

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Intracranial cerebral atherosclerosis (ICAS) is a major risk factor for cerebrovascular disease, particularly in Asians. ICAS is also associated with recurrent stroke, stroke-related morbidity, and future mortality.1 The importance of ICAS for stroke patients and the associated factors and risk factors remain unclear, although they have been suggested to be aging, racial differences (mainly Asian), hypertension, diabetes mellitus, smoking, obstructive sleep apnea, and obesity.234 Thus, further evaluations to find the factors that explain ICAS are necessary.
Fibroblast growth factor 23 (FGF23) is an endocrine FGF and phosphaturic hormone mainly formed by osteoblasts and osteocytes.5 In harmony with Klotho (a single-pass transmembrane protein expressed in renal tubules), as an obligate coreceptor to bind and activate FGF receptors, FGF23 is activated during bone mineralization and turnover defects.6 In addition, kidney dysfunction, adipose tissue inflammation, and vitamin D dysregulation are involved in systemic FGF23 regulation.7 FGF23 is also involved in systemic atherosclerosis via nitric-oxide-associated endothelial dysfunction and calcium-phosphate-related bone mineralization.8 Previous studies have found increased FGF23 to be associated with subclinical atherosclerosis and an increased left ventricular mass.91011 Furthermore, FGF23 is an independent predictor of cardiovascular events in the general population.12
Major features of ICAS include atherosis caused by cholesterol deposition and inflammation and sclerosis secondary to endothelial dysfunction, leading to arterial stiffness.1 Because FGF23 is also involved in the development of atherosclerosis and endothelial dysfunction,9101113 this growth factor might also be associated with the atherosclerosis of intracranial vessels. We hypothesized that a higher circulating FGF23 concentration is associated with the presence and burden of cerebral atherosclerosis in patients with acute ischemic stroke.
METHODS
Subjects
We prospectively registered 262 patients with first-ever ischemic stroke who were admitted to our institution between June 2014 and May 2016 within 7 days after symptom onset and had a stroke subtype classified as large-artery atherosclerosis, cardioembolism, or small-vessel occlusion. Standard protocols for the stroke registry were applied to all patients, which included a chest X-ray; 12-lead electrocardiography; routine blood tests at admission (white blood cell count, WBC) and creatinine) and after a 12-h fast {vitamin D [25(OH)D], fasting glucose, HbA1c, triglyceride, total cholesterol, low-density lipoprotein, total calcium, phosphate, albumin, alkaline phosphatase, uric acid, and CRP}; brain imaging with CT and/or MRI; and vascular imaging with CT angiography, magnetic resonance angiography (MRA), or digital subtraction angiography.1415 Patients who did not agree to participate in the study, refused to provide blood samples, or who had a history of cancer, autoimmune disease, or bone fractures during the previous 2 months were excluded.
Risk factors were defined as in a previous study and the Supplementary Materials (in the online-only Data Supplement).16 The stroke subtype was classified using the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification system.17 Briefly, patients with potential cardiac emboli were classified as the cardioembolic subtype. If a patient exhibited substantial stenosis of the relevant artery, they were classified as the large-artery atherosclerosis subtype. The small-vessel occlusion subtype was defined if all of the following criteria were met: clinical manifestation of classical lacunar syndrome, relevant subcortical or brainstem lesion, infarction smaller than 15 mm, no significant stenosis in the relevant artery, and no potential cardiac embolism.18 The Fazekas scoring system was used to assess white-matter hyperintensities (WMHs) in MRI FLAIR.19 A Fazekas score of ≥2 in the periventricular or deep white matter was defined as high-grade WMH. The renal function was investigated using the estimated glomerular filtration rate according to the Modification of Diet in Renal Disease study equation.20 This study was approved by our Institutional Review Board (approval no. ECT 2014-04-023), and we obtained informed consent from all participants and their next of kin.
MRI protocol and definition of vascular stenosis
Every patient enrolled in this study underwent intracranial and extracranial MRA. All MR images were obtained using a 3.0-T imaging system (Magnetom Verio, Siemens Healthcare, Erlangen, Germany). Three-dimensional time-of-flight sequences were used to evaluate the intracranial arteries (intracranial internal carotid artery, middle cerebral artery, anterior cerebral artery, posterior cerebral artery, distal vertebral artery, and basilar artery) and the extracranial arteries (extracranial internal carotid artery and common carotid artery). Extracranial cerebral atherosclerosis (ECAS) was not assessed in the extracranial vertebral arteries because it is difficult to distinguish hypoplasia of the vertebral artery from significant stenosis.3
The method used in this study to evaluate stenosis has been described previously,21 and >50% stenosis was defined as ICAS.22 ECAS was assessed using the criteria from the North American Symptomatic Carotid Endarterectomy Trial, with its presence defined as >50% stenosis at the bifurcation of the bilateral carotid artery.23 The most serious lesion was chosen when multiple stenotic lesions were present.2224 The total number of vessels with ICAS was considered as the ICAS burden (ranging from 0 to 11), while the total number of vessels with ECAS was considered the ECAS burden (ranging from 0 to 4).24 Two neurologists blinded to clinical information (Y.C. and T.J.S.) independently assessed the presence of ICAS. The kappa value for interobserver agreement was 0.936 for the presence of ICAS. Any initial disagreements in the neurologist assessments of ICAS were resolved by discussion.
Measurement of plasma FGF23 concentrations
To measure the plasma FGF23 concentration, a blood sample were collected after a 12-h fast in EDTA tubes. The blood was centrifuged at 1,900×g and 4℃ for 15 min to obtain plasma, and then kept at −80℃ until being analyzed. The plasma FGF23 concentrations were measured using an ELISA with a commercial reagent (Kainos Laboratories, Tokyo, Japan).25 The concentration detection range was 3–800 pg/mL, and so the assay was repeated using a 1/10 dilution for concentrations >800 pg/mL.25 The plasma FGF23 concentration was measured twice by two investigators blinded to the medical data (Y.C. and D.R.R.) and then averaged. Intra- and interassay coefficients of variability were 4.2% and 6.5%, respectively.
Statistical analysis
Statistical analyses were conducted using the SPSS software package for Windows (version 21.0, IBM Corp., Armonk, NY, USA). Continuous variables were analyzed using the independent t-test, Mann-Whitney test, one-way ANOVA with Bonferroni's post-hoc analysis, and Kruskal-Wallis test. Categorical variables were analyzed using the chi-square or Fisher's exact test. Univariate and multivariate binary logistic regression analyses were performed to investigate the association between the plasma FGF23 concentration and cerebral atherosclerosis. To investigate the associations of age, body mass index, stroke severity, time to blood sampling from symptom onset, and blood laboratory findings with FGF23, Spearman correlation analysis was performed for the correlations between the National Institutes of Health Stroke Scale (NIHSS) score, blood laboratory findings, and FGF23 concentration.
The association between the plasma FGF23 concentration and the burden of cerebral atherosclerosis was investigated by performing a Spearman correlation analysis and univariate and multivariate ordinal logistic regression analyses. Ordinal logistic regression was used to analyze the association between the FGF23 concentration and the number of arteries with cerebral atherosclerosis. The odds ratio (OR) in ordinal regression expresses the common odds for the increase in the number of arteries with cerebral atherosclerosis at each count. Sex, age, and variables for which p<0.1 in the univariate analysis were included in the multivariate logistic regression. In the multivariate analysis, sex, age, body mass index, coronary artery disease, prestroke antithrombotics, stroke subtype, NIHSS score, high-grade WMHs, Klotho, triglyceride, WBC count, total calcium, and C-reactive protein were adjusted for the presence and burden of ICAS; sex, age, hypertension, stroke subtype, NIHSS score, high-grade WMHs, WBC count, phosphate, and uric acid were adjusted for the presence and burden of ECAS; and sex, age, hypertension, prestroke antithrombotics, NIHSS score, high-grade WMHs, Klotho, triglyceride, WBC count, and C-reactive protein were adjusted for the presence and burden of both ICAS and ECAS. For sensitivity analysis, we investigated the presence of statistical interactions according to underlying renal dysfunction (<60 mL/min/1.73 m2), which was closely related to the plasma FGF23 concentration.11 A two-tailed probability value of p<0.05 was considered statistically significant.
RESULTS
Demographic data and comparative analysis according to presence of cerebral atherosclerosis
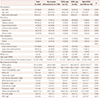
Fig. 1 shows a flowchart of participants according to the inclusion and exclusion criteria applied in this study. The demographics and accompanying risk factors and prior stroke medications did not differ significantly between the included and excluded patients (Supplementary Table 1 in the online-only Data Supplement). Table 1 lists the demographics of the patients in our study. The 262 patients included 58.0% (n=152) males. The mean age was 64.7 years, and the plasma FGF23 concentration was 347.5±549.6 pg/mL (mean±SD). The most common stroke subtype was large-artery atherosclerosis (41.2%, n=108), followed by small-vessel occlusion (40.8%, n=107) and cardioembolism (17.9%, n=47). The plasma FGF23 concentration did not differ among stroke subtypes (p=0.174). ICAS only, ECAS only, and both ICAS and ECAS were present in 31.2% (n=82), 4.9% (n=13), and 6.8% (n=18) of the subjects, respectively (Table 1). The patients with ICAS and both ICAS and ECAS were older (p=0.002) and had higher NIHSS scores (p=0.002) than those without cerebral atherosclerosis. Moreover, patients with ICAS only, ECAS only, or both ICAS and ECAS more often had a history of hypertension (p=0.003) and large-artery atherosclerosis stroke subtype (p=0.001).
The blood laboratory findings indicated that the plasma FGF23 concentration (p=0.001), WBC count (p=0.014), and C-reactive protein concentration (p=0.017) were higher in patients with both ICAS and ECAS than in patients without cerebral atherosclerosis. Patients with ICAS had higher plasma concentrations of FGF23 (p=0.037) and C-reactive protein (p=0.043) compared with patients without cerebral atherosclerosis. Patients with both ICAS and ECAS had a higher plasma FGF23 concentration compared with patients with only ICAS (p=0.001) or only ECAS (p=0.001) (Table 1).
The plasma FGF23 concentration was positively correlated with age (ρ=0.150, p=0.015), NIHSS score (ρ=0.198, p=0.001), vitamin D [25(OH)D] concentration (ρ=0.143, p=0.020), HbA1c (ρ=0.162, p=0.008), triglyceride concentration (ρ=0.319, p<0.001), WBC count (ρ=0.130, p=0.035), and creatinine (ρ=0.178, p=0.004), total calcium (ρ=0.153, p=0.043), phosphate (ρ=0.148, p=0.048), and C-reactive protein (ρ=0.134, p=0.030) concentrations. Moreover, the plasma FGF23 concentration was negatively correlated with the Klotho concentration (ρ=−0.325, p<0.001).
Association of FGF23 with presence of cerebral atherosclerosis
In a multivariate binary logistic analysis, the plasma FGF23 concentration was positively correlated with the presence of ICAS even after adjustment as a continuous variable (per 100 pg/mL) (OR=1.07, 95% CI=1.00–1.15, p=0.039) or dichotomizing based on the median value (cutoff value=182.0 pg/mL; OR=2.52, 95% CI=1.36–4.68, p=0.003) and tertiles [comparing the upper tertile (≥235.16 pg/mL) with the lower tertile (0–146.79 pg/mL): OR=3.28, 95% CI=1.53–7.05] (Table 2, Supplementary Table 2 in the online-only Data Supplement). The plasma FGF23 concentration was marginally related to the presence of ECAS after adjustment as a continuous variable (per 100 pg/mL; OR=1.05, 95% CI=0.99–1.12, p=0.073), but it was not associated with the presence of ECAS after adjustment using the median cutoff value or tertiles (Table 2, Supplementary Table 2 in the online-only Data Supplement). The plasma FGF23 concentration was significantly and positively correlated with the presence of both ICAS and ECAS after adjustment as a continuous variable (per 100 pg/mL; OR=1.10, 95% CI=1.02–1.19, p=0.013) (Table 2, Supplementary Table 2 in the online-only Data Supplement).
There was no statistical interaction between the presence of ICAS (p for interaction=0.872) and ECAS (p for interaction=0.764) with the presence of renal dysfunction (<60 mL/min/1.73 m2).
Association of FGF23 with the burden of cerebral atherosclerosis
The plasma FGF23 concentration was associated with the ICAS burden (ρ=0.317, p=0.001) and the ECAS burden (ρ=0.145, p=0.019). The association of FGF23 with the burden of cerebral atherosclerosis is presented as Fig. 2. In a multivariate ordinal logistic analysis, the plasma FGF23 concentration was positively correlated with the burden of ICAS even after adjustment as a continuous variable (per 100 pg/mL; OR=1.09, 95% CI=1.04–1.15, p=0.001) or dichotomizing based on the median value (cutoff value=182.0 pg/mL; OR=1.10, 95% CI=1.58–5.06, p=0.001) and tertiles [comparing the upper tertile (≥235.16 pg/mL) with the lower tertile (0–146.79 pg/mL): OR=3.30, 95% CI=1.60–6.75] (Table 2, Supplementary Table 3 in the online-only Data Supplement). The plasma FGF23 concentration was related to the burden of ECAS after adjustment as a continuous variable (per 100 pg/mL; OR=1.06, 95% CI=1.00–1.12, p=0.038) but not after adjustment using the median cutoff value or tertiles (Table 2, Supplementary Table 3 in the online-only Data Supplement). The plasma FGF23 concentration was significantly and positively correlated with the burden of both ICAS and ECAS after adjustment as a continuous variable (per 100 pg/mL; OR=1.10, 95% CI=1.02–1.19, p=0.013) (Table 2, Supplementary Table 3 in the online-only Data Supplement).
DISCUSSION
The key finding of our study is that a higher plasma FGF23 concentration was associated with the presence and burden of cerebral atherosclerosis, particularly for ICAS. An association of FGF23 with cerebral atherosclerosis has rarely been reported. A community-based study found that a higher circulating FGF23 concentration was associated with systemic atherosclerosis.26 Moreover, a higher FGF23 concentration was found to be a risk factor for chronic kidney diseases, especially in older, disabled, community-dwelling females.27 In patients with chronic kidney diseases, an elevated FGF23 concentration reportedly contributes directly to a higher rate of left ventricular hypertrophy28 and a higher coronary artery disease burden.29 Combined with previous research, the present study is significant because it confirms the association between the plasma FGF23 concentration and the presence and burden of cerebral atherosclerosis, specifically in stroke patients.
While our study cannot suggest the exact mechanism linking plasma FGF23 and cerebral atherosclerosis, there are plausible hypotheses. First, vascular inflammation of cerebral arteries may explain the relationship between FGF23 and cerebral atherosclerosis. Previous studies have found FGF23 to be an important mediator of vessel inflammation that preceded arteriolosclerosis or arterial stiffness, which was the main cause of cerebral atherosclerosis development, particularly for ICAS.2230 Moreover, FGF23 stimulates the hepatic secretion of the inflammatory markers IL-6 and C-reactive protein.30 C-reactive protein is a sensitive indicator of vascular inflammation and a marker of cerebral atherosclerosis.31 In line with these previous results, the present study found that the plasma FGF23 concentration was positively correlated with that of C-reactive protein, with the latter also being higher in patients with accompanying ICAS than in those without cerebral atherosclerosis. Second, FGF23 is a phosphaturic hormone produced mainly by osteoblasts and osteocytes, and is implicated in blood calcium and phosphate concentrations, the vitamin D pathway, and ectopic site mineralization.5 Increased FGF23 activity disturbs the calcitriol-calcium/phosphate regulation pathway, which may cause hypercalcemia and hyperphosphatemia, likely accounting for the association with ectopic site mineralization.3233 Previous studies have demonstrated the serum calcium concentration to be positively correlated with the presence of ICAS; in contrast, the serum phosphate concentration was not associated with ICAS.34 Furthermore, the phosphate concentration was positively correlated with a greater prevalence of vascular calcification, which is frequently associated with ECAS.3536 Therefore, an FGF23-related calcium-phosphate regulation mechanism may affect the development of cerebral atherosclerosis. Actually, the present study found that the plasma FGF23 was positively correlated with serum calcium and phosphate concentrations, and also that the serum calcium and phosphate concentrations were related to the presence and burden of ICAS and ECAS, respectively.
This study found that the presence and burden of ICAS were significantly associated with a higher FGF23 concentration, whereas the presence and burden of ECAS were not, even though they were related in a univariate analysis. These results may have been due to the sample being too small to reveal a relationship between FGF23 and ECAS. Moreover, other confounding factors such as hypertension are more strongly associated with ECAS than with the FGF23 concentration. In addition, arterial stiffness may be associated with ICAS (rather than ECAS) in Asians,22 and arterial stiffness is also closely related to FGF23,37 which may explain our results. Our study also suggests the presence of a pathophysiological association between circulating FGF23 and ICAS.
This study was subject to some limitations. We did not measure the plasma FGF23 concentration in the general population. However, the main goals of our study were to determine any associations with the presence and burden of cerebral atherosclerosis in stroke patients. All blood samples and brain imaging findings in this study were acquired from acute stroke patients at the time of admission, and so serial changes in the FGF23 concentration and the association of FGF23 with the long-term progression of cerebral atherosclerosis could not be investigated. Although our study prospectively enrolled ischemic stroke patients, it is difficult to generalize our findings and selection bias might have been present due to the smallness of the sample and the exclusion of undetermined stroke subtypes. Even though the plasma FGF23 concentration was found to be associated with the presence of ICAS and ECAS, it did not differ among stroke subtypes. This may have been due to the cardioembolic stroke mechanism or the sample smallness reducing the statistical power. Finally, we did not measure thyroid and parathyroid hormones that may affect the FGF23 concentration, or examine bone abnormalities in the enrolled patients.
In conclusion, this study has demonstrated that a higher plasma FGF23 concentration is independently associated with the presence and burden of cerebral atherosclerosis, particularly with ICAS in stroke patients. We attribute these associations to the essential role of FGF23 in cerebral atherosclerosis.



 XML Download
XML Download