

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
There has always been a pressing need to develop new antiepileptic drugs (AEDs) due to 20–30% of patients with epilepsy remaining refractory to medical or surgical treatment. AED development since 1990 has focused on specific therapeutic targets, but most of the new AEDs have not resulted in significant changes in the proportion of patients with refractory epilepsy. Glutamate, the main excitatory neurotransmitter, opens cation-permeable ion channels that are abundantly expressed in the mammalian brain.1 The fast excitatory neurotransmission of glutamate is mediated by three classes of ionotropic receptors: α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA), N-methyl-d-aspartate (NMDA), and kainite receptors.2 The AMPA receptor is the main excitatory postsynaptic receptor mediating nearly all fast excitatory neurotransmission, and is expressed throughout the CNS.34 Perampanel, the first selective AMPA receptor antagonist,5 is one of the latest AEDs. Neuronal excitation is reduced by inhibiting AMPA-induced increases in intracellular calcium,6 and this new mechanism of action has greatly improved the quality of life of some patients with intractable epilepsy.
Perampanel was initially approved for adjunctive use in partial-onset seizures in 2012, and was subsequently approved as an adjunctive therapy for primary generalized tonic-clonic seizures in patients with epilepsy aged 12 years or older, and then as a monotherapy for partial-onset seizures with or without secondarily generalized seizures in patients with epilepsy of the same.78 The US Food and Drug Administration (FDA) expanded the approval of perampanel to the treatment of partial-onset seizures with or without secondary generalized seizures in patients as young as 4 years in 2018. This very recent expansion of approval means that there have been few real-life studies on pediatric patients.
The aim of the present study was to determine the long-term efficacy, factors affecting treatment response, and tolerability of perampanel as an add-on therapy in pediatric patients aged 4 years or older with epilepsy.
METHODS
This multicenter retrospective observational study collected data from pediatric epilepsy centers of four Korean national universities. The Institutional Review Board of each university approved the protocol that included patients with refractory epilepsy aged 4 years or older. The IRB numbers for each institution are 2018-08-034 (Kyungpook National University Hospital); 05-2018-025 (Pusan National University Yangsan Hospital); 2018-04-003 (Chungbuk National University Hospital); 2018-09-016 (Chonbuk National University Hospital). The need to obtain informed consent was waived due to the retrospective design of the study.
Perampanel was administered to patients aged 4 years or older who had been diagnosed with epilepsy in a pediatric neurology clinic at the participating university hospitals between January 2016 and December 2017. The patients should have had recurrent seizures while taking at least one AED, and the concomitant AEDs had to have remained unchanged for the duration of the study. Due to this being a multicenter retrospective study, the criteria for the timing of add-on therapy had not been unified. The data collected included the following information: sex, seizure types, presence of intellectual disability, etiology of epilepsy, history of ketogenic diet/vagus nerve stimulation (VNS)/epilepsy surgery, age at seizure onset, age when started on AEDs, age when started on perampanel, duration of epilepsy, duration of perampanel treatment, number of concomitant AEDs, monthly seizure frequency, initial daily dose of perampanel, final daily dose of perampanel, retention at the end of the study, and number of adverse events. Seizure types were classified into generalized, focal, and combined focal and generalized, while epilepsy etiologies were classified into genetic, infectious, metabolic, structural, and unknown.9 The efficacy was assessed based on the mean monthly seizure frequency during the 3 months before starting perampanel treatment. A response was defined as a reduction of 50% or more in the monthly seizure frequency compared with the baseline. Perampanel was given once in the evening and its dosage was increased depending on the clinical response and tolerability. The 2-mg formulation was used in divided doses to increase the daily dose by 0.5 mg or 1 mg. The subjects were divided into two groups by age: A) 4–16 years and B) 17–20 years. Changes in the seizure frequency from baseline, adverse events, and retention rates were obtained at 3, 6, and 12 months. Adverse events and discontinuation profiles were obtained to assess tolerability. Worsening of seizures was classified as an adverse event.
All of the analyses in this study were performed using R software (version 3.2.1, meta package, R Foundation for Statistical Computing, Beijing, China), and all statistical tests were two-sided. Odds ratios with 95% confidence intervals were utilized to evaluate the effect of AEDs for all dichotomous outcomes. The potential heterogeneity was assessed using the Q statistic, χ2-test, and I2. A random-effects model was used to pool the effect size if significant heterogeneity was detected (p<0.05 or I2>50%); otherwise a fixed-effects model was adopted. The retention rate according to age when started on perampanel and according to seizure type were analyzed using Kaplan-Meier survival analysis in SPSS software (version 23; IBM Corp., Armonk, NY, USA).
RESULTS
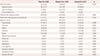
This study included 220 children and adolescents comprising 117 males and 103 females ranging in age from 4 to 20 years (15.4±2.9 years, mean±SD). Most (84%) of the patients had intractable epilepsy, and their duration of perampanel treatment was 11.5±6.9 months. The starting dosage of perampanel was 2.0±0.2 mg/day and the final dosage was 5.5±2.8 mg/day. The retention rate at the end of the study was 70.5%. Table 1 compares demographics and clinical features between the two age groups when they were started on perampanel. There were no significant subgroup differences in sex ratio, seizure type, history of ketogenic diet, VNS, epilepsy surgery, age when started on AEDs, duration of perampanel treatment, number of concomitant AEDs, initial and final daily doses of perampanel, or retention rate. Patients in group A (aged 4–16 years) had more intellectual disability, more infectious or structural etiologies, and a higher baseline monthly seizure frequency than those in group B (aged 17–20 years).
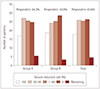
The overall response rate was 43.6%, and the seizure-freedom rate was 17.7%. The response rate did not differ significantly between group A (44.2%) and group B (42.9%) (Fig. 1). The overall retention rate was 85.0% at 3 months, 71.8% at 6 months, and 50.5% at 12 months, and the retention rate according to age when started on perampanel did not differ significantly among the groups (Fig. 2).
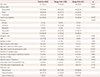
Comparing demographics and outcomes between responders and nonresponders (Table 2) revealed that both the age at seizure onset (p=0.005) and the age when started on AEDs (p=0.002) were significantly higher in responders than in nonresponders. The duration of epilepsy (p=0.013) was significantly shorter and the duration of perampanel treatment (p<0.001) was significantly longer in responders than in nonresponders. The number of patients with intellectual disability (p=0.003) and the number of concomitant AEDs (p<0.001) were significantly smaller in responders than in nonresponders. The discontinuation rate was lower (p<0.001) and the point of discontinuation (p<0.001) was later in responders than in nonresponders.
In a logistic regression model of factors affecting a good treatment response and seizure freedom (Table 3), a good treatment response was negatively correlated with the presence of intellectual disability (p=0.0259) and the number of AEDs (p=0.0018). Seizure freedom was negatively correlated with the number of AEDs (p<0.0001) and the baseline seizure frequency (p<0.04).
As indicated in Table 4, in terms of adverse events and discontinuation profiles of treatment groups by age, 40% of patients experienced adverse events, and some of the adverse events occurred simultaneously. The dosage when adverse events occurred was 5.3±3.2 mg/day. Perampanel was discontinued in 29.5% of the patients, and the rate of discontinuation due to side effects was higher in group B than in group A. Somnolence was more common in group A than in group B, and it was the most common adverse event, followed by dizziness, ataxia, violence, anger, worsening of seizure, insomnia, headache, depression, low appetite, cognitive decline, and nausea/vomiting, while there was one suicide attempt. The side effects (other than the single suicide attempt) were mild in severity and resolved after the dose reduction or discontinuation of perampanel. The patient who attempted suicide was a 16-year-old female with a history of impulse control disorder and anxiety. She had visited a psychiatrist but had never attempted suicide before taking perampanel. She cut her wrist while taking perampanel, was admitted to a psychiatry department, and diagnosed with bipolar disorder. After discontinuing perampanel she has not displayed any further suicidal tendencies. The wrist wound was nonlethal and she made a full recovery.
The efficacy, tolerability, and factors affecting a good treatment response of perampanel in pediatric patients aged 4 years or older with epilepsy are summarized in Fig. 3.
DISCUSSION
The efficacy of perampanel add-on therapy in children and adolescents in this study was similar to that found in previous studies. The first multicenter study of children and adolescents aged 2–17 years with various types of epilepsy found a 31% response rate and 9% seizure-freedom rate, which are similar to adult data.10 In subsequent studies involving children and adolescents, the response rate has ranged from 42% to 59% and the seizure-freedom rate has ranged from 5% to 12.5%.11121314 Children aged 6 years or older have tended to show better responses (36%) than very young children (9%),10 as also revealed by a comparison between children aged 12 years and older (54%) and younger (25%) children.12 However, no significant difference according to age groups was found in our study, which included a larger number of patients.
The factors affecting the treatment response based on a logistic regression model indicated that good response can be expected in patients without intellectual disability and with a small number of concomitant AEDs. The factors affecting seizure freedom were a small number of concomitant AEDs and a low baseline monthly seizure frequency.
While the number of concomitant AEDs was related to the treatment response, the presence of enzyme-inducing AEDs was not. Perampanel is primarily metabolized by CYP3A4 of the P450 enzyme system, and enzyme-inducing drugs such as carbamazepine, oxcarbazepine, and phenytoin significantly increase the clearance of perampanel and decrease its plasma concentration.1516 Perampanel has been studied in the presence of various AEDs, including enzyme-inducing AEDs, and there have been improved treatment outcomes regardless of the types of concomitant AEDs despite the known interaction between perampanel and enzyme-inducing AEDs.1718 Unlike in previous studies, our patients were not affected by concomitant enzyme-inducing AEDs. However, increased dosages and the faster titration of perampanel may be needed when a patient is taking enzyme-inducing AEDs.19
The overall safety profile in our study was similar to previous reports. The rate of adverse events occurring in children and adolescents ranged from 31% to 71%, and the most frequently reported ones include behavioral changes, dizziness, somnolence, and gait disturbance.10111213 Particular attention should be paid to younger patients because they are more susceptible to somnolence. Most adverse events were mild in severity, with the exception of a single suicide attempt; this potentially serious adverse event occurred in a patient with impulse control disorder and anxiety. Although she had underlying psychiatric problems, she had not had any suicidal tendencies before taking perampanel. She was started on a daily perampanel dose of 2 mg, and this was increased slowly by 1 mg per month before reaching 5 mg. While on a 5-mg dose of perampanel she cut her wrist and was admitted to a psychiatry department. The FDA lists ‘serious psychiatric and behavioral reactions’ as a potential adverse effect of perampanel, and psychiatric adverse events including suicidal ideation are the most common reasons for withdrawal.20 In a retrospective study in Canada, 50% of pediatric patients experienced adverse behavioral events that resulted in perampanel withdrawal, and 58% of them had behavioral comorbidities.11 Thus, adverse events should be carefully monitored especially in patients with underlying behavioral/psychiatric problems, even when starting on a low dose and slowly increasing it until reaching the final dose.
By including 220 pediatric patients aged 4 years or older, this was the largest study to evaluate the efficacy, factors affecting treatment response, and tolerability of perampanel in epilepsy as an add-on therapy. It is suggested that adjunctive treatment with perampanel can be efficacious and tolerated, and that early perampanel treatment may help to lower the seizure burden and improve the quality of life in pediatric patients with epilepsy. Further prospective studies of young children or even infants with refractory epilepsy are needed to elucidate the benefit of perampanel in those populations.




 XML Download
XML Download