

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Sleep-related problems in Parkinson's disease (PD) have received increasing attention in past years due to their occurrence in early stages of the disease, as well as their clinical influence on morbidity, disability, and the health-related quality of life (HRQoL) of patients with advanced disease.1234 Parkinson's Disease Sleep Scale (PDSS) is a patient-reported instrument recommended by the Movement Disorder Society task force, and is designed to rate overall sleep problems in the PD population.56 A revision of PDSS (PDSS-2) was recently published that places particular emphasis on improving scale properties and encompassing nocturnal symptoms that were not previously included (e.g., restless leg syndrome, sleep apnea, akinesia, and nocturnal pain).7 PDSS-2 has been successfully applied in several clinical trials as a reliable patient-reported outcome measure.7891011 This prompted us to translate and adapt PDSS-2 to Korean individuals and evaluate its clinimetric properties in the assessment of sleep disturbances among Korean-speaking patients with PD.
This study also sought to determine the discriminatory capacity of the new Korean version of PDSS-2 (K-PDSS-2) by conducting latent class analysis (LCA) to characterize subtypes of sleep disturbance in PD. Several studies have applied LCA in PD populations to address depression-anxiety subtypes1213 and neurocognitive subtypes.14 The potential causes of sleep disturbances vary widely, and have been suggested to include primary insomnia, depression, rapid-eye-movement sleep-behavior disorder (RBD), restless leg syndrome, nocturnal motor symptoms, antiparkinsonian drug side effects, nocturia, and sleep-related breathing disorders, all of which frequently co-occur.134 However, few studies have attempted to empirically outline the clinical heterogeneity of sleep-related problems in patients with PD. LCA has previously been used to identify subtypes of sleep disturbance in patients with Alzheimer's disease.15 An empirical search for latent homogeneous subgroups of patients who experience similar patterns in sleep-related problems and nocturnal disabilities could help to elucidate the pathophysiology of these conditions and lead to the development of more-targeted management strategies. To our knowledge, the present study is the first to document the application of an LCA approach for identifying subtypes of sleep disturbance in patients with PD.
METHODS
Subjects
This study, which had a test-retest design, recruited patients who met the United Kingdom Parkinson's Disease Society Brain Bank criteria for PD between August 2014 and September 2015 from 31 different movement-disorder centers in Korea. All of the patients included in the study were required to be on a known and stable antiparkinsonian medication for the 4 weeks prior to study commencement. Patients with secondary parkinsonism, atypical parkinsonian syndrome, concomitant treatment with hypnotics and/or antipsychotics, a score of <20 on the Korean version of the Mini-Mental State Examination (K-MMSE), or those aged 40 years or younger at disease onset were excluded. Written informed consent was obtained from all of the study participants, and the study protocol was approved by the Institutional Review Boards at the participating centers (IRB No. 2014-08-029). This investigation formed part of a larger nationwide program studying the cultural adaptation and clinimetric validation of different scales for nonmotor manifestations of PD in Korea.216
Translation and cross-cultural adaptation of K-PDSS-2
The original questionnaire was translated from English into Korean by two independent bilingual translators. A translation committee consisting of movement disorder experts reviewed both translated versions to reconcile a single forward-translated version, which was then backward translated from Korean to English by another independent bilingual translator who was blinded to the previous steps. The back-translated version was compared to the original English questionnaire, and forward–backward amendments were made by the translation committee based on consensus. The amended translated version was pretested on four patients with PD who were not a part of this study in order to assess its interpretation of items, ease of comprehension, and cross-cultural relevance. These processes produced the final harmonized version of the K-PDSS-2 instrument.5911
Study procedure
Both demographics and clinical data were collected for all study patients. The overall severity of disease was evaluated using Hoehn and Yahr (H–Y) staging and parts I–III of the Unified Parkinson's Disease Rating Scale (UPDRS). The motor phenotype was classified based on the ratio of UPDRS items proposed by Jankovic et al.17 We administered the Korean version of the Non-Motor Symptoms Scale (K-NMSS) consisting of the following nine domains to quantify the range of nonmotor manifestations of the disease: cardiovascular, sleep/fatigue, mood, perceptual problems, attention/memory, gastrointestinal, urinary, sexual function, and miscellaneous.18 The disease-specific HRQoL was investigated using the Korean version of the 39-item Parkinson's Disease Questionnaire (K-PDQ-39).19 The Korean version of the Montgomery-Åsberg Depression Rating Scale (K-MADRS) was used to assess depressive symptoms, while K-MMSE and the Korean version of the Montreal Cognitive Assessment (Mo-CA-K) were administered to evaluate cognitive function.2021 Sleep-related problems and nocturnal disabilities among the study patients were globally addressed using the K-PDSS-2 instrument obtained from the above-described cross-cultural adaptation process. The test–retest reliability was measured by applying the K-PDSS-2 questionnaire twice over an interval from 10 to 14 days.
Statistical analysis
Clinimetric properties were statistically evaluated using IBM SPSS (version 19, IBM Corporation, Armonk, NY, USA) for internal consistency, test–retest reliability, convergent validity, and scale precision for measurement errors. Cronbach's α coefficients for total scores and item-total correlations for individual items were calculated to assess internal consistency.5 Cronbach's α coefficients >0.70 and item-total correlation coefficients >0.30 were used to tentatively define an acceptable level of consistency.91116 Test–retest reliability was measured with the intraclass correlation coefficient (ICC) using a two-way random model and a criterion of >0.60.722 The scale precision for measurement errors was tested through the standard error of the mean (SEM) using the ICC as the reliability coefficient. The measurement errors of K-PDSS-2 were considered sufficiently low if the SEM was less than half of the standard deviation (SD).79 Convergent validity with the K-NMSS sleep/fatigue domain score and other nonmotor measures of PD were evaluated using the Spearman rank-order correlation coefficient (rs), with a value of rs>0.40 considered to indicate a moderate or stronger correlation.1116 The Jonckheere-Terpstra test for trend detection was used to evaluate the relationship between K-PDSS-2 total scores and the H-Y stages of the study patients, and p values <0.05 were considered to reflect statistical significance.
The discriminatory capacity of the K-PDSS-2 instrument was statistically assessed using LCA, which identifies classes of patients with similar patterns of sleep disturbances. A polytomous-variable LCA was conducted with the open-source statistical software R (version 3.4.1, R Foundation for Statistical Computing, Vienna, Austria) using the R package depmixS4 (version 1.3–3).23 The discrete model fit was assessed based on the interpretability, parsimony of latent classes, Akaike information criterion, and Bayesian information criterion statistics.12,14 Demographics and clinical differences were compared among identified latent classes using the chi-square test or the Kruskal-Wallis test followed by post-hoc comparisons with Bonferroni-corrected Mann-Whitney U tests, as appropriate.
RESULTS
Table 1 presents demographics and clinical data of the 122 patients enrolled in this study. At the baseline evaluation, the K-PDSS-2 score was 11.67±9.87 (mean±SD), with a median of 9 and an interquartile range (IQR) of 4–16. Most (97.5%, n=119) of the 122 study patients who completed the baseline evaluation also participated in the retest K-PDSS-2 evaluation, in which the score was 12.61±11.67, with a median of 10 and an IQR of 4–17. In terms of internal consistency, the item-total correlation coefficient ranged from 0.169 to 0.739 at baseline and from 0.138 to 0.746 at the retest. All items except for item 8 (nocturia) satisfied the criterion of the itemtotal correlation coefficient (>0.30; Table 2). Cronbach's α coefficients for the K-PDSS-2 total scores at baseline and the retest were 0.851 and 0.880, respectively, thereby meeting the standard established for internal consistency (Cronbach's α >0.70; Table 3). With regards to the test–retest reliability over the interval from 10 to 14 days, the ICCs ranged from 0.672 (item 4) to 0.848 (item 7), with ICC >0.60 for all items (Table 2). The ICC of the K-PDSS-2 total score was 0.867, and hence exceeded the threshold of 0.60. The scale precision as determined by the SEM was 3.60, therefore also meeting the criterion (<½SD=4.94).
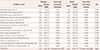
Table 3 lists the coefficients for the correlations between K-PDSS-2 and the range of clinical rating scales of PD used to assess convergent validity. The total K-PDSS-2 score showed significant correlations with the K-PDQ-39 summary index (rs=0.496) and K-MADRS score (rs=0.523), and was strongly correlated with the total K-NMSS score (rs=0.552) and the scores in some of the corresponding K-NMSS domains. As expected, the strongest correlation among K-NMSS domains was observed for the K-NMSS sleep/fatigue domain (rs=0.544; Table 3). There was also a significant relationship between the total K-PDSS-2 score and H-Y stage (standardized Jonckheere-Terpstra statistic=2.091, p=0.037).
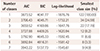
LCAs were conducted with K-PDSS-2 items to identify subtypes of sleep problems, trialing solutions involving from one to seven latent classes. A three-class solution was found to be the most-parsimonious model based on interpretability and fit indices (Table 4). Symptom profiles of the 3 subtypes of sleep disturbance are presented graphically in Fig. 1 as the predicted responses of the study patients in each class on a range of 15 items of K-PDSS-2. Across all study participants (n=122), 78 patients (63.9%) were assigned to class 1, the largest latent class. The symptom profiles of class 1 were characterized by overall low predicted responses on K-PDSS-2 items (Fig. 1), and so individuals in class 1 were labeled as “lesstroubled sleepers.” Twenty-two patients (18.0%) were classified into class 2, with high predicted responses for the restlessness of legs or arms at night (item 4), urge to move legs or arms (item 5), distressing dreams at night (item 6), distressing hallucinations at night (item 7), pain in arms or legs (item 10), muscle cramps in arms or legs (item 11), and tremor on waking (item 13). Since most of these items have been described as PD symptoms at night and motor symptoms at night in previous factor analyses,79 class 2 was labeled “PD-related nocturnal difficulties.” Finally, 22 patients (18.0%) were assigned to class 3, which was profiled by marked predicted responses in bad sleep quality (item 1), difficulties falling asleep (item 2), difficulties staying asleep (item 3), and nocturia (item 8). Since most of these items have indicated disturbed sleep or fragmented sleep in previous factor-analysis studies,7911 individuals in class 3 were labeled as “disturbed sleepers” (Fig. 1).
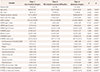
Table 5 compares demographics and clinical variables among the three classes. Group differences based on the Kruskal-Wallis test were found across age, total K-PDSS-2 score (both at baseline and the retest), K-PDQ-39 summary index, UPDRS part I score, K-MADRS score, total K-NMSS score, and scores in four K-NMSS domains (sleep/fatigue, mood, attention/memory, and urinary domains). Post-hoc analysis of between-group differences indicated that the patients in class 3 tended to be younger and have a higher total K-NMSS score, K-NMSS sleep/fatigue domain score, K-NMSS attention/memory domain score, and K-PDQ-39 summary index than those in class 1. Class 3 patients also showed a higher NMSS urinary domain score compared with those in class 1 or 2. Compared to class 1 patients, those in classes 2 and 3 showed a markedly higher UPDRS part I score, K-MADRS score, and K-NMSS mood domain score. There were no significant differences in sex, disease duration, motor phenotype, levodopa equivalent daily dosage, use of antiparkinsonian medication, or UPDRS part II or III scores between the three classes.
DISCUSSION
The purpose of the current study was twofold: to determine 1) the clinimetric properties of the K-PDSS-2 and 2) whether distinct subtypes of sleep disturbance can be distinguished among patients with PD on the basis of the validated K-PDSS-2 instrument.
Overall, the cross-cultural adaptation of the K-PDSS-2 instrument developed using a structured translation and review processes exhibited satisfactory clinimetric attributes. Similar to the original PDSS-2 validation study, we found that the new instrument had good internal consistency and good test–retest reliability.723 The scale precision of the K-PDSS-2 on measurement error was acceptable in terms of the SEM value, which was less than half the SD.79 The SEM of K-PDSS-2 of our study (3.60 <½SD=4.94) was comparable to that found in the original PDSS-2 validation study (3.98<½SD=4.45)7 and the study by the Hungarian group (2.459<½SD=5.404).9
The convergent validity of K-PDSS-2 was well supported by its statistical correlations with other clinical measures. Consistent with the findings of previously published analyses, the sleep-related problems and nocturnal disabilities as measured herein with K-PDSS-2 increased with advancing disease severity according to H-Y stages.924 Higher K-PDSS-2 scores were significantly correlated with worse K-PDQ-39 scores, indicating a relationship between HRQoL and sleep disturbance in PD patients. This finding corroborates previous reports of significant correlations between PDSS-2 scores and the HRQoL as measured via PDQ-39 or its subdomains.7891125 It is important to note that we found no significant correlation between K-PDSS-2 and neurocognitive performance as assessed by both MoCA-K and K-MMSE, whereas depression as assessed by K-MADRS was closely related to the total K-PDSS-2 score. Our results are consistent with two other groups finding no significant correlation between the PDSS-2 total score and cognitive outcomes assessed using the original MoCA9 and MMSE11 instruments.
Using LCA, we were able to classify sleep disturbances in patients with PD into three latent groups: one baseline subtype (class 1), which covered approximately two-thirds of the study patients, and two subtypes (classes 2 and 3) associated with increased sleep disturbances. One remarkable LCA finding was that the three latent classes did not directly parallel all 15 K-PDSS-2 items in terms of severity (i.e., mild, moderate, and severe). Instead, the predicted item responses (Fig. 1) showed that patients in class 2 were more likely to experience more PD-related nocturnal symptoms, whereas patients in class 3 were more likely to report general sleep difficulties than patients in the other subtypes. Our LCA outcomes indicated that sleep disorders in patients with PD are more complicated than simply the degree of severity of sleep disturbances; instead, there are different subgroups of patients with sleep disturbances, including those with PD-specific or general sleep difficulties.
In a recent review, Diederich and McIntyre3 proposed categorizing sleep problems in PD into 1) primary causes relating to degeneration of the brainstem regulatory center and impaired thalamocortical arousal, 2) secondary causes including motor symptoms, nocturnal dyskinesia, and dysautonomia, 3) tertiary causes mainly due to medication, and 4) other causes including depression, cardiac, and pulmonary comorbidity. Louter et al.1 also suggested three main subgroups of sleep disorders in patients with PD: 1) primary sleep symptoms caused by neurodegeneration in sleep-regulating regions, 2) nocturnal disturbances due to PD symptoms, and 3) medication-related sleep disorders. Our study empirically characterized the underlying structure of sleep disturbances in PD that have been and continue to be observed routinely by movement disorder experts and clinical neurologists in practice. The present LCA results suggested that patients in class 3 can suffer from neurodegeneration in sleepregulating regions, whereas patients in class 2 manifest with PD-related nocturnal disturbances.134 Since the K-PDSS-2 instrument did not directly address the medications taken by patients, medication-related sleep problems might not have been sufficiently captured.
It is particularly interesting that the differences between groups of motor symptoms as assessed by UPDRS parts II and III remained small. In contrast, patients identified as being in either class 2 or 3 had more-severe nonmotor symptoms. Our findings of a discrepancy between motor and nonmotor symptoms in relation to sleep-disturbance subtypes are consistent with those of several data-driven subtyping studies in PD that have found patients experiencing PD motor symptoms of similar severities exhibiting considerable differences in the severities of their nonmotor symptoms.26272829
It is important to note the potential limitations of this study. First, our classification of sleep disturbances was based on the K-PDSS-2 instrument, which does not include items related to RBD-related nocturnal motor features.830 The validity of this subtyping has not been tested using polysomnography, sleep latency testing, or actigraphy.3132 RBD, obstructive sleep apnea, or other sleep-related respiratory disturbances can account for some instances of sleep disturbance observed in class 3, warranting further evaluation by objective testing methods such as polysomnography. The second limitation is that our study included only patients with K-MMSE scores ≥20 at the time of registration, and the mild cognitive impairments in PD could go unrecognized if screening is performed using MMSE scores.33 Third, convergent validity was only tested against the corresponding K-NMSS domain (domain 2 of K-NMSS), and not against other generic sleep scales such as the Pittsburgh Sleep Quality Index or the Wisconsin Sleep Questionnaire.634 Fourth, our study did not determine the optimal cutoff score for K-PDSS-2. No such information is provided for Korean patients with PD, and thus further studies are needed to address the cutoff value for the K-PDSS-2 instrument.1024 Another drawback of our study is that measure of daytime sleep disturbances (e.g., excessive daytime sleepiness) and related assessment instruments were not utilized.
In conclusion, the K-PDSS-2 instrument demonstrated clinimetric reliability and validity, indicating that it is a suitable tool for measuring nocturnal disturbances and sleep disorders in Korean patients with PD. Moreover, using a datadriven approach, we were able to identify subtypes of sleep disturbance in patients with PD. The validity of our LCA-derived subtypes was supported by distinct differences in demographics and clinical features between the groups. We expect our findings to be useful in both research and clinical evaluations of sleep disturbances in PD.



 XML Download
XML Download