

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Neuropathic pain is defined by the International Association for the Study of Pain (IASP) as pain that arises as a direct consequence of a lesion or disease affecting the somatosensory system.1 Such pain is generally resistant to treatment and profoundly affects the quality of life.23 Neuromyelitis optica spectrum disorder (NMOSD) and multiple sclerosis (MS) are inflammatory diseases of the CNS, and conditions involving CNS inflammation such as myelitis are associated with neuropathic pain.23 NMOSD was previously regarded as a variant of MS, but since the identification of pathogenic anti-aquaporin-4 immunoglobulin G (AQP4-IgG), NMOSD has been considered a distinctive disease entity with a pathogenic mechanism that differs from that of MS.45 Pain was reported to be more common and severe in NMOSD patients than in MS patients.67 Because of different pathogeneses, the neuropathic pain would be also different between NMOSD and MS groups. However, previous studies have not differentiated neuropathic pain and non-neuropathic pain, and thorough comparative analyses focused on neuropathic pain and its impact on daily life in NMOSD and MS patients have not been conducted.67 The aim of the current study was therefore to compare the characteristics of neuropathic pain and its impacts on daily life between NMOSD and MS patients.
METHODS
Patients
Fig. 1 presents a flow chart of the pain investigation in this study. Between 2016 and 2018, a total of 500 patients with NMOSD and MS from six referral medical centers in Korea underwent pain investigations. NMOSD patients fulfilled the 2015 diagnostic criteria for NMOSD and MS patients met the 2010 McDonald criteria.89 In accordance with the IASP, pain was defined as an unpleasant sensory or emotional experience associated with actual or potential tissue damage, or described in terms of such damage.1 Overall, 151 of the 252 NMOSD patients and 85 of the 248 MS patients complained of current pain. As women are more vulnerable to pain than men and the pain may be influenced by longer disease duration,6710 the two patient groups were matched for sex ratio and disease duration.
To investigate neuropathic pain, Korean version of the PainDETECT questionnaire1112 was applied for the patients with current pain at least 3 months after acute clinical relapse. The patients who suffered from pain syndromes that did not directly result from CNS damage associated with NMOSD and MS such as migraine, herniated intervertebral disc, and postherpetic neuralgia were excluded. Finally, the PainDETECT questionnaires completed by 157 patients were analyzed: 99 NMOSD patients (91 with AQP4-IgG) and 58 MS patients.8913 The Korean version of the short form of the Brief Pain Inventory (BPI)14 was subsequently analysed in 50 NMOSD patients and 24 MS patients experiencing pain with a neuropathic component (PainDETECT score >12). Because involvement of the spinal cord is one of the well-known causes of central neuropathic pain,1516 the frequency of previous myelitis attacks was compared between the NMOSD and MS patients. Expanded Disability Status Scale (EDSS) scores of the enrolled patients were used to evaluate their neurological disability status.17 The Institutional Review Board of the participating hospitals approved the study protocol (IRB Nos. NCC 2014-0146, KC17T-EDI0427, KUGH 2016-07-040-001).
Questionnaires
PainDETECT questionnaire
The PainDETECT questionnaire consists of three categories.1112 The first is the severity of pain, which consists of seven descriptive components for evaluating the features of neuropathic pain on a 6-point Likert scale ranging from 0 (no pain) to 5 (very strong pain). The neuropathic pain descriptions in this category include burning, tingling/prickling, mechanical allodynia, sudden electric shock-like sensations, thermal hyperalgesia, numbness, and pain aggravated by pressure. The second category pertains to the patterns of pain, which is rated as persistent pain with slight fluctuations, persistent pain with pain attacks, or pain attacks without pain between them, or pain attacks with pain between them. For the latter two of these patterns 1 extra point is added to the total score, while for persistent pain with slight fluctuations no points are added, and for persistent pain with pain attacks, 1 point is subtracted from the total score. The final category assesses radiating pain via a simple ‘yes’ or ‘no’ question, with 2 points added to the total score for a ‘yes’ response. The scores derived from the three categories are added, producing a maximum possible score of 38. Scores of 19 or greater are considered strongly suggestive of neuropathic pain, scores of 13–18 are suggestive of pain with a neuropathic component, and scores of 12 or less suggest that neuropathic pain is unlikely to be present.
Short form of the Brief Pain Inventory
The BPI comprises two main components, pain severity and pain-related interference in daily life.14 The severity component is scored from 0 (no pain) to 10 (the severest pain subjects can imagine), and subjects rate the severity of their pain via individual questions for the present, worst, least, and average pain, with the average of these four scores representing their pain severity index score. The pain-related interference score has the following seven domains: general activity, mood, walking ability, capacity for normal work, relationships with other people, sleep, and enjoyment of life. Respondents rate interference in daily life on a scale from 0 (no interference) to 10 (complete interference), and the scores are added to obtain a total pain-related interference score. The current study also investigated whether the patients were currently taking pain medication and the percentage of pain relief they ascribed to that pain medication within 24 hours.
RESULTS
Clinical characteristics and frequencies of neuropathic pain in NMOSD and MS patients
The sex ratio, disease duration, and presence of immunological therapy did not differ between the NMOSD and MS patients, whereas both current age and EDSS scores were higher in NMOSD patients than in MS patients (Table 1). Neither BDI scores nor FSS scores differed significantly between the two groups. A PainDETECT status of being strongly suggestive of neuropathic pain (score >18) was significantly more frequent in NMOSD patients than in MS patients. (27% vs. 12%, p=0.043) (Fig. 1). A PainDETECT status suggestive of pain with a neuropathic component (score >12) was also more common in NMOSD patients than in MS patients, but the difference was not statistically significant.
PainDETECT questionnaire
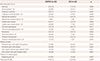
Table 2 presents the results derived from the PainDETECT in NMOSD and MS patients. The values of pain descriptions in all domains were higher in NMOSD patients than in MS patients, with the differences being statistically significant for mechanical allodynia [1.1±1.4 vs. 0.5±1.0 (mean±SD), p=0.014] and thermal hyperalgesia (1.5±1.6 vs. 0.9±1.2, p=0.011), whereas those for burning, tingling/prickling, sudden pain attacks, numbness and pressure-induced pain were not statistically significant. There were also significant differences between the NMOSD and MS groups with regard to severe or very severe pain ratings (score >3) for tingling or prickling (25% vs. 10%, p=0.024), mechanical allodynia (9% vs. 0%, p=0.027), sudden pain attacks (29% vs. 12%, p=0.018), and thermal hyperalgesia (18% vs. 2%, p=0.002). There was no significant difference in the patterns of pain between NMOSD and MS patients, but radiating pain was significantly more frequent in NMOSD patients (47% vs. 24%, p=0.007). The total PainDETECT score was significantly higher in NMOSD patients than in MS patients (13.9±7.3 vs. 10.3±6.0, p=0.002).
BPI and previous myelitis in NMOSD and MS patients experiencing pain with a neuropathic component
The pain severity index was significantly higher in NMOSD patients than in MS patients (5.0±1.8 vs. 4.0±1.6, p=0.017), as was the total pain-related interference score on the BPI (33.8±15.0 vs. 26.1±15.1, p=0.045) (Table 3). Pain-related interferences in normal work (p=0.045) and in relationships with other people (p=0.039) were significantly greater in NMOSD patients than in MS patients. The current use of pain medication was more prevalent in NMOSD patients than in MS patients (82% vs. 60%, p=0.046), while the percentage of pain relief derived from that medication was lower in NMOSD patients [50% (range=10–100%) vs. 60% (range=30–100%), p=0.037). Unsatisfactory pain relief (≤30%) by analgesics was significantly more frequent in NMOSD patients than in MS patients (38% vs. 13%, p=0.031). The prevalence of previous myelitis did not differ between NMOSD and MS patients experiencing pain with a neuropathic component.
DISCUSSION
This study involving a large multicenter cohort of patients with CNS inflammatory diseases found that neuropathic pain was more severe in NMOSD patients than in MS patients. The PainDETECT questionnaire was developed by a German neuropathic pain research network to distinguish nociceptive pain from neuropathic pain, and one of the largest databases for neuropathic pain was established using this questionnaire.20 We observed that the PainDETECT scores for mechanical allodynia and thermal hyperalgesia—which are representative of central neuropathic pain—were significantly higher in NMOSD patients than in MS patients, with strong involvement (score >3) of these types of pain also being significantly frequent in NMOSD patients. Among patients experiencing pain with a neuropathic component (PainDETECT score >12), the pain severity and pain-related interference were both significantly greater in NMOSD patients than in MS patients. The prescription of pain medication and the presence of insufficiently controlled pain despite treatment were significantly more common in NMOSD patients than in MS patients. Neuropathic pain is known to be influenced by the depression and fatigue status,21 the BDI and FSS scores did not differ between the NMOSD and MS patients in the present study. Collectively, more special attention to prudent pain evaluation and active pharmacological management should be considered in NMOSD patients than in MS patients.
One of the well-known causes of central neuropathic pain is involvement of the spinal cord.1516 Although the frequency of previous myelitis attacks did not differ significantly between NMOSD and MS patients experiencing pain with a neuropathic component (PainDETECT score >12) (Table 3), the degree of mechanical allodynia and thermal hyperalgesia—which can be predominantly influenced by CNS inflammation22—was significantly higher in NMOSD patients than in MS patients. Therefore, the difference in the extent and location of the spinal cord lesions between NMOSD and MS patients is likely to explain this difference. The spinal cord is often more extensively affected in NMOSD patients than in MS patients, with gray matter being preferentially affected.2324 The nociceptive nerve fibers from the nociceptive signaling pathway terminate at laminae I and II in the gray matter in the spinal cord.25 The preferential involvement of the nociceptive signaling pathway in gray matter in NMOSD may contribute to neuropathic pain being more severe in those patients than in MS patients.24 Additionally, radiating pain was more prevalent in NMOSD compared to MS patients, which might be due to dorsal root ganglion damage resulting from fulminant inflammatory involvement of the spinal cord.24
Despite the fact that pain medication was prescribed by several physicians from different hospitals, pain medication including anti-epileptic drugs and/or opioids was consistently prescribed, as was the sequential titration of pain medication. When the neuropathic pain medication was not sufficient to control the symptoms, a combination of pain medications was applied. While pain medication was prescribed using a consistent therapeutic approach, it was subjectively reported that the effectiveness of neuropathic pain medication was worse in NMOSD compared to MS patients. Moreover, the interference in daily life among patients experiencing pain with a neuropathic component was much greater in NMSOD patients than in MS patients. Taken together these results suggest that neuropathic pain that may impact daily life should be considered as an important clinical symptom and treated via a multidisciplinary approach in NMOSD patients. Further studies focused on therapeutic strategies of neuropathic pain in NMOSD and MS patients are warranted.
Previous studies have found that the age at onset and the attack severity were higher in NMOSD patients than in MS patients.4 In the present study we matched the durations of the two diseases, since neuropathic pain may be influenced by a longer disease duration. Consequently, age and disability status were inevitably higher in the NMOSD group than in the MS group, and neuropathic pain in NMOSD patients might have been influenced by these factors to some extent. Additionally, methodological limitations in the present study associated with the recruitment of NMOSD and MS patients from referral centers may have resulted in unintentional selection bias. Future investigations are needed that include stratification analyses of different age and disability groups in larger cohorts.
In conclusion, the neuropathic pain was more severe and interfered to a greater extent in daily life in NMOSD patients than in MS patients. Physicians should have a comprehensive understanding of the differences in the characteristics of neuropathic pain between NMOSD and MS patients, and such characteristics may provide a basis for the individualized analgesic management of neuropathic pain in these patients.



 XML Download
XML Download