence of CMBs.
We further performed logistic regression analyses to identify associations between amyloid positivity and the CMBs in each topographic area. The presence of the APOE ε4 genotype (odds ratio=4.218, p<0.001) and lobar CMBs (odds ratio=2.382, p=0.034) was significantly associated with amyloid positivity in patients with cognitive complaints (Model 1). When classified by topographical region, parietal CMBs (odds ratio=3.197, p=0.050) were significantly associated with amyloid positivity (Model 2) (Table 4).
DISCUSSION
This study found that CMBs were present in 25.5% of patients with cognitive decline, which is a higher prevalence than that in the general population (5–6%) and similar to that in patients with stroke.1920 CMBs were more prevalent in the patients with positive amyloid scans, in which they were predominantly located in the lobar area and are known to be more closely linked with CAA.21
Our patients showed distinctive clinical profiles according to the coexistence of CMBs and amyloid pathology. The presence of CMBs was strongly correlated with old age and hypertension in the patients with positive amyloid PET scans, but not in those with negative scans. Old age and hypertension are well known to be risk factors for conventional small-vessel disease, which includes CMBs. CMBs are thought to be caused by small-vessel wall damage due to both vascular risk factors and the accumulation of Aβ.22 We hypothesized that conventional vascular risk factors play more important roles in the expression of CMBs when they coexist with amyloid pathology.
In this study the presence of CMBs was strongly correlated with a higher burden of WMHs in patients with positive amyloid scans but not in those with negative scans. The etiology of WMHs remains unclear, and may be multifactorial to include reduced cerebral blood flow, cerebrovascular reactivity, and leakage across the blood-brain barrier.23 Recent studies have shown that WMHs are closely related to amyloid angiopathy as well as the vascular pathway in patients with AD.2425 In a study of patients with autosomal-dominant mutations for AD, the WMH volume, particularly in posterior regions, appeared to be increased at as long as 22 years prior to symptom onset.26 Other studies have also found that the increased WMHs are closely associated with presence of CMBs—which are possibly representative markers of CAA—in patients with AD.2728 Our results are consistent with previous reports of WMHs being increased in patients with AD and closely associated with CMBs.2829
With regard to the neuropsychological profile, patients with amyloid positivity and CMBs performed worse in confrontation naming and executive function. Previous studies found that CMBs mainly impair executive function and processing speed, which are characteristics of vascular cognitive impairment. 2230 Our results are consistent with those of previous studies, but it was particularly interesting that the neuropsychological performance did not differ with the presence of CMBs in patients with negative amyloid scans. These results suggest that CMBs play a greater role in clinical deterioration in patients with amyloid pathology than in those without this pathology. One previous study indicated that CAA patients exhibit structural network dysfunction, especially projecting to occipital, parietal, and temporal regions, and these associations remained independent after controlling for WMHs, microbleeds, and brain volume. Other studies have also found that patients with CAA presented with a significantly lower global cortical thickness even after controlling for WMHs and microbleeds.31 These findings suggest that CMBs in AD affect cognitive function via an independent pathway mediated by CAA-related vascular dysfunction, rather than a general vascular dysfunction pathway.
The APOE ε2 and ε4 alleles are well-known risk factors for lobar CMBs. The exact role of the APOE genotype is not known, but the findings of several pathological studies suggest that the ε2 allele contributes to vessel weakening or fragility while the ε4 allele contributes to either increased Aβ deposition or decreased Aβ clearance in brain vessels.3233 In the present study, the overall prevalence of the APOE ε4 allele was higher in patients with positive amyloid scans than in those with negative scans. However, among patients with positive amyloid scans, the APOE ε4 allele was more common in those without CMBs than in those with CMBs. The most plausible explanation for this difference is that the APOE ε4 allele contributes more to the parenchymal deposition of amyloid than to vascular deposition such as CAA.34 The prevalence of the APOE ε2 allele did not differ with the presence of CMBs in patients with positive amyloid scans, but it was more common in patients with negative amyloid scans with CMBs than in those without CMBs. This result is consistent with another previous study indicating that the APOE ε2 allele increases CAA in aging, but not in AD patients. This might be due to the protection afforded by the APOE ε2 allele against the risk of AD via effects on other AD-relevant pathways such as inflammation.35 Further investigations of the exact roles of the APOE genotype and of Aβ accumulation and microbleeds are needed.
Finally, we found that lobar CMBs were closely associated with amyloid positivity in patients with cognitive decline, especially when they were located in the parietal lobe. Previous studies have shown that CAA favors posterior brain structures, especially the temporal and occipital lobes.363738 They have also demonstrated a tendency for low Aβ42 levels and high CSF/serum albumin ratios in patients with CMBs in the occipital lobe.39 These findings suggest that CMBs are closely related to damage in the blood-brain barrier that affects amyloid clearance in AD.
Our study was subject to several limitations. First, it did not have a prospective design and included a relatively small sample, which means that causal relationships remain unclear. Second, we analyzed positivity and negativity in amyloid PET scans solely by visual ratings, and so quantitative analyses of amyloid burden were not performed. Finally, CMBs may play distinct roles according to the stage of disease (SCD, MCI, or AD), but we could not analyze our data according to diagnosis. Further studies with larger samples should be able to clarify and extend these results.
In conclusion, we found that the prevalence of CMBs in patients with cognitive decline was higher than that in the general population, and that CMBs play distinctive roles in affecting clinical parameters and neuropsychological profiles according to the coexistence of amyloid pathology. The present findings should be confirmed in prospective studies with larger samples.


 XML Download
XML Download